Anda mungkin juga menyukai
- 702 FullDokumen10 halaman702 FullDesi HutapeaBelum ada peringkat
- KDIGO Optimal Anemia Management - Scope For Public ReviewDokumen13 halamanKDIGO Optimal Anemia Management - Scope For Public ReviewDesi HutapeaBelum ada peringkat
- Peritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDokumen6 halamanPeritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDesi HutapeaBelum ada peringkat
- Peritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDokumen9 halamanPeritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDesi HutapeaBelum ada peringkat
- Peritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDokumen9 halamanPeritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDesi HutapeaBelum ada peringkat
- Spond Ylo ArthritisDokumen5 halamanSpond Ylo ArthritisSuwandi AlghozyBelum ada peringkat
- Musa 2015Dokumen15 halamanMusa 2015Jose Luis Morales BautistaBelum ada peringkat
- Patof Spell PDFDokumen3 halamanPatof Spell PDFAnggi CalapiBelum ada peringkat
- ANCA Glomerulonephritis and VasculitisDokumen12 halamanANCA Glomerulonephritis and VasculitisSofía Elizabeth BlancoBelum ada peringkat
- ANCA Glomerulonephritis and VasculitisDokumen12 halamanANCA Glomerulonephritis and VasculitisSofía Elizabeth BlancoBelum ada peringkat
- Peritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDokumen6 halamanPeritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDesi HutapeaBelum ada peringkat
- Current Management of Acquired Solitary KidneyDokumen4 halamanCurrent Management of Acquired Solitary KidneyDesi HutapeaBelum ada peringkat
- Renal PhysiologyDokumen7 halamanRenal PhysiologyLucas TheotonioBelum ada peringkat
- Peritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDokumen6 halamanPeritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDesi HutapeaBelum ada peringkat
- 796 FullDokumen3 halaman796 FullDesi HutapeaBelum ada peringkat
- 796 FullDokumen3 halaman796 FullDesi HutapeaBelum ada peringkat
- KDIGO Dialysis Initiation Conf Report in PressDokumen11 halamanKDIGO Dialysis Initiation Conf Report in PressDesi HutapeaBelum ada peringkat
- FastDokumen10 halamanFastAnonymous Lxho3IBelum ada peringkat
- s41581 018 0077 4 PDFDokumen15 halamans41581 018 0077 4 PDFDesi HutapeaBelum ada peringkat
- s41581 018 0077 4 PDFDokumen15 halamans41581 018 0077 4 PDFDesi HutapeaBelum ada peringkat
- 28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDokumen5 halaman28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDesi HutapeaBelum ada peringkat
- Use of Vitamin D Drops Leading To Kidney Failure in A 54-Year-Old ManDokumen5 halamanUse of Vitamin D Drops Leading To Kidney Failure in A 54-Year-Old ManDesi HutapeaBelum ada peringkat
- CJN 10640918 FullDokumen8 halamanCJN 10640918 FullDesi HutapeaBelum ada peringkat
- Onco Neph PDFDokumen9 halamanOnco Neph PDFNarinder SharmaBelum ada peringkat
- 641 FullDokumen12 halaman641 FullDesi HutapeaBelum ada peringkat
- Relationship of Kidney Injury Biomarkers With Long-Term Cardiovascular Outcomes After Cardiac SurgeryDokumen9 halamanRelationship of Kidney Injury Biomarkers With Long-Term Cardiovascular Outcomes After Cardiac SurgeryDesi HutapeaBelum ada peringkat
- CJN 09630818 FullDokumen10 halamanCJN 09630818 FullDesi HutapeaBelum ada peringkat
- NephrologyDokumen10 halamanNephrologyDesi HutapeaBelum ada peringkat
- Nrneph 2017 2Dokumen17 halamanNrneph 2017 2Desi HutapeaBelum ada peringkat
- CJN 09630818 FullDokumen10 halamanCJN 09630818 FullDesi HutapeaBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Quantitative Analysis of Continuous Intravenous Infusions in Pediatric Anesthesia. Safety Implications of Dead Volume, Flow Rates, and Fluid DeliveryDokumen9 halamanQuantitative Analysis of Continuous Intravenous Infusions in Pediatric Anesthesia. Safety Implications of Dead Volume, Flow Rates, and Fluid DeliveryDavid Arvizo HuitronBelum ada peringkat
