Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Proteins in Serum & UrineDokumen66 halamanProteins in Serum & Urinekiedd_04100% (1)
- Corticosteroids: Ghadi Mahmoud Elbarghathi Roll Number: 1950 5 Year 2021-2022Dokumen26 halamanCorticosteroids: Ghadi Mahmoud Elbarghathi Roll Number: 1950 5 Year 2021-2022Ghadi ElbarghathiBelum ada peringkat
- Knowing Ourselves: What Does The Body Want To Tell Us With Diseases? MR Joman Romero LopezDokumen582 halamanKnowing Ourselves: What Does The Body Want To Tell Us With Diseases? MR Joman Romero LopezKsenija Medic100% (1)
- Acute Care Surgery Handbook: General Aspects, Non-Gastrointestinai and Critical Care EmergenciesDokumen512 halamanAcute Care Surgery Handbook: General Aspects, Non-Gastrointestinai and Critical Care EmergenciesOscar Villacres100% (6)
- Topical Diagnosis: Department of Anatomy Medical Faculty, Hasanuddin UniversityDokumen48 halamanTopical Diagnosis: Department of Anatomy Medical Faculty, Hasanuddin UniversityRey Alwiwikh100% (1)
- KDIGO GD Guideline Key Takeaways For Clinicians Lupus NephritisDokumen1 halamanKDIGO GD Guideline Key Takeaways For Clinicians Lupus Nephritisadamu mohammadBelum ada peringkat
- Introduction To Clinical Medicine MCQ Set ADokumen2 halamanIntroduction To Clinical Medicine MCQ Set AHimanshu Karmacharya100% (9)
- Annals of Surgery Volume Issue 2015 (Doi 10.1097/SLA.0000000000001495) Mentula, Panu Sammalkorpi, Henna Leppäniemi, Ari - Reply To Letter PDFDokumen1 halamanAnnals of Surgery Volume Issue 2015 (Doi 10.1097/SLA.0000000000001495) Mentula, Panu Sammalkorpi, Henna Leppäniemi, Ari - Reply To Letter PDFOscar VillacresBelum ada peringkat
- Annals of Surgery Volume Issue 2015 (Doi 10.1097/sla.0000000000001494) Weber, Dieter G. Di Saverio, Salomone - Letter To The Editor PDFDokumen1 halamanAnnals of Surgery Volume Issue 2015 (Doi 10.1097/sla.0000000000001494) Weber, Dieter G. Di Saverio, Salomone - Letter To The Editor PDFOscar VillacresBelum ada peringkat
- Nonsurgical Treatment of Appendiceal Abscess or Phlegmon: A Systematic Review and Meta-AnalysisDokumen8 halamanNonsurgical Treatment of Appendiceal Abscess or Phlegmon: A Systematic Review and Meta-AnalysisOscar VillacresBelum ada peringkat
- Laparoscopic Surgery or Conservative Treatment For Appendiceal Abscess in Adults?Dokumen6 halamanLaparoscopic Surgery or Conservative Treatment For Appendiceal Abscess in Adults?Oscar VillacresBelum ada peringkat
- Mastery in Bariatric Surgery: The Long-Term Surgeon Learning Curve of Roux-en-Y Gastric BypassDokumen6 halamanMastery in Bariatric Surgery: The Long-Term Surgeon Learning Curve of Roux-en-Y Gastric BypassOscar VillacresBelum ada peringkat
- Mastery in Bariatric Surgery: The Long-Term Surgeon Learning Curve of Roux-en-Y Gastric BypassDokumen6 halamanMastery in Bariatric Surgery: The Long-Term Surgeon Learning Curve of Roux-en-Y Gastric BypassOscar VillacresBelum ada peringkat
- Essentialelementsof Multimodalanalgesiain Enhancedrecoveryafter Surgery (Eras) GuidelinesDokumen29 halamanEssentialelementsof Multimodalanalgesiain Enhancedrecoveryafter Surgery (Eras) GuidelinesOscar VillacresBelum ada peringkat
- Cochrane SCA Sindrome Confusional AgudoDokumen43 halamanCochrane SCA Sindrome Confusional AgudoOscar VillacresBelum ada peringkat
- The Non Operative Treatment For Acute Appendicitis (NOTA) Study: Is Less Surgery Better Surgery?Dokumen1 halamanThe Non Operative Treatment For Acute Appendicitis (NOTA) Study: Is Less Surgery Better Surgery?Oscar VillacresBelum ada peringkat
