Anda mungkin juga menyukai
- Measles 2019 AerDokumen9 halamanMeasles 2019 AerJose BritesBelum ada peringkat
- Gono Aer 2022 Report FinalDokumen10 halamanGono Aer 2022 Report FinalLIFO LIFO (Magazine)Belum ada peringkat
- Euro Area Unemployment at 7.3%: October 2021Dokumen6 halamanEuro Area Unemployment at 7.3%: October 2021jetiradoBelum ada peringkat
- EU Population in 2020: Almost 448 Million: First Population Estimates More Deaths Than BirthsDokumen6 halamanEU Population in 2020: Almost 448 Million: First Population Estimates More Deaths Than BirthsEly Go AbarquezBelum ada peringkat
- Chlam Aer 2022 ReportDokumen9 halamanChlam Aer 2022 ReportLIFO LIFO (Magazine)Belum ada peringkat
- Proilul IT-istilor RomaniDokumen5 halamanProilul IT-istilor RomaniClaudiuBelum ada peringkat
- 9 25102016 Ap enDokumen5 halaman9 25102016 Ap enVeronica OlteanuBelum ada peringkat
- 1 Ghid GDPR Colegiul Psihologilor 23052018Dokumen5 halaman1 Ghid GDPR Colegiul Psihologilor 23052018CatalinTascaBelum ada peringkat
- Table 1: Health Expenditure in OECD Countries, 2000 To 2006Dokumen8 halamanTable 1: Health Expenditure in OECD Countries, 2000 To 2006snamicampaniaBelum ada peringkat
- CPI 2009 Regional Highlights EU WE en - Corruption Perceptions Index 2009 - Regional Highlights For The European Union and Western EuropeDokumen2 halamanCPI 2009 Regional Highlights EU WE en - Corruption Perceptions Index 2009 - Regional Highlights For The European Union and Western EuropeJon C.Belum ada peringkat
- Education Trainning Monitor 2020Dokumen8 halamanEducation Trainning Monitor 2020sales002-1Belum ada peringkat
- BP Stats Review 2018 All DataDokumen111 halamanBP Stats Review 2018 All DataNeeraj YadavBelum ada peringkat
- Dengue: Surveillance ReportDokumen7 halamanDengue: Surveillance Reportramona donisaBelum ada peringkat
- BP Statistical ReviewDokumen158 halamanBP Statistical Reviewbrayan7uribeBelum ada peringkat
- Ecv TemplateDokumen1 halamanEcv TemplateVieru VeronicaBelum ada peringkat
- Table 1: Number of Tertiary Education Students by Level and Sex, 2015Dokumen52 halamanTable 1: Number of Tertiary Education Students by Level and Sex, 2015Delia RaduBelum ada peringkat
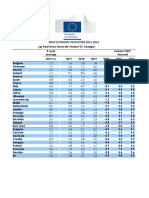
- Forecast Tables EN PDFDokumen2 halamanForecast Tables EN PDFSyed Maratab AliBelum ada peringkat
- BP Statistical Review of World Energy 2017 Underpinning DataDokumen69 halamanBP Statistical Review of World Energy 2017 Underpinning DatadairandexBelum ada peringkat
- Ecfin Forecast Spring 2020 Overview en 0Dokumen6 halamanEcfin Forecast Spring 2020 Overview en 0Gordon FreenmanBelum ada peringkat
- Euro Area Annual Inflation Up To 8.6%: Flash Estimate - June 2022Dokumen2 halamanEuro Area Annual Inflation Up To 8.6%: Flash Estimate - June 2022Milan PetrikBelum ada peringkat
- Note On Stock of Liabilities of Trade Credits and AdvancesDokumen2 halamanNote On Stock of Liabilities of Trade Credits and Advancesathanasios_syrakisBelum ada peringkat
- BP Statistical Review of World Energy 2017: Energy Consumption DataDokumen70 halamanBP Statistical Review of World Energy 2017: Energy Consumption DataThales MacêdoBelum ada peringkat
- 5 07052010 Ap enDokumen3 halaman5 07052010 Ap enpapintoBelum ada peringkat
- EU Local Government Key DataDokumen26 halamanEU Local Government Key DataKicki AnderssonBelum ada peringkat
- IMF - WEO - 202004 - Statistical Appendix - Tables B PDFDokumen8 halamanIMF - WEO - 202004 - Statistical Appendix - Tables B PDFAnna VassilovskiBelum ada peringkat
