Anda mungkin juga menyukai
- Acute Medical Emergencies: The Practical ApproachDari EverandAcute Medical Emergencies: The Practical ApproachBelum ada peringkat
- DR - Muhammad Aasam Maan: Consultant Pain SpecialistDokumen23 halamanDR - Muhammad Aasam Maan: Consultant Pain SpecialistMuhammad Aasim MaanBelum ada peringkat
- Manual of Practice Management for Ambulatory Surgery Centers: An Evidence-Based GuideDari EverandManual of Practice Management for Ambulatory Surgery Centers: An Evidence-Based GuideNiraja RajanBelum ada peringkat
- Optimizing Acute Pain Management: A Guide To Multimodal Analgesia and Quality ImprovementDokumen10 halamanOptimizing Acute Pain Management: A Guide To Multimodal Analgesia and Quality ImprovementAgus HendraBelum ada peringkat
- Effect of Postoperative Continuation of Antibiotic Prophylaxis On The Incidence of Surgical Site InfectionDokumen11 halamanEffect of Postoperative Continuation of Antibiotic Prophylaxis On The Incidence of Surgical Site InfectionAde Ewa Permana100% (1)
- Surgical Site Infection PreventionDokumen22 halamanSurgical Site Infection Preventionmed stuBelum ada peringkat
- Surgical Care Improvement Project JCIDokumen50 halamanSurgical Care Improvement Project JCIKania FitrianiBelum ada peringkat
- Perioperative Pain Management Focus On Parecoxib - Eddy Rahardjo SurabayaDokumen42 halamanPerioperative Pain Management Focus On Parecoxib - Eddy Rahardjo SurabayaHammad AjaBelum ada peringkat
- LidocaineDokumen11 halamanLidocaineStanford AnesthesiaBelum ada peringkat
- American College of Surgeons and Surgical Infection Society - Surgical Site Infection Guidelines, 2016 Update (SSI)Dokumen16 halamanAmerican College of Surgeons and Surgical Infection Society - Surgical Site Infection Guidelines, 2016 Update (SSI)Anonymous LnWIBo1GBelum ada peringkat
- Acute Pain Service Handbook: Pain Pathways, Transmission and ModulationDokumen116 halamanAcute Pain Service Handbook: Pain Pathways, Transmission and ModulationdennyramdhanBelum ada peringkat
- Acute Postoperative Pain Manila Relef.Dokumen134 halamanAcute Postoperative Pain Manila Relef.Muchtar Luthfi100% (1)
- Analgesics Chronic PainDokumen36 halamanAnalgesics Chronic PainRobMarvinBelum ada peringkat
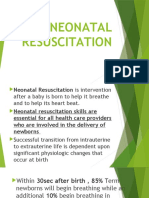
- Neonatal ResuscitationDokumen7 halamanNeonatal ResuscitationJavier López García100% (1)
- Neonatal Resuscitation New GuidelinesDokumen11 halamanNeonatal Resuscitation New GuidelinesJl ABelum ada peringkat
- Guidelines On The Management of Postoperative PainDokumen38 halamanGuidelines On The Management of Postoperative PainIeyna Key Nor Azmina100% (1)
- Prevalence of Surgical Site Infections Among Surgical Operated Patients in Zewditu Memorial Hospital Addis Ababa EthiopiDokumen10 halamanPrevalence of Surgical Site Infections Among Surgical Operated Patients in Zewditu Memorial Hospital Addis Ababa EthiopiAngelo Michilena100% (1)
- NYSORA - The New York School of Regional Anesthesia - Keys To Success With Peripheral Nerve BlocksDokumen13 halamanNYSORA - The New York School of Regional Anesthesia - Keys To Success With Peripheral Nerve BlocksBarbara Sakura Riawan100% (1)
- Surgical InfectionDokumen108 halamanSurgical InfectionAmrit Preet KaurBelum ada peringkat
- Current Trends in Anesthesia For Esophagectomy 2017Dokumen6 halamanCurrent Trends in Anesthesia For Esophagectomy 2017Ajay Varun ReddyBelum ada peringkat
