Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Week 6Dokumen20 halamanWeek 6Julian Lee BermioBelum ada peringkat
- Multivessel Pci Nejm - AppendixDokumen47 halamanMultivessel Pci Nejm - Appendixmajeid saidBelum ada peringkat
- 2023 Heart Failure With Preserved Ejection Fraction-JACC Scientific StatementDokumen25 halaman2023 Heart Failure With Preserved Ejection Fraction-JACC Scientific Statementdian lestariBelum ada peringkat
- A Level 2016 Specimen Paper 2Dokumen14 halamanA Level 2016 Specimen Paper 2Lola BeeBelum ada peringkat
- Atrial Septal DefectDokumen4 halamanAtrial Septal DefectDimpal ChoudharyBelum ada peringkat
- HBP ReportDokumen2 halamanHBP ReportMindi May AguilarBelum ada peringkat
- Science Nat Parallel Test2Dokumen11 halamanScience Nat Parallel Test2Kristine BarredoBelum ada peringkat
- 2nd Periodical Test in Science 6Dokumen6 halaman2nd Periodical Test in Science 6Jonniza AlbitBelum ada peringkat
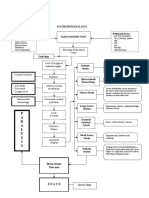
- Pathophysiology: P A R A L Y S I SDokumen1 halamanPathophysiology: P A R A L Y S I SJordan Garcia AguilarBelum ada peringkat
- 26 Pycnogenol EbookDokumen36 halaman26 Pycnogenol EbookPredrag TerzicBelum ada peringkat
- Sample PrognosisDokumen3 halamanSample PrognosisjudssalangsangBelum ada peringkat
- Electrophysiological Maneuvers For Arrhythmia Analysis-Cardiotext Publishing (2014)Dokumen211 halamanElectrophysiological Maneuvers For Arrhythmia Analysis-Cardiotext Publishing (2014)Ali Uğur Soysal100% (1)
- Cad AsimtomatikDokumen24 halamanCad AsimtomatikAditya Arya PutraBelum ada peringkat
- Cardiovascular System Integrated Teaching ModuleDokumen2 halamanCardiovascular System Integrated Teaching ModuleShivan UmamaheswaranBelum ada peringkat
- Heart MudraDokumen4 halamanHeart MudracpschungathBelum ada peringkat
- ThrombosisDokumen11 halamanThrombosisNobby Onist JuniorBelum ada peringkat
- Q32.Heart Development, Anatomy, Topography, Function. Valves and Fibrous Skeleton of The HeartDokumen10 halamanQ32.Heart Development, Anatomy, Topography, Function. Valves and Fibrous Skeleton of The HeartMohammed RamzyBelum ada peringkat
- Mechanism of Lymph Node Metastasis in Prostate CancerDokumen20 halamanMechanism of Lymph Node Metastasis in Prostate CancerAlexBritoBelum ada peringkat
- T4 Vocabulary Activity 2 - 7 (Human Body)Dokumen6 halamanT4 Vocabulary Activity 2 - 7 (Human Body)Aprilia Salsabilla DindaBelum ada peringkat
- Med 1 Block 2 - Wet Lab NotesDokumen36 halamanMed 1 Block 2 - Wet Lab NotesluckyBelum ada peringkat
- EmbryologyDokumen1 halamanEmbryologyprasannaipad324Belum ada peringkat
- Skeletal SystemsDokumen3 halamanSkeletal Systemsemmanuel richardBelum ada peringkat
- PhyseoDokumen7 halamanPhyseoRabiaNaseemBelum ada peringkat
- Pediatric Cardiology PDFDokumen382 halamanPediatric Cardiology PDFfarzadfusion100% (5)
- p56 - p110Dokumen6 halamanp56 - p110Bhushan D ThombareBelum ada peringkat
- Point-Of-Care Ultrasound in Cardiac ArrestDokumen13 halamanPoint-Of-Care Ultrasound in Cardiac ArrestEgorSazhaevBelum ada peringkat
- Acute Anterior Wall Myocardial InfarctionDokumen2 halamanAcute Anterior Wall Myocardial InfarctionMelinda Cariño BallonBelum ada peringkat
- Heart and Breath SoundsDokumen9 halamanHeart and Breath Soundszeglam0% (1)
- Tao of Revitalization: Exercises For Self-HealingDokumen25 halamanTao of Revitalization: Exercises For Self-HealingAnirudh100% (1)
- Angiography 50%Dokumen17 halamanAngiography 50%Nova SipahutarBelum ada peringkat