Anda mungkin juga menyukai
- Mechanical Asphyxia 1Dokumen86 halamanMechanical Asphyxia 1Piash AnikBelum ada peringkat
- AsphyxiaDokumen122 halamanAsphyxiaAbdul MajidBelum ada peringkat
- Asphyxia and Asphyxial Death: Prepared by Mohidul Islam Mymensingh Medical College Session-2016-2017 (4 Year)Dokumen85 halamanAsphyxia and Asphyxial Death: Prepared by Mohidul Islam Mymensingh Medical College Session-2016-2017 (4 Year)Umme najiajahan50% (2)
- Forensic II - Asphyxia, 2007Dokumen6 halamanForensic II - Asphyxia, 2007Roel PalmairaBelum ada peringkat
- Rigor MortisDokumen2 halamanRigor Mortisapi-238242929Belum ada peringkat
- Violent Asphyxial DeathsDokumen168 halamanViolent Asphyxial Deathsapi-19916399Belum ada peringkat
- Forensic PathologyDokumen3 halamanForensic PathologyjmosserBelum ada peringkat
- Lectures in Forensic MedicineDokumen3 halamanLectures in Forensic MedicinelindagabitBelum ada peringkat
- Death & PM ChangesDokumen125 halamanDeath & PM ChangesPiash AnikBelum ada peringkat
- Cerebrovascular Accident: TypesDokumen10 halamanCerebrovascular Accident: TypesJulia SalvioBelum ada peringkat
- Death& Postmortem ChangesDokumen28 halamanDeath& Postmortem Changeswrashwan27Belum ada peringkat
- Burn Injury: Our Lady of Fatima University College of NursingDokumen21 halamanBurn Injury: Our Lady of Fatima University College of NursingPOTENCIANA MAROMABelum ada peringkat
- Semen AnalysisDokumen9 halamanSemen AnalysisGlydenne Glaire Poncardas GayamBelum ada peringkat
- Skull FractureDokumen13 halamanSkull FractureEddie LimBelum ada peringkat
- Negative AutopsyDokumen21 halamanNegative Autopsydr rizwanBelum ada peringkat
- COPD Lecture Slides For BlackBoardDokumen52 halamanCOPD Lecture Slides For BlackBoardClayton JensenBelum ada peringkat
- Spirometry: Dr. Dora FlorianDokumen15 halamanSpirometry: Dr. Dora FlorianDoraBelum ada peringkat
- 12 White Blood Cell DisordersDokumen16 halaman12 White Blood Cell Disordersndnplaya712Belum ada peringkat
- FingerprintingDokumen36 halamanFingerprintingapi-291003259100% (1)
- Perinatal AsphyxiaDokumen29 halamanPerinatal AsphyxiastmsubashBelum ada peringkat
- Deaths Due To Thermal BurnsDokumen48 halamanDeaths Due To Thermal BurnsSheharyarHassanKhanBelum ada peringkat
- Violent Asphyxial DeathsDokumen188 halamanViolent Asphyxial DeathsARIF-UR-REHMAN86% (14)
- BurnsDokumen1 halamanBurnsasdfghjBelum ada peringkat
- 4 CPCRDokumen35 halaman4 CPCRrika nisfularikaBelum ada peringkat
- Postmortem Changes and Postmortem Time IntervalDokumen24 halamanPostmortem Changes and Postmortem Time IntervalkhadzxBelum ada peringkat
- Empyema 171013100219Dokumen23 halamanEmpyema 171013100219Mahmoud Abdel MoneimBelum ada peringkat
- Sickle Cell DiseaseDokumen23 halamanSickle Cell Diseasealejandrino_leoaugusto100% (1)
- Motor ExaminationDokumen40 halamanMotor ExaminationBinte Muhammad100% (1)
- General Physical ExaminationDokumen18 halamanGeneral Physical ExaminationNick JacobBelum ada peringkat
- Pulmonary Tuberculosis: Presented By: Mis.M.K.Kaku Nursing TutorDokumen16 halamanPulmonary Tuberculosis: Presented By: Mis.M.K.Kaku Nursing TutorKaku ManishaBelum ada peringkat
- 1 - MCCDDokumen26 halaman1 - MCCDAnupam SarkarBelum ada peringkat
- Fluid and Electrolyte 2018-1Dokumen33 halamanFluid and Electrolyte 2018-1EN.BASSAM ALSABAHI100% (1)
- Violent Asphyxial DeathsDokumen188 halamanViolent Asphyxial DeathsEduard TomițaBelum ada peringkat
