Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Role of Creativity in EntrepreneurshipDokumen35 halamanThe Role of Creativity in Entrepreneurshipscorpion999Belum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Using Mind Power and Affirmations 6 PagesDokumen6 halamanUsing Mind Power and Affirmations 6 Pagesscorpion999Belum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Ralf General Assessment Profile !Dokumen20 halamanRalf General Assessment Profile !scorpion999Belum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- A Complete Program For Living An Uncommon Life 63 PagesDokumen4 halamanA Complete Program For Living An Uncommon Life 63 Pagesscorpion999Belum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Beliefchange 29 Pages PDFDokumen29 halamanBeliefchange 29 Pages PDFscorpion999100% (1)
- Table 3: Nutritional Goals For Proposed Daily Food Intake Patterns Page 1, Goals For VitaminsDokumen4 halamanTable 3: Nutritional Goals For Proposed Daily Food Intake Patterns Page 1, Goals For Vitaminsscorpion999Belum ada peringkat
- Controlmind 25 PagesDokumen25 halamanControlmind 25 Pagesscorpion999Belum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Gloria Gonzalez: Reborn: The Wanderer in US Hispanic Literature. Sancho Rodriguez, ChairDokumen2 halamanGloria Gonzalez: Reborn: The Wanderer in US Hispanic Literature. Sancho Rodriguez, Chairscorpion999Belum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Assistant Accountant CV TemplateDokumen2 halamanAssistant Accountant CV Templatescorpion999Belum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rita CVDokumen2 halamanRita CVscorpion999Belum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Zap Your LifeDokumen27 halamanZap Your Lifescorpion999Belum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Target Suggested Suggested Target Suggested Suggested AGE EER Pattern EER Pattern (S) EER Pattern (S) AGE EER Pattern EER Pattern (S) EER Pattern (S)Dokumen2 halamanTarget Suggested Suggested Target Suggested Suggested AGE EER Pattern EER Pattern (S) EER Pattern (S) AGE EER Pattern EER Pattern (S) EER Pattern (S)scorpion999Belum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Iabc in Numbers: Connect With UsDokumen2 halamanIabc in Numbers: Connect With Usscorpion999Belum ada peringkat
- Agenda: TRX Suspension Trainer CourseDokumen1 halamanAgenda: TRX Suspension Trainer Coursescorpion999Belum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Rita CVDokumen2 halamanRita CVscorpion999Belum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- July - August Training2Dokumen7 halamanJuly - August Training2scorpion999Belum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A 3 Table of Surgical Procedures TOSP With Minor Surgical Procedures MSPs 1Dokumen94 halamanA 3 Table of Surgical Procedures TOSP With Minor Surgical Procedures MSPs 1Chee Yung NgBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- @MBS MedicalBooksStore 2020 Dentofacial Esthetics From Macro ToDokumen514 halaman@MBS MedicalBooksStore 2020 Dentofacial Esthetics From Macro ToMazen AlwajihBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Gut and Psychology Syndrome - Natural Treatment For Autism, Dyspraxia, A.D.130015Dokumen5 halamanGut and Psychology Syndrome - Natural Treatment For Autism, Dyspraxia, A.D.130015liza lizaBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
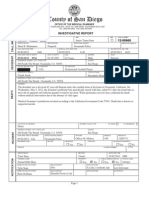
- Junior Seau Autopsy ReportDokumen16 halamanJunior Seau Autopsy ReportDeadspin83% (6)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- BNB ListDokumen73 halamanBNB ListbenBelum ada peringkat
- Hemophilic ArthropathyDokumen2 halamanHemophilic ArthropathyKimmybee GarciaBelum ada peringkat
- Yoga and PainDokumen29 halamanYoga and PainGanesh Babu100% (1)
- Management of Failed Block - Harsh.Dokumen48 halamanManagement of Failed Block - Harsh.Faeiz KhanBelum ada peringkat
- Ahprn Getting Involved in Research A Pocket Guide 0 0 0Dokumen215 halamanAhprn Getting Involved in Research A Pocket Guide 0 0 0Rusnifaezah MusaBelum ada peringkat
- Substance Abuse Counseling Complete 5th EditionDokumen379 halamanSubstance Abuse Counseling Complete 5th EditionTravis Blankenship100% (4)
- Planetary ThreadsDokumen2 halamanPlanetary ThreadsViviana PueblaBelum ada peringkat
- Mood Disorder and SuicideDokumen58 halamanMood Disorder and SuicideMichael AsetreBelum ada peringkat
- Sixth ScheduleDokumen3 halamanSixth Scheduleangelene koidBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Patient Blood Management Equals Patient SafetyDokumen19 halamanPatient Blood Management Equals Patient SafetyMuhammadBudiman RbcBelum ada peringkat
- Mental Illness and HomelessnessDokumen2 halamanMental Illness and HomelessnessLauren FaustBelum ada peringkat
- What To Know About General AnesthesiaDokumen8 halamanWhat To Know About General AnesthesiaPADAYON MEDISINABelum ada peringkat
- Topical AntifungalsDokumen14 halamanTopical AntifungalsRasha Mohammad100% (1)
- Ankle FracturesDokumen41 halamanAnkle Fracturesshammasbm100% (12)
- Perineal RuptureDokumen24 halamanPerineal RuptureIzz ShuhaimiBelum ada peringkat
- Engineering A Healthy Body: Career CatalystDokumen6 halamanEngineering A Healthy Body: Career CatalystB6D4N0Belum ada peringkat
- The Homeopathic Treatment of Ear Infections PDFDokumen104 halamanThe Homeopathic Treatment of Ear Infections PDFdipgang7174Belum ada peringkat
- West Bengal's Leather Industry OpportunitiesDokumen5 halamanWest Bengal's Leather Industry OpportunitiesDeepak AgarwalBelum ada peringkat
- Final1 1Dokumen23 halamanFinal1 1sheena LesBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Endodontic Clinic Manual 2015 - 1Dokumen134 halamanEndodontic Clinic Manual 2015 - 1Adina Popa100% (2)
- Wastewater Treatment Advanced PDFDokumen368 halamanWastewater Treatment Advanced PDFradoineBelum ada peringkat
- Week 1 - Trauma (BB)Dokumen11 halamanWeek 1 - Trauma (BB)lizzy596Belum ada peringkat
- Self Efficacy Theory - Case StudiesDokumen13 halamanSelf Efficacy Theory - Case StudiesPetros Akin-Nibosun0% (1)
- Renal Cell Carcinoma: DR Kalyan K Sarkar Ms FrcsedDokumen38 halamanRenal Cell Carcinoma: DR Kalyan K Sarkar Ms FrcsedMichael ParkBelum ada peringkat
- Discharge Planning of DM2Dokumen2 halamanDischarge Planning of DM2Robert BianesBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 4.5 dari 5 bintang4.5/5 (82)