Anda mungkin juga menyukai
- DT ImunisasiDokumen54 halamanDT ImunisasiMar'aturrahmahBelum ada peringkat
- PertusisDokumen28 halamanPertusiswenyinriantoBelum ada peringkat
- Fever and Rash Apcp 260818 FinalDokumen69 halamanFever and Rash Apcp 260818 FinalPriscilla Putri HarmanyBelum ada peringkat
- 15th Indonesian Congress of PediatricsDokumen52 halaman15th Indonesian Congress of PediatricsDody FirmandaBelum ada peringkat
- Program Internship Dokter Indonesia Laporan Mini ProjectDokumen26 halamanProgram Internship Dokter Indonesia Laporan Mini ProjectdeniansaBelum ada peringkat
- Kuliah TuberkulosisDokumen64 halamanKuliah TuberkulosisLeonardBelum ada peringkat
- 0.5 ml IMBooster: 12-15 monthsKIPI: redness , swelling , feverContraindication: history of anaphylaxis tovaccine componentsDokumen47 halaman0.5 ml IMBooster: 12-15 monthsKIPI: redness , swelling , feverContraindication: history of anaphylaxis tovaccine componentsAtika Mayasari PutriBelum ada peringkat
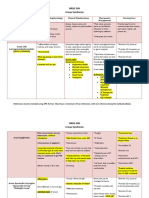
- NRSG 206 Croup SyndromeDokumen3 halamanNRSG 206 Croup SyndromeGirlwithnonameBelum ada peringkat
- MVDBWP VP ZL UP3 L 4 V5 XH G1636761573Dokumen23 halamanMVDBWP VP ZL UP3 L 4 V5 XH G1636761573Ummu muzhaffarBelum ada peringkat
- Kuliah Pengayaan DM 2017-1Dokumen100 halamanKuliah Pengayaan DM 2017-1Syarifah Maharani HidayatBelum ada peringkat
- Tuberkulosis Pada Anak - Prof HedaDokumen50 halamanTuberkulosis Pada Anak - Prof Hedamuhammad ilmanBelum ada peringkat
- Congenital Tuberculosis A Review ArticleDokumen5 halamanCongenital Tuberculosis A Review ArticleMasita RochsalehaBelum ada peringkat
- Dr. Bambang Pujo Semedi, SP An - Antibiotics in Critically Ill E4ED FinalDokumen46 halamanDr. Bambang Pujo Semedi, SP An - Antibiotics in Critically Ill E4ED FinalcittaarunikaBelum ada peringkat
- Sindrom Nefritik DebDokumen2 halamanSindrom Nefritik DebrchristevenBelum ada peringkat
- Hamed2016Dokumen4 halamanHamed2016Franknanda D'enzieroX-zhirawaxaveriuz PutrascreamoDark-nataseBelum ada peringkat
- Curriculum Vitae and Career of Dr. Jeanne Rini PoespoprodjoDokumen23 halamanCurriculum Vitae and Career of Dr. Jeanne Rini PoespoprodjoIBhe Damianry QritezzBelum ada peringkat
- Buku PKB 74 PDFDokumen43 halamanBuku PKB 74 PDFLissaberti AmaliahBelum ada peringkat
- Eczema Finger Tip UnitsDokumen2 halamanEczema Finger Tip UnitsNatasha Natalia100% (1)
- Tatalaksana Malaria Terkini Pada AnakDokumen61 halamanTatalaksana Malaria Terkini Pada Anakretno adijayaBelum ada peringkat
- NBS Law FinalDokumen33 halamanNBS Law Finalkissiah Cajetas100% (1)
- 5 Soal Pilgan EnglishDokumen16 halaman5 Soal Pilgan EnglishAde100% (2)
- Logbook Obeserver E3Dokumen28 halamanLogbook Obeserver E3Ricky PebriansyahBelum ada peringkat
- WHO 2009 Dengue ClassificationDokumen31 halamanWHO 2009 Dengue ClassificationGarata DwiBelum ada peringkat
- LAM-PTKes 0Q00689 Accreditation Certificate for Medical Doctor ProgramDokumen1 halamanLAM-PTKes 0Q00689 Accreditation Certificate for Medical Doctor ProgramMargaret SimmonsBelum ada peringkat
- Fluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversityDokumen61 halamanFluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversitygozaBelum ada peringkat
- Newborn Screening PKB IDAI Papua DR - SandraDokumen39 halamanNewborn Screening PKB IDAI Papua DR - SandraIBhe Damianry QritezzBelum ada peringkat
- Fluid Managementuntuk Mahasiswa SajaDokumen56 halamanFluid Managementuntuk Mahasiswa SajaPratami Rieuwpassa IIBelum ada peringkat
- Aprc BLS PDFDokumen17 halamanAprc BLS PDFNovi BaliBelum ada peringkat
- Strategi Penanganan Gangguan (Speech Delay) Terhadap Interaksi Sosial Anak Usia Dini Di TK Negeri Pembina SurabayaDokumen14 halamanStrategi Penanganan Gangguan (Speech Delay) Terhadap Interaksi Sosial Anak Usia Dini Di TK Negeri Pembina SurabayaRosida WatiBelum ada peringkat
