Anda mungkin juga menyukai
- Kinesiology ElbowDokumen53 halamanKinesiology Elbowsingle_ladyBelum ada peringkat
- Jurnal Ilmiah Fisioterapi (JIF) Volume 03 Nomor 01 Februari 2020Dokumen6 halamanJurnal Ilmiah Fisioterapi (JIF) Volume 03 Nomor 01 Februari 2020Putri teopani saragihBelum ada peringkat
- Drop Foot Therapy PracticesDokumen3 halamanDrop Foot Therapy PracticesRiina HapsariiBelum ada peringkat
- Development of The Early Activity Scale For EnduranceDokumen1 halamanDevelopment of The Early Activity Scale For EnduranceAsesino GuerreroBelum ada peringkat
- Wrist Joint Anatomy and TestsDokumen38 halamanWrist Joint Anatomy and Testscamy bhagatBelum ada peringkat
- Chest Physio RCT Finds No Benefit in Pediatric PneumoniaDokumen7 halamanChest Physio RCT Finds No Benefit in Pediatric Pneumoniaaufa memeyBelum ada peringkat
- Algoritma LeDokumen1 halamanAlgoritma LerimaBelum ada peringkat
- Short Wave Diathermy Is Defined As The Clinical Application of High Frequency Alternating Current, at A Frequency of 27.12Mhz and Wavelength of 11.06 MeterDokumen1 halamanShort Wave Diathermy Is Defined As The Clinical Application of High Frequency Alternating Current, at A Frequency of 27.12Mhz and Wavelength of 11.06 MeterMohd AsadBelum ada peringkat
- Painful Hemiplegic ShoulderDokumen53 halamanPainful Hemiplegic ShoulderpipitBelum ada peringkat
- Modified Bass TestDokumen7 halamanModified Bass Testchristopher100% (1)
- Journal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDDokumen9 halamanJournal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDWinda FRBelum ada peringkat
- Shoulder Pain and Disability Index SPADI .44Dokumen1 halamanShoulder Pain and Disability Index SPADI .44knikmahBelum ada peringkat
- Tinpus HNPDokumen34 halamanTinpus HNPDimas JanuarBelum ada peringkat
- Microwave Diathermy 2013Dokumen27 halamanMicrowave Diathermy 2013Faisal QureshiBelum ada peringkat
- Frozen Shoulder JurnalDokumen11 halamanFrozen Shoulder JurnalDandy DharmaBelum ada peringkat
- De Quervain SyndromeDokumen5 halamanDe Quervain SyndromePaula ZorziBelum ada peringkat
- Analisis Gerakan Open and Close Kinetic ChainDokumen5 halamanAnalisis Gerakan Open and Close Kinetic ChainAyoe FeratywiBelum ada peringkat
- Matsyasana (Fish Pose) : TechniqueDokumen1 halamanMatsyasana (Fish Pose) : TechniqueKarisma SenapatiBelum ada peringkat
- Sop Muskulo (Tennis Elbow)Dokumen15 halamanSop Muskulo (Tennis Elbow)Melissa Erjani Adam100% (2)
- Penatalaksanaan Fisioterapi Pada LymphedemaDokumen19 halamanPenatalaksanaan Fisioterapi Pada Lymphedemamaevy dwiBelum ada peringkat
- NEUROPATI: KLASIFIKASI DAN PENYEBAB UTAMA LESI SARAF PERIFER</TITLEDokumen126 halamanNEUROPATI: KLASIFIKASI DAN PENYEBAB UTAMA LESI SARAF PERIFER</TITLErismaBelum ada peringkat
- Jurnal CtsDokumen10 halamanJurnal CtsjuanBelum ada peringkat
- Laporan Assesment TMJDokumen21 halamanLaporan Assesment TMJHusnannisa ArifBelum ada peringkat
- Arthrogryposis Congenital ContractureDokumen32 halamanArthrogryposis Congenital ContractureMayesa Akiro100% (1)
- Patologi KardiopulmonalDokumen43 halamanPatologi Kardiopulmonal9661jackBelum ada peringkat
- Twstrs ScalaDokumen2 halamanTwstrs ScalaAlin Lin-LinBelum ada peringkat
- Report on Ankle Sprain AssessmentDokumen11 halamanReport on Ankle Sprain AssessmentGildarts KunBelum ada peringkat