- Inflació 1Dokumen2 halamanInflació 1Maria José RodríguezBelum ada peringkat
- World's top steel producing countries in 2010Dokumen3 halamanWorld's top steel producing countries in 2010Harprit SinghBelum ada peringkat
- Ip183 - en - Statistical AnnexDokumen3 halamanIp183 - en - Statistical AnnexPeter DerdakBelum ada peringkat
- Commercial vehicle registrations in EU down 4% in December 2018Dokumen7 halamanCommercial vehicle registrations in EU down 4% in December 2018Dan RosoiuBelum ada peringkat
- GDP Up by 0.6% in Both The Euro Area and The EU28: Flash Estimate For The Second Quarter of 2017Dokumen3 halamanGDP Up by 0.6% in Both The Euro Area and The EU28: Flash Estimate For The Second Quarter of 2017loginxscribdBelum ada peringkat
- Chapter 13: International Comparisons: 2015 Annual Data Report V 2: E - S R DDokumen51 halamanChapter 13: International Comparisons: 2015 Annual Data Report V 2: E - S R DPankaj DasBelum ada peringkat
- France 2021-07-22 Deaths Covid 19Dokumen175 halamanFrance 2021-07-22 Deaths Covid 19Guillaume FeralBelum ada peringkat
- m4 Imports of CoffeeDokumen1 halamanm4 Imports of Coffeedorie_dorinaBelum ada peringkat
- Table 53: Taxes On Capital As % of GDP - TotalDokumen30 halamanTable 53: Taxes On Capital As % of GDP - TotalRalwkwtza NykoBelum ada peringkat
- Aer Hep B 2020 Final CorrectedDokumen11 halamanAer Hep B 2020 Final Correctedelena pintiliiBelum ada peringkat
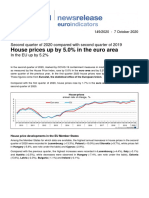
- House prices up 5% in euro area and EU in Q2 2020Dokumen3 halamanHouse prices up 5% in euro area and EU in Q2 2020PapasimaBelum ada peringkat
- European Union: Statistical FactsheetDokumen22 halamanEuropean Union: Statistical FactsheetloginxscribdBelum ada peringkat
- 6fc55141 enDokumen2 halaman6fc55141 enTalila SidaBelum ada peringkat
- The European Foundry Industry 2019 Annual Statistics and National Reports 1Dokumen112 halamanThe European Foundry Industry 2019 Annual Statistics and National Reports 1Ryan KnightBelum ada peringkat
- 9 Statistica InternationalaDokumen19 halaman9 Statistica InternationalaMihai GandraburaBelum ada peringkat
- Energy Prices International Comparisons: Industrial Electricity Prices in The IEADokumen8 halamanEnergy Prices International Comparisons: Industrial Electricity Prices in The IEAUfficioBelum ada peringkat
- ВВП с 2010 с Другими СтранамиDokumen18 halamanВВП с 2010 с Другими СтранамилюдмилаBelum ada peringkat
- Of Total ExportsDokumen1 halamanOf Total ExportsLya HellenBelum ada peringkat
- Annex Table 38. Export Volumes of Goods and Services: Source: OECD Economic Outlook 88 DatabaseDokumen17 halamanAnnex Table 38. Export Volumes of Goods and Services: Source: OECD Economic Outlook 88 DatabaseRaghvendra NarayanBelum ada peringkat
- Educ - Thpertch-Teachers and Trainers Age Distributions - Pupils To Teachers RatioDokumen10 halamanEduc - Thpertch-Teachers and Trainers Age Distributions - Pupils To Teachers RatioDesa MarkovicBelum ada peringkat
- Seasonally adjusted unemployment rates across EuropeDokumen6 halamanSeasonally adjusted unemployment rates across EuropeRobert SzymańskiBelum ada peringkat
- Unemployment by Sex and Age - Annual Data (UNE - RT - A - Custom - 2553687)Dokumen10 halamanUnemployment by Sex and Age - Annual Data (UNE - RT - A - Custom - 2553687)Nicoleta DinuBelum ada peringkat
- ACEA Report: Vehicles in Use Europe 2019Dokumen21 halamanACEA Report: Vehicles in Use Europe 2019spam.recycler1048Belum ada peringkat
- Indice BigmacDokumen71 halamanIndice BigmacDidier RamosBelum ada peringkat
