Anda mungkin juga menyukai
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- DFFGGGDokumen1 halamanDFFGGGayuBelum ada peringkat
- Asal Usul Burung CenderawasihDokumen11 halamanAsal Usul Burung CenderawasihayuBelum ada peringkat
- Personal PDF File For H. C. Fayaz, J. B. Jupiter: Galeazzi Fractures: Our Modified Classification and Treatment RegimenDokumen4 halamanPersonal PDF File For H. C. Fayaz, J. B. Jupiter: Galeazzi Fractures: Our Modified Classification and Treatment RegimenayuBelum ada peringkat
- Personal PDF File For H. C. Fayaz, J. B. Jupiter: Galeazzi Fractures: Our Modified Classification and Treatment RegimenDokumen4 halamanPersonal PDF File For H. C. Fayaz, J. B. Jupiter: Galeazzi Fractures: Our Modified Classification and Treatment RegimenayuBelum ada peringkat
- Galeazzi Fractures: Our Modified Classification and Treatment RegimenDokumen5 halamanGaleazzi Fractures: Our Modified Classification and Treatment RegimenayuBelum ada peringkat
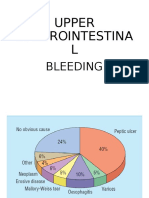
- Upper Gastrointestina L: BleedingDokumen35 halamanUpper Gastrointestina L: BleedingayuBelum ada peringkat
- Asal Usul Burung CenderawasihDokumen11 halamanAsal Usul Burung CenderawasihayuBelum ada peringkat
- DFFGGGDokumen1 halamanDFFGGGayuBelum ada peringkat
- The Pathogenesis of Fever: Kathryn M. Edwards, MDDokumen54 halamanThe Pathogenesis of Fever: Kathryn M. Edwards, MDayuBelum ada peringkat
- Lower GI Bleeding Causes, Symptoms, and TreatmentDokumen32 halamanLower GI Bleeding Causes, Symptoms, and TreatmentayuBelum ada peringkat
- Approach To Jaundice (1) .PPT ALAWAJIDokumen28 halamanApproach To Jaundice (1) .PPT ALAWAJIayuBelum ada peringkat
- LeptospirosisDokumen22 halamanLeptospirosisayuBelum ada peringkat
- Gastroenteritis: - Inflammation of Stomach or IntestinesDokumen31 halamanGastroenteritis: - Inflammation of Stomach or IntestinesayuBelum ada peringkat
- HDokumen33 halamanHayuBelum ada peringkat
- Penyakit CacingDokumen17 halamanPenyakit CacingayuBelum ada peringkat
- Perlemakan HatiDokumen42 halamanPerlemakan HatiayuBelum ada peringkat
- Penyakit CacingDokumen17 halamanPenyakit CacingayuBelum ada peringkat
- Defisiensi VitaminDokumen30 halamanDefisiensi VitaminayuBelum ada peringkat
- Gastroenteritis: - Inflammation of Stomach or IntestinesDokumen31 halamanGastroenteritis: - Inflammation of Stomach or IntestinesayuBelum ada peringkat
- Perlemakan HatiDokumen42 halamanPerlemakan HatiayuBelum ada peringkat
- Defisiensi VitaminDokumen30 halamanDefisiensi VitaminayuBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Clinical Anatomy of the Hand: A Guide for SurgeonsDokumen54 halamanClinical Anatomy of the Hand: A Guide for Surgeonsmarikos82Belum ada peringkat
- Bones Flash CardDokumen22 halamanBones Flash CardMiki AberaBelum ada peringkat
- TX of Colles FXDokumen4 halamanTX of Colles FXJessica CaronBelum ada peringkat
- Fracture Treatment ProtocolsDokumen14 halamanFracture Treatment ProtocolsZikrul IdyaBelum ada peringkat
- Elbow Special TestDokumen4 halamanElbow Special TestEllaiza Astacaan100% (1)
- Hand and Wrist AAOs 2019 PDFDokumen70 halamanHand and Wrist AAOs 2019 PDFYusuf RizalBelum ada peringkat