- Efektivitas Peningkatan Aktifitas Fungsional Dengan Intervensi Ice Massage Dan Terapi Latihan Pada Kasus Plantar FasciitisDokumen8 halamanEfektivitas Peningkatan Aktifitas Fungsional Dengan Intervensi Ice Massage Dan Terapi Latihan Pada Kasus Plantar FasciitisTiara PutriBelum ada peringkat
- Fugel MayerDokumen2 halamanFugel MayerRoman AlexandruBelum ada peringkat
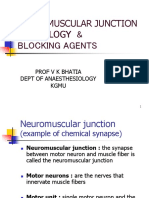
- Neuromuscular Junction Physiology & Blocking Agents: Prof V K Bhatia Dept of Anaesthesiology KgmuDokumen39 halamanNeuromuscular Junction Physiology & Blocking Agents: Prof V K Bhatia Dept of Anaesthesiology KgmuAthira S MadhuBelum ada peringkat
- (Reproduce Freely But Acknowledge Source.) : Abingdon Road, Oxford Oxi 4XdDokumen1 halaman(Reproduce Freely But Acknowledge Source.) : Abingdon Road, Oxford Oxi 4XdBudi RamandaBelum ada peringkat
- Nyeri Pada Tennis Elbow Tipe IIDokumen14 halamanNyeri Pada Tennis Elbow Tipe IIlisaBelum ada peringkat
- Understanding the Underlying Process of Trauma and Its TreatmentDokumen3 halamanUnderstanding the Underlying Process of Trauma and Its TreatmentannyBelum ada peringkat
- Genu Valgus Genu VarusDokumen35 halamanGenu Valgus Genu VarusRatu FaniaBelum ada peringkat
- 02 Naskah PublikasiDokumen15 halaman02 Naskah PublikasiDesbyan candraBelum ada peringkat
- Chondromalacia Patella: Causes, Tests, and Physical Therapy TreatmentsDokumen10 halamanChondromalacia Patella: Causes, Tests, and Physical Therapy TreatmentsAfifah NurBelum ada peringkat
- CV Dr Tirza Z Tamin Rehabilitation ExpertDokumen71 halamanCV Dr Tirza Z Tamin Rehabilitation ExpertAnastasia WibiantoBelum ada peringkat
- Cts Nerve GlidingDokumen10 halamanCts Nerve Glidinganon_259271136Belum ada peringkat
- Pediatric Balance Scale Sixteen Balance TestDokumen8 halamanPediatric Balance Scale Sixteen Balance TestEddy Lanang'e JagadBelum ada peringkat
- Physical Therapy Clinical ManagementDokumen24 halamanPhysical Therapy Clinical ManagementClaudia MicuBelum ada peringkat
- Knee Replacement Exercises - NewDokumen2 halamanKnee Replacement Exercises - NewrBelum ada peringkat
- Effectiveness of Cupping Therapy Versus Myofascial Release (MFR) in Reducing Gastrocnemius Muscle Tightness in High Heels Users - A Comparative StudyDokumen6 halamanEffectiveness of Cupping Therapy Versus Myofascial Release (MFR) in Reducing Gastrocnemius Muscle Tightness in High Heels Users - A Comparative StudyInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- UNDERLYING PROCESS MeniscusDokumen1 halamanUNDERLYING PROCESS MeniscusshafiyahBelum ada peringkat
- Torticollis III BPTDokumen31 halamanTorticollis III BPTKASTURI COLLEGEBelum ada peringkat
- Cubitus Varus Deformity Causes Complications Diagnosis TreatmentDokumen7 halamanCubitus Varus Deformity Causes Complications Diagnosis TreatmentaeruginoBelum ada peringkat
- Low Back Pain: March 2021Dokumen6 halamanLow Back Pain: March 2021sayid najibullahBelum ada peringkat
- Amyotrophic Lateral SclerosisDokumen15 halamanAmyotrophic Lateral SclerosisYakan AbdulrahmanBelum ada peringkat
- Treating Patients With Hemiplegic Shoulder Pain PDFDokumen12 halamanTreating Patients With Hemiplegic Shoulder Pain PDFasdar fajrinBelum ada peringkat