- Guide to Epidural Use in LabourDokumen11 halamanGuide to Epidural Use in LabourcignalBelum ada peringkat
- 5 Reducing Time To Analgesia in The Emergency Department Using ADokumen10 halaman5 Reducing Time To Analgesia in The Emergency Department Using AMegaHandayaniBelum ada peringkat
- Surgical Site Infection PreventionDokumen9 halamanSurgical Site Infection PreventionRachmat HasanBelum ada peringkat
- Higher Risk Surgical Patient 2011 Web PDFDokumen34 halamanHigher Risk Surgical Patient 2011 Web PDFKaren Osorio GilardiBelum ada peringkat
- Bier's BlockDokumen1 halamanBier's BlockAnnie JoBelum ada peringkat
- FCAP Smoking Cessation Clinic Records and ServicesDokumen24 halamanFCAP Smoking Cessation Clinic Records and Servicesmary grace banaBelum ada peringkat
- Postoperative Management in AdultsDokumen58 halamanPostoperative Management in AdultsAjay KumarBelum ada peringkat
- EMS Urology CatalogDokumen41 halamanEMS Urology CatalogIon VasianBelum ada peringkat
- The stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeDokumen287 halamanThe stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeSAJID ALIBelum ada peringkat
- Pain ManagementDokumen7 halamanPain ManagementDenisia HoltBelum ada peringkat
- Standards of Good Practice For Spinal Interventional ProceduresDokumen20 halamanStandards of Good Practice For Spinal Interventional ProceduresMadyline VictoryaBelum ada peringkat
- Skin Grafts PDFDokumen112 halamanSkin Grafts PDFalinutza_childBelum ada peringkat
- General AnasthesiaDokumen7 halamanGeneral AnasthesiaUdunk Adhink0% (1)
- Intrathecal Morphine Single DoseDokumen25 halamanIntrathecal Morphine Single DoseVerghese GeorgeBelum ada peringkat
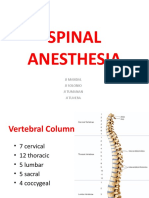
- Spinal Anesthesia: Ji Mandal Ji Solonio Ji Tumanan Ji TuveraDokumen32 halamanSpinal Anesthesia: Ji Mandal Ji Solonio Ji Tumanan Ji TuveraGehlatin TumananBelum ada peringkat
- REVIEW Anesthesia For Thoracic Surgery PDFDokumen22 halamanREVIEW Anesthesia For Thoracic Surgery PDFcristinaBelum ada peringkat
- Acute Service Pain Handbook 2011Dokumen116 halamanAcute Service Pain Handbook 2011Iskandar414Belum ada peringkat
- Anesthesia Free FlapDokumen4 halamanAnesthesia Free FlapSergio ArbelaezBelum ada peringkat
- Endoscopy Department: Graphic Standards Programming and Schematic DesignDokumen25 halamanEndoscopy Department: Graphic Standards Programming and Schematic Designmonir61100% (1)
- Anesthesia For Orthopedic SurgeryDokumen27 halamanAnesthesia For Orthopedic Surgeryjeremy_raineyBelum ada peringkat
- Tibial Plateau FractureDokumen5 halamanTibial Plateau FracturezonadianBelum ada peringkat
- ART 2014 Clinic Report Full PDFDokumen588 halamanART 2014 Clinic Report Full PDFmeltwithsnow163.comBelum ada peringkat
- CCCDokumen487 halamanCCCSlaviša KovačevićBelum ada peringkat
- A Toolkit For Intensive Care UnitsDokumen28 halamanA Toolkit For Intensive Care UnitsekramsBelum ada peringkat
- Eye Care Centre - Best Eye Hospital in India - Shroff Eye CentreDokumen19 halamanEye Care Centre - Best Eye Hospital in India - Shroff Eye CentreShroff Eye Centre - Eye hospitalBelum ada peringkat
- Patient Controlled AnalgesiaDokumen129 halamanPatient Controlled AnalgesiamehranerezvaniBelum ada peringkat
