Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- NCP Difficulties in BreathingDokumen4 halamanNCP Difficulties in BreathingKingJayson Pacman06Belum ada peringkat
- NURS FPX 6021 Assessment 1 Concept MapDokumen7 halamanNURS FPX 6021 Assessment 1 Concept MapEmma WatsonBelum ada peringkat
- Spesifikasi Evita V800 AdvanceDokumen3 halamanSpesifikasi Evita V800 AdvancemurifuBelum ada peringkat
- Respiratory Distress and CPAP: Maternity and Neonatal Clinical GuidelineDokumen32 halamanRespiratory Distress and CPAP: Maternity and Neonatal Clinical GuidelinePediatri UnsratBelum ada peringkat
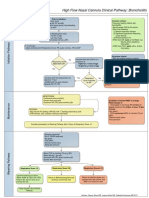
- High Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion CriteriaDokumen1 halamanHigh Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion Criteriad'Agung NugrohoBelum ada peringkat
- Bear Cub 750 - Quick User GuideDokumen2 halamanBear Cub 750 - Quick User GuideSn DayanidhiBelum ada peringkat
- ArdsDokumen7 halamanArdsIpar DayBelum ada peringkat
- Pulmonary PathoPhysiologyDokumen45 halamanPulmonary PathoPhysiologySuliman Garalleh100% (1)
- Respiratory System DisordersDokumen115 halamanRespiratory System DisordersFaith Levi Alecha Alferez100% (1)
- NebulizationDokumen4 halamanNebulizationleoBelum ada peringkat
- Thorax and Lungs: Chapter EighteenDokumen12 halamanThorax and Lungs: Chapter Eighteengrool29r67% (3)
- HH2 Pediatric Asthma Case StudyDokumen3 halamanHH2 Pediatric Asthma Case Studyshazel chiasaokwuBelum ada peringkat
- NCPDokumen4 halamanNCPMark Benedict Ocampo VelardeBelum ada peringkat
- NCP-Airway ClearanceDokumen2 halamanNCP-Airway ClearanceTimi BCBelum ada peringkat
- AtelektasisDokumen10 halamanAtelektasisSaputri AnggiBelum ada peringkat
- A Male Adult Patient Hospitalized For Treatment of A Pulmonary Embolism Develops Respiratory AlkalosisDokumen4 halamanA Male Adult Patient Hospitalized For Treatment of A Pulmonary Embolism Develops Respiratory AlkalosisCezanne CruzBelum ada peringkat
- First Announcement Pdpi Update 1Dokumen25 halamanFirst Announcement Pdpi Update 1sheeno2607Belum ada peringkat
- Congenital Laryngomalacia Is Related To Exercise-Induced Laryngeal Obstruction in Adolescence - Archdischild-2015.fullDokumen7 halamanCongenital Laryngomalacia Is Related To Exercise-Induced Laryngeal Obstruction in Adolescence - Archdischild-2015.fullwawa chenBelum ada peringkat
- M 371Dokumen14 halamanM 371Anonymous h0DxuJTBelum ada peringkat
- Lung AuscultogramDokumen1 halamanLung AuscultogramJacklyn M. oBelum ada peringkat
- Demo Request Form - ECOBAG - PSADokumen12 halamanDemo Request Form - ECOBAG - PSAAllyssa BuenaventuraBelum ada peringkat
- CpapDokumen33 halamanCpapAtikah Putri AtmojoBelum ada peringkat
- Greek BTSDokumen51 halamanGreek BTSIrene Chrysovalanto ThemistocleousBelum ada peringkat
- Lesson Exemplar Health10 Luna San JuanDokumen14 halamanLesson Exemplar Health10 Luna San JuanGiezelle LeopandoBelum ada peringkat
- Non-Invasive Ventilation of The NeonateDokumen21 halamanNon-Invasive Ventilation of The NeonatesiputamaliaputriBelum ada peringkat
- Mechanical Ventilation in ChildrenDokumen74 halamanMechanical Ventilation in ChildrenBhawna PandhuBelum ada peringkat
- iHope RV Series Ventilator DatasheetDokumen2 halamaniHope RV Series Ventilator DatasheetNoe Muñoz QuitoBelum ada peringkat
- Respiratory Care: by Armstrong MedicalDokumen2 halamanRespiratory Care: by Armstrong MedicalYessenia CiezaBelum ada peringkat
- Chronic Obstructive Pulmonary Disease: A Case Presentation OnDokumen95 halamanChronic Obstructive Pulmonary Disease: A Case Presentation OnJunery Bagunas100% (2)
- Basics of Mechanical VentilationDokumen63 halamanBasics of Mechanical VentilationDiem KhueBelum ada peringkat