- Alcohol PoisoningDokumen43 halamanAlcohol PoisoningImteaz ahamadBelum ada peringkat
- Cardiovascular System Diseases Part 1Dokumen22 halamanCardiovascular System Diseases Part 1Prince Rener Velasco PeraBelum ada peringkat
- Pathophysiology of DeathDokumen28 halamanPathophysiology of DeathMuhammad Furqon FahlulyBelum ada peringkat
- Genetics: OLFU - College of MedicineDokumen7 halamanGenetics: OLFU - College of MedicineMiguel CuevasBelum ada peringkat
- Complement SystemDokumen21 halamanComplement SystemEl FatihBelum ada peringkat
- NCM 103 - Oxy RespiDokumen21 halamanNCM 103 - Oxy RespiMaureen Gonzalo-FlorendoBelum ada peringkat
- Blood Pressure-For StudentsDokumen79 halamanBlood Pressure-For StudentsAshok Kumar P100% (1)
- Organophosphate PoisoningDokumen19 halamanOrganophosphate PoisoningapokawBelum ada peringkat
- Organophosphate PoisoningDokumen19 halamanOrganophosphate PoisoningPanda Kuma0% (1)
- Chapter 2 Death and Postmortem ChangesDokumen72 halamanChapter 2 Death and Postmortem ChangesdebbytenriBelum ada peringkat
- Leukaemia: Definition: Leukemia Is A Malignant Disease of The Hematopoietic System (Blood Forming Cells)Dokumen16 halamanLeukaemia: Definition: Leukemia Is A Malignant Disease of The Hematopoietic System (Blood Forming Cells)Arnab Ghosh100% (1)
- Legal MedicineDokumen7 halamanLegal MedicineEric CamposBelum ada peringkat
- Surgery, General, Wounds and Wound HealingDokumen15 halamanSurgery, General, Wounds and Wound HealingRhazes78100% (1)
- Immunoglobulins - Structure and Function Definition: Immunoglobulins (Ig)Dokumen9 halamanImmunoglobulins - Structure and Function Definition: Immunoglobulins (Ig)Valdez Francis ZaccheauBelum ada peringkat
- Why Is A Prothrombin Time Test Performed?: WarfarinDokumen6 halamanWhy Is A Prothrombin Time Test Performed?: WarfarinMamta ShindeBelum ada peringkat
- Genetic Disorder and Genetic Counselling: Ruthanne Lorraine T. Datul BML2ADokumen32 halamanGenetic Disorder and Genetic Counselling: Ruthanne Lorraine T. Datul BML2AKhelly Joshua Uy100% (1)
- A State in Which Body Lacks O or Defective Aeration of Blood - Mechanical Interference With RespirationDokumen99 halamanA State in Which Body Lacks O or Defective Aeration of Blood - Mechanical Interference With RespirationVirendar Pal SinghBelum ada peringkat
- BurnsDokumen80 halamanBurnsAlina IlovanBelum ada peringkat
- Bone Marrow and Stem Cell TranspplantDokumen28 halamanBone Marrow and Stem Cell TranspplantVILLEJO JHOVIALENBelum ada peringkat
- Lecture 29 - Pathology of HypertensionDokumen24 halamanLecture 29 - Pathology of Hypertensionapi-3703352100% (6)
- Hydrocarbon PoisoningDokumen10 halamanHydrocarbon PoisoningVarshith GandlaBelum ada peringkat
- AnaphylaxisDokumen1 halamanAnaphylaxisMazo KhanBelum ada peringkat
- StarvationDokumen23 halamanStarvationUjjawalShriwastav100% (1)
- Transport of OxygenDokumen41 halamanTransport of OxygenEsther DeepikaBelum ada peringkat
- Forensic Medicine (Autosaved) 2Dokumen20 halamanForensic Medicine (Autosaved) 2Lohith RajBelum ada peringkat
- AsphyxiaDokumen55 halamanAsphyxiahelenthongBelum ada peringkat
- ASPHYXIA Introduction (2) .ZipDokumen37 halamanASPHYXIA Introduction (2) .Ziprooshan tahirBelum ada peringkat
- Quarterly Report On Case FindingDokumen2 halamanQuarterly Report On Case FindingTrishenth FonsekaBelum ada peringkat
- Quarterly Report On TB and non-TB WardsDokumen3 halamanQuarterly Report On TB and non-TB WardsTrishenth FonsekaBelum ada peringkat