- The Who Emergency Care System Framework and Assessment Tool: The Ethiopian Federal Moh ExperienceDokumen23 halamanThe Who Emergency Care System Framework and Assessment Tool: The Ethiopian Federal Moh ExperienceshoriatBelum ada peringkat
- DEVELOPING PHYSIOTHERAPY LED SHOULDER CLINICS: A PROPOSAL TO ADJUST SCOPE OF PRACTICE BY TENDAYI MUTSOPOTSI Bsc. HPT (Hons) MSc. ORTHO-MEDDokumen15 halamanDEVELOPING PHYSIOTHERAPY LED SHOULDER CLINICS: A PROPOSAL TO ADJUST SCOPE OF PRACTICE BY TENDAYI MUTSOPOTSI Bsc. HPT (Hons) MSc. ORTHO-MEDPhysiotherapy Care SpecialistsBelum ada peringkat
- 2020 Gaumard CatalogDokumen252 halaman2020 Gaumard Catalogjuan javier apazaBelum ada peringkat
- Truspected Stroke AlgorithmDokumen4 halamanTruspected Stroke Algorithmtri wahyunoBelum ada peringkat
- Bob Peripheral Nerve Blocks AspanDokumen70 halamanBob Peripheral Nerve Blocks AspanPrunaru BogdanBelum ada peringkat
- General Anaesthesia: Anaesthesia and Critical Care DeptDokumen46 halamanGeneral Anaesthesia: Anaesthesia and Critical Care DeptAnonymous A2d5hUNeMiBelum ada peringkat
- Gautam Das Clinical ExaminationDokumen233 halamanGautam Das Clinical ExaminationHenry SugihartoBelum ada peringkat
- Anesthesiology Table of Contents 2018 PDFDokumen822 halamanAnesthesiology Table of Contents 2018 PDFRaul ForjanBelum ada peringkat
- Preprocedure Check-In Sign-In Time-Out Sign-OutDokumen2 halamanPreprocedure Check-In Sign-In Time-Out Sign-OutSyahri DzikriBelum ada peringkat
- Chronic Pain SAQ'sDokumen52 halamanChronic Pain SAQ'sNaser AhmedBelum ada peringkat
- Job DescriptionDokumen10 halamanJob Descriptionpioneer92Belum ada peringkat
- Dr. Budwig - Original Cancer ProgramDokumen102 halamanDr. Budwig - Original Cancer Programirfan ahmedBelum ada peringkat
- Dr. Arlene Jane Sy-Reodica Clinical Applications Specialist - ASEAN Monitoring SolutionsDokumen43 halamanDr. Arlene Jane Sy-Reodica Clinical Applications Specialist - ASEAN Monitoring SolutionsArBelum ada peringkat
- ED and Attachment, A Contemporary Psychodynamic PerspectiveDokumen21 halamanED and Attachment, A Contemporary Psychodynamic Perspectiveanindya2293Belum ada peringkat
- A Substance Called Food: Long-Term Psychodynamic Group Treatment For Compulsive OvereatingDokumen25 halamanA Substance Called Food: Long-Term Psychodynamic Group Treatment For Compulsive Overeatinganindya2293Belum ada peringkat
- Psychological Interventions For Adults Who Are Overweight or Obese (Protocol)Dokumen23 halamanPsychological Interventions For Adults Who Are Overweight or Obese (Protocol)anindya2293Belum ada peringkat
- A Substance Called Food: Long-Term Psychodynamic Group Treatment For Compulsive OvereatingDokumen25 halamanA Substance Called Food: Long-Term Psychodynamic Group Treatment For Compulsive Overeatinganindya2293Belum ada peringkat
- Are Atopy and Eosinophilic Bronchial Inflammation Associated With Relapsing Forms of Chronic Rhinosinusitis With Nasal PolypsDokumen6 halamanAre Atopy and Eosinophilic Bronchial Inflammation Associated With Relapsing Forms of Chronic Rhinosinusitis With Nasal Polypsanindya2293Belum ada peringkat
- Doping in SportsDokumen9 halamanDoping in Sportsursvenki4ever3793Belum ada peringkat
- Bmet 262 Outline 2022 2023Dokumen12 halamanBmet 262 Outline 2022 2023Emmanuel PrahBelum ada peringkat
- ECRI Hemodialysis UnitsDokumen24 halamanECRI Hemodialysis Unitsgimen100% (1)