- Konker XVI Conference AnnouncementDokumen16 halamanKonker XVI Conference Announcementyonna anggrelinaBelum ada peringkat
- Leaflet Kelas Ibu BalitaDokumen4 halamanLeaflet Kelas Ibu BalitaUPT Puskesmas Banjarangkan 1Belum ada peringkat
- TB Paru FK UncenDokumen66 halamanTB Paru FK UncenAndira Trianingrum TukanBelum ada peringkat
- Enteral Nutrition of Preterm BabyDokumen54 halamanEnteral Nutrition of Preterm Babylordoftheweb100% (5)
- Rhino PharyngitisDokumen27 halamanRhino PharyngitisinriantoBelum ada peringkat
- Otitis Media AkutDokumen7 halamanOtitis Media AkutghostmanzBelum ada peringkat
- Delivery of TwinsDokumen25 halamanDelivery of TwinsCakraEkkyBelum ada peringkat
- Pneumokokus Dan Penyakit Pneumokokus - Ari PrayitnoDokumen36 halamanPneumokokus Dan Penyakit Pneumokokus - Ari PrayitnoIndri MmrBelum ada peringkat
- Early-Onset Sepsis :clinical and Laboratory ChallengeDokumen34 halamanEarly-Onset Sepsis :clinical and Laboratory ChallengelordofthewebBelum ada peringkat
- Pola Imunologi Janin Dalam Kehamilan Dengan Toxoplasmosis: Khairunnisa Abd Rauf A.Zakaria Amien Octo ZulkarnainDokumen18 halamanPola Imunologi Janin Dalam Kehamilan Dengan Toxoplasmosis: Khairunnisa Abd Rauf A.Zakaria Amien Octo ZulkarnainArdian Zaka RABelum ada peringkat
- DEN GU E: DengueDokumen53 halamanDEN GU E: Denguerose OBelum ada peringkat
- Classification and Management of Feeding Difficulties in Children HO11-004 - E - With - WMDokumen2 halamanClassification and Management of Feeding Difficulties in Children HO11-004 - E - With - WMCarlos GonzalezBelum ada peringkat
- Neonatal Sepsis: A Study of The Risk FactorsDokumen42 halamanNeonatal Sepsis: A Study of The Risk FactorsNithin100% (3)
- Kuliah 3. Pengaturan Osmolalitas UrinDokumen19 halamanKuliah 3. Pengaturan Osmolalitas UrinAnnisa DamayantiBelum ada peringkat
- Obesity in Children: Causes, Symptoms and TreatmentDokumen22 halamanObesity in Children: Causes, Symptoms and TreatmentFitri RahmawatiBelum ada peringkat
- Picu Nicu Yogya April 2015 PDFDokumen18 halamanPicu Nicu Yogya April 2015 PDFIgd Rsim SumberrejoBelum ada peringkat
- Golden OurDokumen89 halamanGolden OurRosmauliana DamanikBelum ada peringkat
- Dr. Nastiti K - Manajemen Asma Pada Anak 2018 PDFDokumen72 halamanDr. Nastiti K - Manajemen Asma Pada Anak 2018 PDFagnesspratiwiBelum ada peringkat
- Konker PeralmunI Malang 2021 Workshop ImunologiDokumen7 halamanKonker PeralmunI Malang 2021 Workshop ImunologiMikyal BulqiahBelum ada peringkat
- Materi OS IDAI Aceh Dr. Dr. Anggraini Alam, Sp.A (K)Dokumen26 halamanMateri OS IDAI Aceh Dr. Dr. Anggraini Alam, Sp.A (K)ajes coolBelum ada peringkat
- Checklist UKMPPD NovemberDokumen6 halamanChecklist UKMPPD Novemberuci marley100% (1)
- Asma BronkialDokumen39 halamanAsma BronkialLidia WatiBelum ada peringkat
- K21-Fever With RashDokumen76 halamanK21-Fever With RashMarisa Perucana SinambelaBelum ada peringkat
- Tinea BarbaeDokumen4 halamanTinea BarbaeKevin EdroBelum ada peringkat
- Skrinning Karsinoma ServiksDokumen33 halamanSkrinning Karsinoma ServiksnowemgfBelum ada peringkat
- Dampak Jangka Panjang StuntingDokumen37 halamanDampak Jangka Panjang StuntingFina GisnawatyBelum ada peringkat
- 03 - DR - Dominicus - PELATIHAN DIFTERI SMD 17 Jan 2018 - Diagnosis - SharedDokumen54 halaman03 - DR - Dominicus - PELATIHAN DIFTERI SMD 17 Jan 2018 - Diagnosis - SharedFebria Valentine AritonangBelum ada peringkat
- Examining The Accuracy of VisualDokumen5 halamanExamining The Accuracy of VisualFarhan HepsandaBelum ada peringkat
- Leflet Asmpid New-3Dokumen1 halamanLeflet Asmpid New-3TheAru21Belum ada peringkat
- RasproDokumen63 halamanRasprofany hertinBelum ada peringkat
- Tetanus Case StudyDokumen4 halamanTetanus Case StudyKervy Jay AgraviadorBelum ada peringkat