Anda mungkin juga menyukai
- Lim 2015Dokumen11 halamanLim 2015joshuaBelum ada peringkat
- 03JBC F9differentiationDokumen8 halaman03JBC F9differentiation이용문Belum ada peringkat
- Regenerative BiologyDokumen9 halamanRegenerative Biologymattyg35Belum ada peringkat
- Hegde SS - Identification of Bone-Specific Alkaline Phosphatase in Saliva and Its Correlation With Skeletal Age.Dokumen5 halamanHegde SS - Identification of Bone-Specific Alkaline Phosphatase in Saliva and Its Correlation With Skeletal Age.ShwethaBelum ada peringkat
- Biochimica Et Biophysica Acta: N. Plotegher, E. Gratton, L. BubaccoDokumen11 halamanBiochimica Et Biophysica Acta: N. Plotegher, E. Gratton, L. BubaccoDavor Dann'sBelum ada peringkat
- Transcription of The SCL TAL1 Interrupting Locus Stil - 2014 - Journal of BioDokumen7 halamanTranscription of The SCL TAL1 Interrupting Locus Stil - 2014 - Journal of BioMary GarridoBelum ada peringkat
- Neuroscience Letters: Laura Monni, Filippo Ghezzi, Silvia Corsini, Andrea NistriDokumen6 halamanNeuroscience Letters: Laura Monni, Filippo Ghezzi, Silvia Corsini, Andrea NistriardhiBelum ada peringkat
- Unique Features of Different Members of The HumanDokumen9 halamanUnique Features of Different Members of The HumanRadwan AlzidanBelum ada peringkat
- Caro 2012Dokumen9 halamanCaro 2012Ro BellingeriBelum ada peringkat
- Jurnal Enzim 3Dokumen4 halamanJurnal Enzim 3Laris Donar Marukkap SihombingBelum ada peringkat
- The Effects of Kisspeptin-10 On Serum Metabolism and Myocardium in RatsDokumen19 halamanThe Effects of Kisspeptin-10 On Serum Metabolism and Myocardium in RatsÁlex GómezBelum ada peringkat
- Arg9 人抗HBsAg单链抗体 EGFP融合蛋白基因的构建 表达及活性分析Dokumen4 halamanArg9 人抗HBsAg单链抗体 EGFP融合蛋白基因的构建 表达及活性分析api-3804372Belum ada peringkat
- Balic Et Al-2005-Orthodontics & Craniofacial ResearchDokumen7 halamanBalic Et Al-2005-Orthodontics & Craniofacial ResearchNicolas PintoBelum ada peringkat
- RANK/RANKL/OPG System in The Intervertebral Disc: Researcharticle Open AccessDokumen10 halamanRANK/RANKL/OPG System in The Intervertebral Disc: Researcharticle Open AccessSHURJEEL ALI KHANBelum ada peringkat
- Neurotrophic Properties of The Lion's Mane Medicinal Mushroom, Hericium Erinaceus (Higher Basidiomycetes) From MalaysiaDokumen16 halamanNeurotrophic Properties of The Lion's Mane Medicinal Mushroom, Hericium Erinaceus (Higher Basidiomycetes) From MalaysiaDayon BochniaBelum ada peringkat
- Biofeature: Applications of Green Fluorescent Protein in PlantsDokumen6 halamanBiofeature: Applications of Green Fluorescent Protein in Plantsannisa pramestiBelum ada peringkat
- Art 1Dokumen11 halamanArt 1KatherineSerranoBelum ada peringkat
- AgNPs Paper 9Dokumen15 halamanAgNPs Paper 9VILEOLAGOLDBelum ada peringkat
- Hefti - 1988Dokumen13 halamanHefti - 1988Majd HusseinBelum ada peringkat
- Agrimson 2017Dokumen15 halamanAgrimson 2017Jair BrachoBelum ada peringkat
- Wang 2015Dokumen14 halamanWang 2015Manuel Esquivel OrtegaBelum ada peringkat
- Flpstop, A Tool For Conditional Gene Control in DrosophilaDokumen33 halamanFlpstop, A Tool For Conditional Gene Control in DrosophilahaihuaiheBelum ada peringkat
- Genotoxic Damage Induced by Isopropanol in Germinal and Somatic Cells of Drosophila MelanogasterDokumen7 halamanGenotoxic Damage Induced by Isopropanol in Germinal and Somatic Cells of Drosophila MelanogasterD LorduyBelum ada peringkat
- Tujuh BelasDokumen5 halamanTujuh BelasPut_r4Belum ada peringkat
- Olivia et al. 2018_O nervo vago modula a expressão do BDNF e a neurogênese no hipocampo_ENPDokumen10 halamanOlivia et al. 2018_O nervo vago modula a expressão do BDNF e a neurogênese no hipocampo_ENPPierre AugustoBelum ada peringkat