- Management of HydrocephalusDokumen4 halamanManagement of HydrocephalusShine CharityBelum ada peringkat
- 4 Daftar PustakaDokumen3 halaman4 Daftar PustakaDian ApriyaniBelum ada peringkat
- Gastrointestinal System Ppt.-NewDokumen117 halamanGastrointestinal System Ppt.-NewFatima Syed100% (3)
- Huckstep Nail For Periimplant FractureDokumen3 halamanHuckstep Nail For Periimplant FracturePurushothama Rao NalamatiBelum ada peringkat
- Types of PsychologyDokumen62 halamanTypes of PsychologyParamjit SharmaBelum ada peringkat
- Q-MED ADRENALINE INJECTION 1 MG - 1 ML PDFDokumen2 halamanQ-MED ADRENALINE INJECTION 1 MG - 1 ML PDFchannalingeshaBelum ada peringkat
- 04.retrievable Metal Ceramic Implant-Supported Fixed ProsthesesDokumen9 halaman04.retrievable Metal Ceramic Implant-Supported Fixed Prostheses친절Belum ada peringkat
- Stress Management in StudentsDokumen25 halamanStress Management in StudentsJangBelum ada peringkat
- RSOP Pneumatic TourniquetsDokumen10 halamanRSOP Pneumatic Tourniquetsdr_hafizBelum ada peringkat
- Practicing The A, B, C'S: Albert Ellis and REBTDokumen24 halamanPracticing The A, B, C'S: Albert Ellis and REBTShareenjitKaurBelum ada peringkat
- Myopia ManualDokumen337 halamanMyopia ManualRealPurgatory100% (1)
- Case Report in Psychiatry051.03Dokumen4 halamanCase Report in Psychiatry051.03Christian Tan Getana100% (1)
- Leptin HormoneDokumen21 halamanLeptin Hormonemarah almahameed100% (2)
- AgeLOC R Squared Product and Science PresentationDokumen27 halamanAgeLOC R Squared Product and Science PresentationSiaw Sing OngBelum ada peringkat
- MEDUMAT Standard 2 83700-ENDokumen16 halamanMEDUMAT Standard 2 83700-ENJagath PrasangaBelum ada peringkat
- Analgezia Si Anestezia in Obstetrica. Analgezia IN Travaliu: IndicatiiDokumen31 halamanAnalgezia Si Anestezia in Obstetrica. Analgezia IN Travaliu: IndicatiiAlex GrigoreBelum ada peringkat
- Unit 2: Supportive Psychotherapy: A Basic Technique?Dokumen11 halamanUnit 2: Supportive Psychotherapy: A Basic Technique?Luz TanBelum ada peringkat
- Paediatric Protocols 4th Edition (MPA Version) 2nd Print Aug 2019Dokumen686 halamanPaediatric Protocols 4th Edition (MPA Version) 2nd Print Aug 2019kibbitBelum ada peringkat
- Primarily Obsessional OCDDokumen5 halamanPrimarily Obsessional OCDRalphie_Ball100% (2)
- Critical AppraisalDokumen132 halamanCritical AppraisalSanditia Gumilang100% (2)
- Congenital Syphilis Causes and TreatmentDokumen4 halamanCongenital Syphilis Causes and TreatmentAlya Putri Khairani100% (1)
- Case Nephrotic SyndromeDokumen32 halamanCase Nephrotic SyndromeTera SurbaktiBelum ada peringkat
- Lecture 9 - POCT Blood GlucoseDokumen43 halamanLecture 9 - POCT Blood GlucoseRama ArdianaBelum ada peringkat
- Cataract: Presented By: HomipalDokumen12 halamanCataract: Presented By: Homipalankita singhBelum ada peringkat
- Country Presentation: CambodiaDokumen11 halamanCountry Presentation: CambodiaADBI Events100% (1)
- Hemoroid Interna Grade IV: By: Khairunnis A G1A21801 1Dokumen34 halamanHemoroid Interna Grade IV: By: Khairunnis A G1A21801 1Bella ReynaldiBelum ada peringkat
- Kher 2017Dokumen39 halamanKher 2017Evelyn LimBelum ada peringkat
- Easyway Express: Stop Smoking and Quit E-CigarettesDari EverandEasyway Express: Stop Smoking and Quit E-CigarettesPenilaian: 5 dari 5 bintang5/5 (15)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductDari EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductPenilaian: 5 dari 5 bintang5/5 (31)