- Principles of Tendon Transfer in The Hand and ForearmDokumen9 halamanPrinciples of Tendon Transfer in The Hand and Forearm'Ema Surya PertiwiBelum ada peringkat
- Forearm Fracture Types and TreatmentsDokumen21 halamanForearm Fracture Types and TreatmentsAbdullah MatarBelum ada peringkat
- AXEL ElectrodPlacement Manual V11Dokumen28 halamanAXEL ElectrodPlacement Manual V11leung_ting_2Belum ada peringkat
- Muscles of Hand & WristDokumen43 halamanMuscles of Hand & WristWasemBhatBelum ada peringkat
- Univ of Michigan - Gross Anatomy - Muscles Tables PDFDokumen39 halamanUniv of Michigan - Gross Anatomy - Muscles Tables PDFsabrina aswanBelum ada peringkat
- Chapter 08 MusculoskeletalDokumen5 halamanChapter 08 MusculoskeletalBernard Paul GuintoBelum ada peringkat
- Bpes2 SemDokumen95 halamanBpes2 Semnishthabanga1525Belum ada peringkat
- Atlas Hand Clin Volume 8 Issue 1 March 2003 - Scaphoid InjuriesDokumen189 halamanAtlas Hand Clin Volume 8 Issue 1 March 2003 - Scaphoid InjuriesМарина Катькалова100% (1)
- Solution Manual For Human Anatomy Laboratory Manual With Cat Dissections 7 e 7th EditionDokumen11 halamanSolution Manual For Human Anatomy Laboratory Manual With Cat Dissections 7 e 7th EditionJamesThomasngec100% (42)
- Ar PDFDokumen26 halamanAr PDFBárbara Romero OlateBelum ada peringkat
- Finger Force Capability - 10.1.1.498.673Dokumen103 halamanFinger Force Capability - 10.1.1.498.673Sidney M. SilvaBelum ada peringkat
- The Musculoskeletal SystemDokumen173 halamanThe Musculoskeletal SystemSupratik Chakraborty100% (1)
- Clinical Case 1 Muscular SystemDokumen8 halamanClinical Case 1 Muscular SystemKier Nikki RualBelum ada peringkat
- OIA of Cat MusclesDokumen8 halamanOIA of Cat Musclesksdfsd8903Belum ada peringkat
- Extract Pages From 373422607-1-Print-Microsystems-AcupunctureDokumen11 halamanExtract Pages From 373422607-1-Print-Microsystems-AcupunctureHenrique CaldasBelum ada peringkat
- Upper LimbDokumen48 halamanUpper LimbPrince XavierBelum ada peringkat
- Annotate VR HandsDokumen16 halamanAnnotate VR Handsrandy andresBelum ada peringkat
- The Skeletal System Human Body (206) Axial Skeleton (80) Skull (28) A. Paired Bones (11x2 22)Dokumen17 halamanThe Skeletal System Human Body (206) Axial Skeleton (80) Skull (28) A. Paired Bones (11x2 22)Leo Cordel Jr.Belum ada peringkat
- Blandino We0413Dokumen25 halamanBlandino We0413RohitOkeBelum ada peringkat
- Orthopaedic Intruments and Surgeries: DR Tejasvi Agarwal Senior Resident Dept of OrthopaedicsDokumen43 halamanOrthopaedic Intruments and Surgeries: DR Tejasvi Agarwal Senior Resident Dept of OrthopaedicsKapil LakhwaraBelum ada peringkat
- 10 AnatomyApproaches Orthobullets2017Dokumen177 halaman10 AnatomyApproaches Orthobullets2017jazelBelum ada peringkat
- Bednar MS, James MA, Light TR. Congenital Longitudinal Deficiency. J Hand Surg Am. 2009Dokumen9 halamanBednar MS, James MA, Light TR. Congenital Longitudinal Deficiency. J Hand Surg Am. 2009AsdfBelum ada peringkat
- Mallet AnatomyDokumen277 halamanMallet AnatomyJethro Rola SiguaBelum ada peringkat
- Gross Anatomy CheatsheetDokumen302 halamanGross Anatomy CheatsheetNobody2015100% (1)