- Quarterly Report On Program ManagementDokumen7 halamanQuarterly Report On Program ManagementTrishenth FonsekaBelum ada peringkat
- Quarterly Report On Sputum Conversion of Positive Patients at The End of Intensive PhaseDokumen1 halamanQuarterly Report On Sputum Conversion of Positive Patients at The End of Intensive PhaseTrishenth FonsekaBelum ada peringkat
- Quarterly Report On Microscopic Activities and LogisticsDokumen2 halamanQuarterly Report On Microscopic Activities and LogisticsTrishenth FonsekaBelum ada peringkat
- Quarterly Report On The Results of Treatment of Patients Registered 12-15 Months EarlierDokumen2 halamanQuarterly Report On The Results of Treatment of Patients Registered 12-15 Months EarlierTrishenth FonsekaBelum ada peringkat
- Register of TB SuspectsDokumen1 halamanRegister of TB SuspectsTrishenth FonsekaBelum ada peringkat
- Duties of MOHDokumen3 halamanDuties of MOHTrishenth FonsekaBelum ada peringkat
- Laborotory Manual For Tuberculosis ControlDokumen5 halamanLaborotory Manual For Tuberculosis ControlTrishenth FonsekaBelum ada peringkat
- National TB Control ManualDokumen223 halamanNational TB Control ManualTrishenth FonsekaBelum ada peringkat
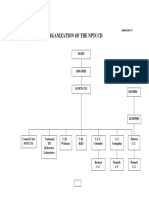
- Organization of NPTCCD PDFDokumen2 halamanOrganization of NPTCCD PDFTrishenth FonsekaBelum ada peringkat
- Lab Form For Sputum Examination PDFDokumen1 halamanLab Form For Sputum Examination PDFTrishenth FonsekaBelum ada peringkat
- District TB RegisterDokumen2 halamanDistrict TB RegisterTrishenth FonsekaBelum ada peringkat
- Living With AFib Patient GuideDokumen73 halamanLiving With AFib Patient GuideTrishenth FonsekaBelum ada peringkat
- QuotesDokumen1 halamanQuotesTrishenth FonsekaBelum ada peringkat
- Gas Poisoning (Irrespirable Gases) : Asphyxial DeathDokumen5 halamanGas Poisoning (Irrespirable Gases) : Asphyxial DeathTrishenth FonsekaBelum ada peringkat
- The Premature BabyDokumen92 halamanThe Premature BabyTrishenth Fonseka100% (1)
- Neck Pain and Pain Down The ArmDokumen27 halamanNeck Pain and Pain Down The ArmTrishenth FonsekaBelum ada peringkat
- 29 - Heart Disease Complicating PregnancyDokumen18 halaman29 - Heart Disease Complicating PregnancyTrishenth FonsekaBelum ada peringkat
- Paediatric UrologyDokumen194 halamanPaediatric UrologyTrishenth FonsekaBelum ada peringkat
- SLEDokumen42 halamanSLETrishenth FonsekaBelum ada peringkat
- 15 - CN Poisoning 2Dokumen2 halaman15 - CN Poisoning 2Trishenth FonsekaBelum ada peringkat
- 11 - SLMCDokumen27 halaman11 - SLMCTrishenth FonsekaBelum ada peringkat
- 13 - Medicolegal Duties of A DoctorDokumen13 halaman13 - Medicolegal Duties of A DoctorTrishenth FonsekaBelum ada peringkat
- 12 - Medical NegligenceDokumen34 halaman12 - Medical NegligenceTrishenth FonsekaBelum ada peringkat
- 11 - Professional SecrecyDokumen10 halaman11 - Professional SecrecyTrishenth Fonseka100% (1)
- 09 - Changes After Death and Time Since DeathDokumen9 halaman09 - Changes After Death and Time Since DeathTrishenth FonsekaBelum ada peringkat
- 10 - Introduction To Legal System in SLDokumen6 halaman10 - Introduction To Legal System in SLTrishenth FonsekaBelum ada peringkat
- 11 - Medical EthicsDokumen23 halaman11 - Medical EthicsTrishenth FonsekaBelum ada peringkat
- 08 - Post Mortem InstrumentsDokumen6 halaman08 - Post Mortem InstrumentsTrishenth FonsekaBelum ada peringkat