- Role of NLRP3 Inflammasome in Eosinophilic and Non-Eosinophilic Chronic Rhinosinusitis With Nasal PolypsDokumen9 halamanRole of NLRP3 Inflammasome in Eosinophilic and Non-Eosinophilic Chronic Rhinosinusitis With Nasal PolypsStanislaus Stanley SuhermanBelum ada peringkat
- 2013 Article AbstractsDokumen135 halaman2013 Article Abstractsmilagros villanuevaBelum ada peringkat
- Nerve Growth Factor-Inducing Activity of Hericium Erinaceus in 1321N1 Human Astrocytoma CellsDokumen6 halamanNerve Growth Factor-Inducing Activity of Hericium Erinaceus in 1321N1 Human Astrocytoma Cellschad_woodsonBelum ada peringkat
- Jkaoms 41 171 PDFDokumen5 halamanJkaoms 41 171 PDFSabiha WaseemBelum ada peringkat
- Irf6-Related Gene Regulatory Network Involved in Palate and Lip DevelopmentDokumen6 halamanIrf6-Related Gene Regulatory Network Involved in Palate and Lip DevelopmentLeonardo Antonio Castillo ZegarraBelum ada peringkat
- What Is A Functional Genetic Polymorphism? Defining Classes of FunctionalityDokumen3 halamanWhat Is A Functional Genetic Polymorphism? Defining Classes of FunctionalityAxel CofréBelum ada peringkat
- Involucramiento de Leuo en Genes Con Resistencia A SulfaDokumen10 halamanInvolucramiento de Leuo en Genes Con Resistencia A SulfaDiegoBelum ada peringkat
- Synaptic Adhesion Molecule Igsf11 Regulates Synaptic Transmission and PlasticityDokumen13 halamanSynaptic Adhesion Molecule Igsf11 Regulates Synaptic Transmission and PlasticityElí LezamaBelum ada peringkat
- Pituitary Adenoma-Neuronal Choristoma Is A Pituitary Adenoma WithDokumen4 halamanPituitary Adenoma-Neuronal Choristoma Is A Pituitary Adenoma WithRoxana Ioana DumitriuBelum ada peringkat
- Archives of Oral BiologyDokumen7 halamanArchives of Oral BiologyElena NicuBelum ada peringkat
- 30 413 Vidas AFP: Summary and Explanation PrincipleDokumen8 halaman30 413 Vidas AFP: Summary and Explanation PrincipleHafizh Widi CahyonoBelum ada peringkat
- 5650100504_ftpDokumen7 halaman5650100504_ftpLeonardo SalesBelum ada peringkat
- Some Non-Classical Intragonadal Regulators of Fish ReproductionDokumen16 halamanSome Non-Classical Intragonadal Regulators of Fish ReproductionBagas Lantip PrakasaBelum ada peringkat
- Journal of Neurochemistry - 2011 - Kraut - Roles of sphingolipids in Drosophila development and diseaseDokumen15 halamanJournal of Neurochemistry - 2011 - Kraut - Roles of sphingolipids in Drosophila development and diseaseaaki2627Belum ada peringkat
- Functional Differences and Similarities in Activated Peripheral Blood Mononuclear Cells by Lipopolysaccharide or Phytohemagglutinin Stimulation Between Human and Cynomolgus Monkeys PDFDokumen25 halamanFunctional Differences and Similarities in Activated Peripheral Blood Mononuclear Cells by Lipopolysaccharide or Phytohemagglutinin Stimulation Between Human and Cynomolgus Monkeys PDFLluis GomezBelum ada peringkat
- Perkembangan Terakhir Dalam Diagnosa Klinik Penyakit Kusta: AbstrakDokumen2 halamanPerkembangan Terakhir Dalam Diagnosa Klinik Penyakit Kusta: AbstrakMuh Firdaus Burhan UthaBelum ada peringkat
- Nerve Growth Factor NGF A Potential Urinary BiomarDokumen10 halamanNerve Growth Factor NGF A Potential Urinary BiomarRyan AndrianBelum ada peringkat
- 2019 Article 421DTNDokumen8 halaman2019 Article 421DTNDulce Maria AngelesBelum ada peringkat
- Per in Etti 2008Dokumen8 halamanPer in Etti 2008Dhiya AlmandaBelum ada peringkat
- GTC Seminar 040716nht FNL 0Dokumen1 halamanGTC Seminar 040716nht FNL 0hidayatdery27Belum ada peringkat