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildDari EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildPenilaian: 3.5 dari 5 bintang3.5/5 (9)
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryDari EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryBelum ada peringkat
- Drunk-ish: A Memoir of Loving and Leaving AlcoholDari EverandDrunk-ish: A Memoir of Loving and Leaving AlcoholPenilaian: 4 dari 5 bintang4/5 (6)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsDari EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsBelum ada peringkat
- Breathing Under Water: Spirituality and the Twelve StepsDari EverandBreathing Under Water: Spirituality and the Twelve StepsPenilaian: 4.5 dari 5 bintang4.5/5 (41)
- Summary of Gary Wilson's Your Brain on PornDari EverandSummary of Gary Wilson's Your Brain on PornPenilaian: 5 dari 5 bintang5/5 (1)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousDari EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousPenilaian: 5 dari 5 bintang5/5 (22)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionDari EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionPenilaian: 5 dari 5 bintang5/5 (63)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionDari EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionPenilaian: 5 dari 5 bintang5/5 (11)
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Dari EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Penilaian: 4 dari 5 bintang4/5 (7)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingDari EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingPenilaian: 5 dari 5 bintang5/5 (11)
- Mommy Doesn't Drink Here Anymore: Getting Through the First Year of SobrietyDari EverandMommy Doesn't Drink Here Anymore: Getting Through the First Year of SobrietyPenilaian: 4.5 dari 5 bintang4.5/5 (17)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerDari EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerPenilaian: 5 dari 5 bintang5/5 (8)
- Total Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDDari EverandTotal Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDPenilaian: 4 dari 5 bintang4/5 (8)
- The Art of Self-Therapy: How to Grow, Gain Self-Awareness, and Understand Your EmotionsDari EverandThe Art of Self-Therapy: How to Grow, Gain Self-Awareness, and Understand Your EmotionsPenilaian: 5 dari 5 bintang5/5 (1)
- We Are the Luckiest: The Surprising Magic of a Sober LifeDari EverandWe Are the Luckiest: The Surprising Magic of a Sober LifePenilaian: 5 dari 5 bintang5/5 (183)
- Stop Drinking Now: The original Easyway methodDari EverandStop Drinking Now: The original Easyway methodPenilaian: 5 dari 5 bintang5/5 (28)
- The Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingDari EverandThe Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingPenilaian: 5 dari 5 bintang5/5 (10)
- Clean: Overcoming Addiction and Ending America's Greatest TragedyDari EverandClean: Overcoming Addiction and Ending America's Greatest TragedyPenilaian: 3.5 dari 5 bintang3.5/5 (13)
- Drop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)Dari EverandDrop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)Penilaian: 4.5 dari 5 bintang4.5/5 (52)