- Some of Us Had Been Threatening Our Friend ColbyDokumen3 halamanSome of Us Had Been Threatening Our Friend ColbyAngelaBelum ada peringkat
- Crime Scene Examination of Murder and Suicide CaseDokumen8 halamanCrime Scene Examination of Murder and Suicide CaseJonathan Dantas PessoaBelum ada peringkat
- EnglishNCRI Monthly - June 2010Dokumen231 halamanEnglishNCRI Monthly - June 2010HRcommitteeNCRIBelum ada peringkat
- A State in Which Body Lacks O or Defective Aeration of Blood - Mechanical Interference With RespirationDokumen99 halamanA State in Which Body Lacks O or Defective Aeration of Blood - Mechanical Interference With RespirationVirendar Pal SinghBelum ada peringkat
- Medico Legal Aspects of InvestigationDokumen171 halamanMedico Legal Aspects of InvestigationBhenjo Hernandez BaronaBelum ada peringkat
- List of Announced Executions 2010Dokumen37 halamanList of Announced Executions 2010HRcommitteeNCRIBelum ada peringkat
- Cdi 3 Special Crime InvestigationDokumen12 halamanCdi 3 Special Crime InvestigationMatias Winner100% (2)
- Insiden Bunuh Diri Secara Gantung DiriDokumen8 halamanInsiden Bunuh Diri Secara Gantung Diribellezaini.94Belum ada peringkat
- The Tale of The Melon CityDokumen9 halamanThe Tale of The Melon CityShubham KarandeBelum ada peringkat
- Materials Used For Suicidal Hanging Recorded During Autopsy From Sir Salimullah Medical College MorgueDokumen5 halamanMaterials Used For Suicidal Hanging Recorded During Autopsy From Sir Salimullah Medical College MorguecapitalBelum ada peringkat
- Commonly Confused WordsDokumen11 halamanCommonly Confused Wordscb107cs224Belum ada peringkat
- Asphyxial DeathDokumen25 halamanAsphyxial DeathanuzBelum ada peringkat
- A Hanging Coloured Notes PDFDokumen6 halamanA Hanging Coloured Notes PDFSaarah MehmoodBelum ada peringkat
- The End of Lynching in Marion County FloridaDokumen68 halamanThe End of Lynching in Marion County FloridaNeil Gillespie100% (3)
- Violent Asphyxial DeathsDokumen188 halamanViolent Asphyxial DeathsARIF-UR-REHMAN86% (14)
- Hanging: Methods of Judicial HangingDokumen12 halamanHanging: Methods of Judicial Hangingamiruljais92Belum ada peringkat
- Suicide by HangingDokumen12 halamanSuicide by HangingpanjiBelum ada peringkat
- Death by AsphyxiaDokumen82 halamanDeath by AsphyxiaJennifer Berg100% (1)
- Jeanne Lynch-Aird Thesis June 2016Dokumen221 halamanJeanne Lynch-Aird Thesis June 2016Agustín GonzálezBelum ada peringkat
- A Hanging - George OrwellDokumen4 halamanA Hanging - George OrwellChris Dougherty100% (1)
- Suicide or Homicide: Case ReportDokumen3 halamanSuicide or Homicide: Case ReportSuvedhya ReddyBelum ada peringkat
- Ligature Strangulation - StudentsDokumen28 halamanLigature Strangulation - StudentsBoţu Alexandru100% (1)
- CriminologyDokumen46 halamanCriminologysaif ali67% (3)
- English Monthly - Nov. 2010Dokumen401 halamanEnglish Monthly - Nov. 2010HRcommitteeNCRIBelum ada peringkat
- ESPYyearDokumen450 halamanESPYyearSean MorrisBelum ada peringkat
- Michelle Carter 1Dokumen9 halamanMichelle Carter 1api-349839396Belum ada peringkat
- InstitutionalDokumen221 halamanInstitutionalSEBIAL, LLOYD A.Belum ada peringkat
- The Newgate Calendar 01Dokumen410 halamanThe Newgate Calendar 01徐其門Belum ada peringkat
- Violent Asphyxial DeathsDokumen188 halamanViolent Asphyxial DeathsRoman MamunBelum ada peringkat
- MCQs in Forensic Medicine and Toxicology 6e by Redd PDFDokumen41 halamanMCQs in Forensic Medicine and Toxicology 6e by Redd PDFnabeel78786977% (22)