- Ne en WhippleDokumen9 halamanNe en WhippleOscar VillacresBelum ada peringkat
- CNS DevelopmentDokumen158 halamanCNS DevelopmentMubashir SiyalBelum ada peringkat
- Jangan Di BukaDokumen15 halamanJangan Di BukaNuraga Dwi PratapaBelum ada peringkat
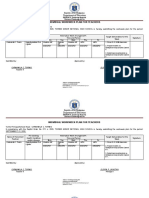
- Individual Workweek Plan For Teachers: Department of EducationDokumen5 halamanIndividual Workweek Plan For Teachers: Department of EducationJestony LubatonBelum ada peringkat
- Case StudyDokumen22 halamanCase StudyBiway RegalaBelum ada peringkat
- Anticholinergic Drugs,: Ganglion Blocking Agents and Neuromuscular Blocking AgentsDokumen26 halamanAnticholinergic Drugs,: Ganglion Blocking Agents and Neuromuscular Blocking AgentsLoai Mohammed IssaBelum ada peringkat
- Obstetric and Gynaecological Nursing IInd YearDokumen8 halamanObstetric and Gynaecological Nursing IInd YearsanthiyasandyBelum ada peringkat
- Katie Is A Teenage Girl Who Suffers From A Rare Disease Called Xeroderma Pigmentosum. HerDokumen4 halamanKatie Is A Teenage Girl Who Suffers From A Rare Disease Called Xeroderma Pigmentosum. HerLyrah ManioBelum ada peringkat
- Inter. J. of Pharmacotherapy / 7(2), 2017, 56-58. Case Study on Dengue Fever with ThrombocytopeniaDokumen3 halamanInter. J. of Pharmacotherapy / 7(2), 2017, 56-58. Case Study on Dengue Fever with ThrombocytopeniaHanna La MadridBelum ada peringkat
- ATLSDokumen34 halamanATLSalice DillerudBelum ada peringkat
- Types of Stroke: Stroke - CVA Cerebral Vascular Accident Ischemic Cerebrovascular DiseaseDokumen7 halamanTypes of Stroke: Stroke - CVA Cerebral Vascular Accident Ischemic Cerebrovascular DiseaseMarrylane GamisBelum ada peringkat
- ICMR Diabetes Guidelines.2018Dokumen70 halamanICMR Diabetes Guidelines.2018A. RaufBelum ada peringkat
- Rumah Sakit Mata ICD X Eng FixDokumen11 halamanRumah Sakit Mata ICD X Eng FixPelayanan MedisBelum ada peringkat
- Alcohols: Merlina L. Cabrera, MDDokumen16 halamanAlcohols: Merlina L. Cabrera, MDMeg AmoonBelum ada peringkat
- Arterial Blood Gas (ABG) Analysis: Normal ValuesDokumen3 halamanArterial Blood Gas (ABG) Analysis: Normal ValuesNayem Hossain HemuBelum ada peringkat
- Kompilasi - ICD MM Dan PM - Reference GuideDokumen93 halamanKompilasi - ICD MM Dan PM - Reference GuidehijraBelum ada peringkat
- Neurological Disease in Lupus: Toward A Personalized Medicine ApproachDokumen12 halamanNeurological Disease in Lupus: Toward A Personalized Medicine ApproachjerejerejereBelum ada peringkat
- Ortho McqsDokumen120 halamanOrtho McqsSyeda Sakina AsgharBelum ada peringkat
- FMGE March 2008 MCQs Hello Everyone, If The Results AreDokumen15 halamanFMGE March 2008 MCQs Hello Everyone, If The Results Arearslansaeed007Belum ada peringkat
- ENT 1.3 Lips and Oral CavityDokumen15 halamanENT 1.3 Lips and Oral CavityZazaBelum ada peringkat
- Assessment Report On Ginkgo Biloba L., Folium DDokumen120 halamanAssessment Report On Ginkgo Biloba L., Folium DMiroslav IlicBelum ada peringkat
- Phlebotomy and Biomedical Waste ManagementDokumen74 halamanPhlebotomy and Biomedical Waste ManagementShivani Yadav0% (1)
- Eucalyptol 1Dokumen10 halamanEucalyptol 1NadiyahBelum ada peringkat
- Important Lists of Helminths: Non-Bile Stained Eggs Operculated Eggs Don't Float in Sat. Salt SolutionDokumen10 halamanImportant Lists of Helminths: Non-Bile Stained Eggs Operculated Eggs Don't Float in Sat. Salt SolutionAjay ShresthaBelum ada peringkat
- Nature Review of The Man Who Wasn't ThereDokumen2 halamanNature Review of The Man Who Wasn't Thereanil.newscientistBelum ada peringkat