- 1 s2.0 S0014488620304258 MainDokumen39 halaman1 s2.0 S0014488620304258 MainFelipe CourtBelum ada peringkat
- BCN 11 557Dokumen16 halamanBCN 11 557Michael UBelum ada peringkat
- Intranasal Administration of Nerve Growth Factor (NGF) Rescues Recognition Memory Deficits in AD11 anti-NGF Transgenic MiceDokumen6 halamanIntranasal Administration of Nerve Growth Factor (NGF) Rescues Recognition Memory Deficits in AD11 anti-NGF Transgenic MiceSergiy Prokofiy MontanoBelum ada peringkat
- Siqueira 2016Dokumen5 halamanSiqueira 2016Nikhil BhavsarBelum ada peringkat
- Herzog 2010Dokumen7 halamanHerzog 2010Enzo German ZampiniBelum ada peringkat
- Flaskos2011 Effects of Sub-Lethal Neurite Outgrowth Inhibitory Concentrations of Chlorpyrifos OxonDokumen7 halamanFlaskos2011 Effects of Sub-Lethal Neurite Outgrowth Inhibitory Concentrations of Chlorpyrifos OxonEmmanuel Domínguez RosalesBelum ada peringkat
- Bone Specific Alkaline PhophataseDokumen6 halamanBone Specific Alkaline PhophataseMohan DesaiBelum ada peringkat
- PNNJDokumen7 halamanPNNJDesi Aryati TampubolonBelum ada peringkat
- Full PDFDokumen6 halamanFull PDFChuco HarrisonBelum ada peringkat
- Fluorosis Induces ER Stress and Apoptosis in OsteoblastsDokumen8 halamanFluorosis Induces ER Stress and Apoptosis in OsteoblastsKenneth MBelum ada peringkat
- 1 s2.0 S0016648020304007 MainDokumen11 halaman1 s2.0 S0016648020304007 MainAntonio Luiz PereiraBelum ada peringkat
- PIIS001502821400363XDokumen7 halamanPIIS001502821400363XzhuzhendongBelum ada peringkat
- EIF4E Knoclout MiceDokumen28 halamanEIF4E Knoclout MiceLaura GarciaBelum ada peringkat
- Propolis Suppresses Tumor Growth by Inducing Apoptosis in Endothelial CellsDokumen5 halamanPropolis Suppresses Tumor Growth by Inducing Apoptosis in Endothelial CellsMirelaMilanBelum ada peringkat
- The GnRH Neuron and its ControlDari EverandThe GnRH Neuron and its ControlAllan E. HerbisonBelum ada peringkat
- Serial NumberDokumen1 halamanSerial NumberChien ChanBelum ada peringkat
- DberrDokumen28 halamanDberrChien ChanBelum ada peringkat
- Serial NumberDokumen1 halamanSerial NumberChien Chan100% (1)
- Eula Microsoft Visual StudioDokumen3 halamanEula Microsoft Visual StudioqwwerttyyBelum ada peringkat
- DberrDokumen28 halamanDberrChien ChanBelum ada peringkat
- Eula 11028Dokumen3 halamanEula 11028Chien ChanBelum ada peringkat
- Eula 11028Dokumen3 halamanEula 11028Chien ChanBelum ada peringkat
- Eula Microsoft Visual StudioDokumen3 halamanEula Microsoft Visual StudioqwwerttyyBelum ada peringkat
- Eula Microsoft Visual StudioDokumen3 halamanEula Microsoft Visual StudioqwwerttyyBelum ada peringkat
- Eula Microsoft Visual StudioDokumen3 halamanEula Microsoft Visual StudioqwwerttyyBelum ada peringkat
- Problem A:: School Tycoon ReadmeDokumen3 halamanProblem A:: School Tycoon ReadmedarnadaBelum ada peringkat
- EmailDokumen1 halamanEmailChien ChanBelum ada peringkat
- CV of Indonesian Nursing Professor and ResearcherDokumen5 halamanCV of Indonesian Nursing Professor and Researcherwedus2Belum ada peringkat
- Name: Nhlakanipho Surname: Khwela Student No.: 61541524 Module Code: BLG1502 Assignment No.: 02 Unique Number: 711357Dokumen8 halamanName: Nhlakanipho Surname: Khwela Student No.: 61541524 Module Code: BLG1502 Assignment No.: 02 Unique Number: 711357Nhlakana Kay KhwelaBelum ada peringkat
- Connective TissuesstudDokumen53 halamanConnective TissuesstudDanial Sharizul100% (1)
- General Biology 1 Workbook Pages 43 52Dokumen12 halamanGeneral Biology 1 Workbook Pages 43 52R VHIBelum ada peringkat
- Bio 473 Cardiac Activity Lab ReportDokumen4 halamanBio 473 Cardiac Activity Lab Reportapi-253602935Belum ada peringkat