- NANIDokumen18 halamanNANIAkhmad “Billy Rafi” HambaliBelum ada peringkat
- Academic Qualifications Courses Taken in University: Disediakan OlehDokumen1 halamanAcademic Qualifications Courses Taken in University: Disediakan OlehKhairina GmBelum ada peringkat
- Data Obat Emesys New UpdateDokumen14 halamanData Obat Emesys New UpdateDhifa Mutia KiraniBelum ada peringkat
- Elfani Nur Sita Augustina-19084Dokumen6 halamanElfani Nur Sita Augustina-19084elfannynr augustinaBelum ada peringkat
- New PDF For PharmacologyDokumen236 halamanNew PDF For PharmacologyDIPENDRA KUMAR KUSHAWAHA100% (1)
- Hair TransplantDokumen7 halamanHair TransplantjessicaBelum ada peringkat
- 02-05 2022 Pharm Pharmacokinetics 2022 R3Dokumen38 halaman02-05 2022 Pharm Pharmacokinetics 2022 R3Amira HelayelBelum ada peringkat
- Medication Administration WorksheetDokumen6 halamanMedication Administration WorksheetCheska CarrionBelum ada peringkat
- BLS Interim Material 2020 - Provider Manual ChangesDokumen2 halamanBLS Interim Material 2020 - Provider Manual ChangesyossyusBelum ada peringkat
- Phenytoin PAR 45Dokumen65 halamanPhenytoin PAR 45Lourdes VictoriaBelum ada peringkat
- NAC Asthma COPD Medications Chart 2022 - A4 - WebDokumen1 halamanNAC Asthma COPD Medications Chart 2022 - A4 - WebkanemuraaBelum ada peringkat
- Format Lplpo 2019Dokumen57 halamanFormat Lplpo 2019Mutty Arra Zya RiezthicaBelum ada peringkat
- Role of Lithium Augmentation in The Management of Major Depressive DisorderDokumen12 halamanRole of Lithium Augmentation in The Management of Major Depressive Disorderdanilomarandola100% (1)
- Naproxen Best NSAID For Heart-Disease PatientsDokumen5 halamanNaproxen Best NSAID For Heart-Disease PatientskurniawanBelum ada peringkat
- Pooja ReviewDokumen6 halamanPooja ReviewKumar Sales Piyush JoshiBelum ada peringkat
- Airway Management in The Critically Ill: ReviewDokumen9 halamanAirway Management in The Critically Ill: ReviewQuarmina HesseBelum ada peringkat
- Prescribing Authority TableDokumen7 halamanPrescribing Authority TablearifadamjiBelum ada peringkat
- Who Par Guidance With AppendixesDokumen69 halamanWho Par Guidance With AppendixeslanikhilBelum ada peringkat
- Pharma Midterms Review UwuDokumen11 halamanPharma Midterms Review UwuAJ BayBelum ada peringkat
- Adrenergic DrugsDokumen33 halamanAdrenergic DrugsZsa Zsa FebryanaBelum ada peringkat
- Farmacologia en ArdillasDokumen3 halamanFarmacologia en ArdillasIvan Gonzalez BernalBelum ada peringkat
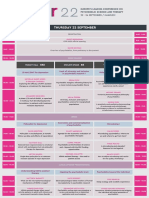
- Europe's Leading Conference on Psychedelic ScienceDokumen6 halamanEurope's Leading Conference on Psychedelic ScienceAndrei GeorgescuBelum ada peringkat
- World University of Bangladesh: An AssignmentDokumen5 halamanWorld University of Bangladesh: An AssignmentMD REFATBelum ada peringkat
- Dr. Wahyuni Indawati, Spa (K)Dokumen43 halamanDr. Wahyuni Indawati, Spa (K)Rara AnisaBelum ada peringkat
- Leipzig Applicator ConeDokumen3 halamanLeipzig Applicator Coneapi-295549343Belum ada peringkat
- BARCODESDokumen7 halamanBARCODESChitPerRhosBelum ada peringkat
- Anti Drug Abuse EducationDokumen32 halamanAnti Drug Abuse EducationGegegegBelum ada peringkat
- Islamabad. Up-Gradation of Official WebsiteDokumen4 halamanIslamabad. Up-Gradation of Official WebsiteAli RizviBelum ada peringkat
- Pharmacology Overview: Drug Actions, Administration & ResponsibilitiesDokumen10 halamanPharmacology Overview: Drug Actions, Administration & ResponsibilitiesNathaniel PulidoBelum ada peringkat