- Capsular pattern identification in idiopathic frozen shoulderDokumen11 halamanCapsular pattern identification in idiopathic frozen shoulderRhany JulyatiBelum ada peringkat
- Upper Cervical Injuries Diagnosis and TreatmentDokumen36 halamanUpper Cervical Injuries Diagnosis and TreatmentesterhsBelum ada peringkat
- Normal Human LocomotionDokumen16 halamanNormal Human LocomotionWendy NgBelum ada peringkat
- Contrast Bath - MKKDokumen10 halamanContrast Bath - MKKKishore KumarBelum ada peringkat
- Stenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandStenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Mckenzie or Williams - Make Your ChoiceDokumen3 halamanMckenzie or Williams - Make Your Choiceemilia gociuBelum ada peringkat
- Williams Flexion Vs McKenzie Extension Exercises Low Back PainDokumen3 halamanWilliams Flexion Vs McKenzie Extension Exercises Low Back PainMasi KhanBelum ada peringkat
- McKenzie Back Extension ExercisesDokumen4 halamanMcKenzie Back Extension ExercisesHitesh KarBelum ada peringkat
- Mckenzie vs. Williams': Protocols For Low Back Pain ManagementDokumen38 halamanMckenzie vs. Williams': Protocols For Low Back Pain ManagementLisa Rosita100% (1)
- McKenzie Vs WilliamsDokumen38 halamanMcKenzie Vs Williamstonhamil100% (2)
- McKenzie - Vs - Williams-Protocols For Low Back Pain ManagementDokumen38 halamanMcKenzie - Vs - Williams-Protocols For Low Back Pain ManagementdjorzaBelum ada peringkat
- Mckenzie Vs William Flexion ExerciseDokumen38 halamanMckenzie Vs William Flexion ExerciseIftinan AmaliaBelum ada peringkat
- 4334 8323 2 PBDokumen7 halaman4334 8323 2 PBlelianaBelum ada peringkat
- Therapeutic ExerciseDokumen32 halamanTherapeutic ExerciseDefaBelum ada peringkat
- Injuries of The Shoulder and KneeDokumen77 halamanInjuries of The Shoulder and KneeDefaBelum ada peringkat
- An Introduction To The Mckenzie Method 1Dokumen24 halamanAn Introduction To The Mckenzie Method 1DefaBelum ada peringkat
- William Vs MC Kenzie-1Dokumen4 halamanWilliam Vs MC Kenzie-1DefaBelum ada peringkat
- Therapeutic ExerciseDokumen32 halamanTherapeutic ExerciseDefaBelum ada peringkat
- William Vs MC Kenzie-1Dokumen4 halamanWilliam Vs MC Kenzie-1DefaBelum ada peringkat
- Concepts of Health, Disease History & TransmissionDokumen25 halamanConcepts of Health, Disease History & TransmissionEASHWARBelum ada peringkat
- Wa0030Dokumen16 halamanWa0030DefaBelum ada peringkat
- AttachmentDokumen61 halamanAttachmentDefaBelum ada peringkat
- Health - Disease AND History of DiseaseDokumen25 halamanHealth - Disease AND History of DiseaseDefaBelum ada peringkat
- William Vs MC Kenzie-1Dokumen4 halamanWilliam Vs MC Kenzie-1DefaBelum ada peringkat
- Aquatic ExerciseDokumen9 halamanAquatic ExerciseDefaBelum ada peringkat
- OTOT KUATDokumen17 halamanOTOT KUATSetyodiartoBelum ada peringkat
- William Flexion ExerciseDokumen22 halamanWilliam Flexion ExerciseDefaBelum ada peringkat
- Osteology Vertebra ServicalDokumen3 halamanOsteology Vertebra ServicalDefaBelum ada peringkat
- Knee Injury and Osteoarthritis Outcome Score Koos PDFDokumen4 halamanKnee Injury and Osteoarthritis Outcome Score Koos PDFNuruel Thamie PoethreeBelum ada peringkat
- Pathway AsmaDokumen21 halamanPathway AsmaYanni Ayii100% (8)
- Contrats BathDokumen5 halamanContrats BathDefaBelum ada peringkat