- Illustrated Laboratory Activity 6 Test For Nucleic AcidsDokumen2 halamanIllustrated Laboratory Activity 6 Test For Nucleic AcidsAlthea Aubrey AgbayaniBelum ada peringkat
- Lesson 1 - Sex and GenderDokumen5 halamanLesson 1 - Sex and Genderweyn feitBelum ada peringkat
- Bioinstrumentation Assignment KQB7002 Case Study PDFDokumen60 halamanBioinstrumentation Assignment KQB7002 Case Study PDFShafiq JSeahBelum ada peringkat
- BiografieDokumen73 halamanBiografieAna-Maria PantazicaBelum ada peringkat
- Differences between Sexual and Asexual ReproductionDokumen12 halamanDifferences between Sexual and Asexual ReproductionrosalynBelum ada peringkat
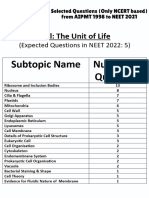
- Cell - The Unit of Life - NCERT Based PYQsDokumen9 halamanCell - The Unit of Life - NCERT Based PYQsAkhil singhBelum ada peringkat
- US Army Medical Course MD0804-200 - Therapeutics IDokumen197 halamanUS Army Medical Course MD0804-200 - Therapeutics IGeorges100% (1)
- X-Ald FinalDokumen3 halamanX-Ald Finalapi-271299065Belum ada peringkat
- Jurnal: Identifikasi Kromosom Homolog Melalui Deteksi Pada Tanaman Bawang MerahDokumen9 halamanJurnal: Identifikasi Kromosom Homolog Melalui Deteksi Pada Tanaman Bawang MerahImaniar FitriatasyaVWBelum ada peringkat
- Biophysics Assignment2 2k19ep042 Hrithik KalkalDokumen4 halamanBiophysics Assignment2 2k19ep042 Hrithik KalkalHarsh Raj EP-037Belum ada peringkat
- Section G: Vocabulary Cloze: Read The Passage Carefully, and Fill in The Blanks With The Words Provided in The BoxDokumen1 halamanSection G: Vocabulary Cloze: Read The Passage Carefully, and Fill in The Blanks With The Words Provided in The BoxNitya Nurul FadilahBelum ada peringkat
- The Bauhaus of Nature Peder Anker PDFDokumen24 halamanThe Bauhaus of Nature Peder Anker PDFtoomuchroseBelum ada peringkat
- Grade 11 - Mango Vaccination InformationDokumen2 halamanGrade 11 - Mango Vaccination InformationKENNEDY VAGAYBelum ada peringkat
- Microorganisms As BiofertilizerDokumen16 halamanMicroorganisms As Biofertilizersivaram888Belum ada peringkat
- Asepsia AntisepsiaDokumen110 halamanAsepsia AntisepsiaAlice Chirila100% (1)
- Zoo GeographyDokumen5 halamanZoo GeographySalma SabirBelum ada peringkat
- Bio 345 Evolution ASU Module 4 Cooperation - Sociality - PVLDokumen23 halamanBio 345 Evolution ASU Module 4 Cooperation - Sociality - PVLTiffanieBelum ada peringkat
- EritropoesisDokumen15 halamanEritropoesisFitriyani Dewi SuwandhiBelum ada peringkat
- Vegetative Incompatibility in Fungi: From Recognition To Cell Death, Whatever Does The TrickDokumen11 halamanVegetative Incompatibility in Fungi: From Recognition To Cell Death, Whatever Does The TrickXimena González GarcíaBelum ada peringkat
- COVID 19 Vaccine or Death VaccineDokumen10 halamanCOVID 19 Vaccine or Death VaccinejanzafarBelum ada peringkat
- Syllabus Gribble, BIOSC 0150, F14 PDFDokumen5 halamanSyllabus Gribble, BIOSC 0150, F14 PDFasdjfkj4kljrjsBelum ada peringkat
- Peripheral Nerve Injuries: Michael D. Robinson, M.D. Phillip R. Bryant, D.ODokumen156 halamanPeripheral Nerve Injuries: Michael D. Robinson, M.D. Phillip R. Bryant, D.OejekimBelum ada peringkat
- (Biophysical Techniques Series) Iain D. Campbell, Raymond A. Dwek-Biological Spectroscopy - Benjamin-Cummings Publishing Company (1984)Dokumen192 halaman(Biophysical Techniques Series) Iain D. Campbell, Raymond A. Dwek-Biological Spectroscopy - Benjamin-Cummings Publishing Company (1984)BrunoRamosdeLima100% (1)
- HIV Simple Case StudyDokumen13 halamanHIV Simple Case StudyJanna Pimentel100% (1)
- ChlorophytaDokumen13 halamanChlorophytamandow85Belum ada peringkat