Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Prabhu 2015Dokumen5 halamanPrabhu 2015entannabilakasdyBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- School Guidance Program - FinalDokumen4 halamanSchool Guidance Program - FinalLoreto C. Morales82% (11)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- 2 CP Bekam Angin Tahap 3Dokumen8 halaman2 CP Bekam Angin Tahap 3Norhissam MustafaBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- 2ton Steel 56.8gDokumen4 halaman2ton Steel 56.8gYasir AzmatBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Amit Tracheostomy Presentation 12 Aug 2010Dokumen59 halamanAmit Tracheostomy Presentation 12 Aug 2010Amit KochetaBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Wilhelm Reich Contact With SpaceDokumen6 halamanWilhelm Reich Contact With Spacebubbaclem100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Jurnal Ebm PDFDokumen10 halamanJurnal Ebm PDFagustin488Belum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Pelepasan Polimer LangerDokumen7 halamanPelepasan Polimer LangerUntia Kartika Sari RamadhaniBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- DisputationDokumen8 halamanDisputationsofiaBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Ganglia: The Blackburn Foot and Ankle HyperbookDokumen3 halamanGanglia: The Blackburn Foot and Ankle Hyperbooksiddig7Belum ada peringkat
- Greys - anatomy.S02E25. 17 Seconds - SRTDokumen55 halamanGreys - anatomy.S02E25. 17 Seconds - SRTYing Xuan EngBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A 10-Point Plan For Avoiding Hyaluronic Acid Dermal Filler-Related Complications During Facial Aesthetic Procedures and Algorithms For ManagementDokumen9 halamanA 10-Point Plan For Avoiding Hyaluronic Acid Dermal Filler-Related Complications During Facial Aesthetic Procedures and Algorithms For Managementleenatalia93100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- RSP Eit Booklet 9066788 en 2Dokumen152 halamanRSP Eit Booklet 9066788 en 2Panji NursetiaBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Dayan Aka Wild-Goose - Qigong IntroducionDokumen2 halamanDayan Aka Wild-Goose - Qigong IntroducionTest4D100% (1)
- Emergency in Respiratory MedicineDokumen73 halamanEmergency in Respiratory MedicineIndra MahaputraBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Nardostachys Jatamansi Improves Learning and Memory in MiceDokumen6 halamanNardostachys Jatamansi Improves Learning and Memory in MiceNayan ChaudhariBelum ada peringkat
- Acceptance and Mindfulness Treatments For Children and Adolescents. A Practitioner's Guide - Greco, L. y Hayes, S.Dokumen249 halamanAcceptance and Mindfulness Treatments For Children and Adolescents. A Practitioner's Guide - Greco, L. y Hayes, S.Antonella María De Jesús Napán Carbajal100% (4)
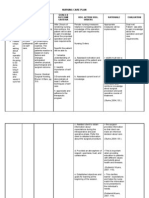
- NCP 1Dokumen4 halamanNCP 1Ke EjieBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Pain Management NCLEXDokumen5 halamanPain Management NCLEXPotchiee PfizerBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Eye and Ear Disorders UpdatedDokumen78 halamanEye and Ear Disorders Updatedjose arreolaBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Bns 209 Module 6 Prevention in Hiv and AidsDokumen12 halamanBns 209 Module 6 Prevention in Hiv and AidslebogangBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Mil DTL 53072CDokumen43 halamanMil DTL 53072CMichael SkrableBelum ada peringkat
- Post Traumatic Stress Disorder PTSD As An Over Activation of Sympathetic Nervous System An Alternative View 2167 1222.1000181Dokumen3 halamanPost Traumatic Stress Disorder PTSD As An Over Activation of Sympathetic Nervous System An Alternative View 2167 1222.1000181Andi ANDIKABelum ada peringkat
- Kyasanur Forest DiseaseDokumen2 halamanKyasanur Forest DiseaseGenoMacaraanBelum ada peringkat
- Leg CellulitisDokumen3 halamanLeg CellulitisJessica Pacris MaramagBelum ada peringkat
- Malaria Control BrochureDokumen2 halamanMalaria Control BrochureEkwoh Okwuchukwu EBelum ada peringkat
- T-Spine MT 1 Review GoodDokumen12 halamanT-Spine MT 1 Review GoodRaymondBelum ada peringkat
- HIS Primary HospitalDokumen7 halamanHIS Primary HospitalJaaaaaaaaazBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Rubella: Congenital Clinically Significant Congenital MalformationsDokumen8 halamanRubella: Congenital Clinically Significant Congenital MalformationsAlexandraBelum ada peringkat
- Pines City Colleges: College of NursingDokumen3 halamanPines City Colleges: College of NursingMara Jon Ocden CasibenBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)