- 33020do001 2019Dokumen4 halaman33020do001 2019Ngọc AnhBelum ada peringkat
- Leading Causes of Death in EuropeDokumen62 halamanLeading Causes of Death in EuropeBogdanRacoviteanuBelum ada peringkat
- Analytics Pageviews by Countries EuropeDokumen2 halamanAnalytics Pageviews by Countries Europesameh aboulsoudBelum ada peringkat
- Consumer Prices - Inflation FP2018Dokumen20 halamanConsumer Prices - Inflation FP2018Dylan ShoBelum ada peringkat
- 2 13112020 Ap enDokumen1 halaman2 13112020 Ap enWeb AdevarulBelum ada peringkat
- Statistical Review of World Energy: 2020 - 69 EditionDokumen4 halamanStatistical Review of World Energy: 2020 - 69 Editionvishalbhavar1Belum ada peringkat
- ВВП с 2010 Годовые ДанныеDokumen7 halamanВВП с 2010 Годовые ДанныелюдмилаBelum ada peringkat
- Ilc mddw02Dokumen10 halamanIlc mddw02Andy LupuBelum ada peringkat
- 2 13052011 Ap enDokumen2 halaman2 13052011 Ap enShruthi JayaramBelum ada peringkat
- 2001 (Corrigendum) - 1Dokumen8 halaman2001 (Corrigendum) - 1KonstantinBelum ada peringkat
- America, Japan & Asia Pacific: America, Japan & Asia PacificDari EverandAmerica, Japan & Asia Pacific: America, Japan & Asia PacificBelum ada peringkat
- Variable Dictionary VaccineTracker-04!11!2021Dokumen3 halamanVariable Dictionary VaccineTracker-04!11!2021Francisca BallesterosBelum ada peringkat
- Joint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Dokumen7 halamanJoint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Francisca BallesterosBelum ada peringkat
- 3interim Advice For Public Health Authorities On Summer Events MPXDokumen6 halaman3interim Advice For Public Health Authorities On Summer Events MPXFrancisca BallesterosBelum ada peringkat
- 5communicable Disease Threats Report 30 Jul 2022 PublicDokumen28 halaman5communicable Disease Threats Report 30 Jul 2022 PublicFrancisca BallesterosBelum ada peringkat
- 2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeDokumen11 halaman2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeFrancisca BallesterosBelum ada peringkat
- Interim Public Health Considerations For COVID 19 Vaccination of AdolescentsDokumen19 halamanInterim Public Health Considerations For COVID 19 Vaccination of AdolescentsFrancisca BallesterosBelum ada peringkat
- ROA Salmonella-Enteritidis-ST11 2022 FinalDokumen19 halamanROA Salmonella-Enteritidis-ST11 2022 FinalFrancisca BallesterosBelum ada peringkat
- 1considerations For Contact Tracing MPX June 2022Dokumen13 halaman1considerations For Contact Tracing MPX June 2022Francisca BallesterosBelum ada peringkat
- Use of Antibody Tests For SARS COV 2 in The Context of Digital Green CertificatesDokumen5 halamanUse of Antibody Tests For SARS COV 2 in The Context of Digital Green CertificatesFrancisca BallesterosBelum ada peringkat
- Antimicrobial Resistance Europe 2015Dokumen120 halamanAntimicrobial Resistance Europe 2015Francisca BallesterosBelum ada peringkat
- Description and Disclaimer Daily ReportingDokumen1 halamanDescription and Disclaimer Daily ReportingFrancisca BallesterosBelum ada peringkat
- COVID 19 in Children and The Role of School Settings in Transmission Second UpdateDokumen37 halamanCOVID 19 in Children and The Role of School Settings in Transmission Second UpdateFrancisca BallesterosBelum ada peringkat
- COVID 19 Considerations For Booster Doses in Adolescents Feb 2022Dokumen14 halamanCOVID 19 Considerations For Booster Doses in Adolescents Feb 2022Francisca BallesterosBelum ada peringkat