- Artology Vertebrae ServicalDokumen3 halamanArtology Vertebrae ServicalDefaBelum ada peringkat
- Osteology Vertebra ServicalDokumen3 halamanOsteology Vertebra ServicalDefaBelum ada peringkat
- Theories of ViolenceDokumen20 halamanTheories of ViolenceJanani PrakashBelum ada peringkat
- Practical Role of Nutritional Intervention For Protein Energy - EditDokumen38 halamanPractical Role of Nutritional Intervention For Protein Energy - EditYi KhineBelum ada peringkat
- GSK Case StudyDokumen8 halamanGSK Case StudyAshutosh KhandkarBelum ada peringkat
- EVS CO-4 Study MaterialDokumen26 halamanEVS CO-4 Study Materialprushi703Belum ada peringkat
- Gene RegulationDokumen15 halamanGene RegulationRajendra PrajapatiBelum ada peringkat
- Chronic Renal Failure Nursing Care PlanDokumen6 halamanChronic Renal Failure Nursing Care PlanRuva Oscass JimmyBelum ada peringkat
- Etika Penelitian Pada ManusiaDokumen32 halamanEtika Penelitian Pada ManusiaAhmad NazharBelum ada peringkat
- Fact Sheet: StutteringDokumen2 halamanFact Sheet: StutteringHaley TutwilerBelum ada peringkat
- E NursingDokumen16 halamanE Nursinggopscharan100% (1)
- Recommendations For Physiotherapy Intervention After Stroke 5712Dokumen9 halamanRecommendations For Physiotherapy Intervention After Stroke 5712Anonymous Ezsgg0VSEBelum ada peringkat
- Healthy Eating Plate Guide to Balanced NutritionDokumen4 halamanHealthy Eating Plate Guide to Balanced Nutritionalexkanno100% (1)
- Bone, Joint and Soft TissueDokumen10 halamanBone, Joint and Soft Tissuesarguss14100% (2)
- Sociology of Work - VDokumen239 halamanSociology of Work - VPriyadarsh Ƿđ SarwadeBelum ada peringkat
- DkaDokumen38 halamanDkaHam SotheaBelum ada peringkat
- My Personal Ayurvedic Recipe BookDokumen295 halamanMy Personal Ayurvedic Recipe BookInterfete Diagnoza100% (2)
- Corps School IIIDokumen421 halamanCorps School IIITim Bonine100% (2)
- Four Year Zoology ProgrammeDokumen16 halamanFour Year Zoology ProgrammeAmod KumarBelum ada peringkat
- Bioterrorism and Intelligence PDFDokumen11 halamanBioterrorism and Intelligence PDFIbs Júnior100% (1)
- Miller 2000Dokumen9 halamanMiller 2000BerryEkaPardaBancinBelum ada peringkat
- Vision Research: Stephanie K. Lynch, Michael D. AbràmoffDokumen7 halamanVision Research: Stephanie K. Lynch, Michael D. Abràmoffanka_mihaelaBelum ada peringkat
- Resolution ABKDDokumen2 halamanResolution ABKDBarangay TawidBelum ada peringkat
- Dasar Teori InokulasiDokumen12 halamanDasar Teori InokulasiAmalia Nur azizahBelum ada peringkat
- Carta Gantt .CHEMISTRYF4Dokumen41 halamanCarta Gantt .CHEMISTRYF4Cikgu AnitaBelum ada peringkat
- Acne TreatmentDokumen15 halamanAcne TreatmentSeptia Kurniaty100% (1)
- EUROIMMUN Diagnostic Method For Hypersensitivity in Allergy Reaction FinalDokumen52 halamanEUROIMMUN Diagnostic Method For Hypersensitivity in Allergy Reaction Finalgonteng sadyogaBelum ada peringkat
- Review QuestionsDokumen5 halamanReview Questionsjmkap13Belum ada peringkat
- Hormonal ImbalanceDokumen1 halamanHormonal ImbalanceAWEDIOHEAD100% (9)
- BeckDokumen8 halamanBeck86ionutBelum ada peringkat
- Health 8 Poster MakingDokumen9 halamanHealth 8 Poster MakingDe Leon, Aaron MarcusBelum ada peringkat
- Visa Application Document PDFDokumen18 halamanVisa Application Document PDFUsama NaveedBelum ada peringkat