- 2021-01-13 Variable Dictionary and Disclaimer National Weekly DataDokumen1 halaman2021-01-13 Variable Dictionary and Disclaimer National Weekly DataFrancisca BallesterosBelum ada peringkat
- Communicable Disease Threats Report 16 Jun 2018Dokumen11 halamanCommunicable Disease Threats Report 16 Jun 2018Francisca BallesterosBelum ada peringkat
- Variable Dictionary VaccineTracker-20-08-2021Dokumen3 halamanVariable Dictionary VaccineTracker-20-08-2021Francisca BallesterosBelum ada peringkat
- Agenda EAAD - European-Level Launch EventDokumen1 halamanAgenda EAAD - European-Level Launch EventFrancisca BallesterosBelum ada peringkat
- ECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyDokumen1 halamanECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyFrancisca BallesterosBelum ada peringkat
- Communicable Disease Threats Report 26 Aug 2017Dokumen9 halamanCommunicable Disease Threats Report 26 Aug 2017Francisca BallesterosBelum ada peringkat
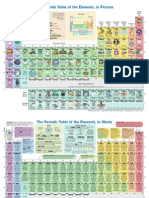
- The Periodic Table of Elements, in PicturesDokumen2 halamanThe Periodic Table of Elements, in Picturesrustyy88100% (1)
- Zika Virus Safety of Substances of Human Origin Update 2017 WebDokumen35 halamanZika Virus Safety of Substances of Human Origin Update 2017 WebFrancisca BallesterosBelum ada peringkat
- Ecdc Infographics2015 Measles Is SeriousDokumen1 halamanEcdc Infographics2015 Measles Is SeriousFrancisca BallesterosBelum ada peringkat
- ECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEADokumen1 halamanECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEAFrancisca BallesterosBelum ada peringkat
- Communicable Disease Threats Report 29 Jul 2017Dokumen13 halamanCommunicable Disease Threats Report 29 Jul 2017Francisca BallesterosBelum ada peringkat
- ECDC - ECDC Policy Briefing - Preparing For Zika in The EUDokumen1 halamanECDC - ECDC Policy Briefing - Preparing For Zika in The EUFrancisca BallesterosBelum ada peringkat
- Who Ccsivd Meetingreport SangreDokumen31 halamanWho Ccsivd Meetingreport SangreFrancisca BallesterosBelum ada peringkat
- ECDC Policy BriefingsDokumen1 halamanECDC Policy BriefingsFrancisca BallesterosBelum ada peringkat
- ECDC Epidemiological SituationDokumen1 halamanECDC Epidemiological SituationFrancisca BallesterosBelum ada peringkat
- ECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsDokumen2 halamanECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsFrancisca BallesterosBelum ada peringkat
- Surgical Site Infections - Review of Current Knowledge, Methods of PreventionDokumen7 halamanSurgical Site Infections - Review of Current Knowledge, Methods of PreventionVeronica GarciaBelum ada peringkat
- 2014 BRE IndianapolisDokumen3.495 halaman2014 BRE IndianapolisIan ScottBelum ada peringkat
- Vaccine Mandate ReinstatementDokumen8 halamanVaccine Mandate ReinstatementChicago Transit Justice CoalitionBelum ada peringkat
- Fundamentals of Nursing 1Dokumen2 halamanFundamentals of Nursing 1Alura Marez Doroteo100% (2)
- Lead Report 2019 Full OnlineDokumen19 halamanLead Report 2019 Full OnlineCrain's New York BusinessBelum ada peringkat
- Extended Zimbabwe National AIDS Strategic Plan 3Dokumen80 halamanExtended Zimbabwe National AIDS Strategic Plan 3Mxolisi Ncube0% (1)
- (2192021123313 PM) Sasolmed Member Guide 2021 - Updated 15 FebDokumen82 halaman(2192021123313 PM) Sasolmed Member Guide 2021 - Updated 15 FebLenox D LengauBelum ada peringkat
- Module 1 NRSG780Dokumen12 halamanModule 1 NRSG780justdoyourBelum ada peringkat
- SCH PHealthDokumen45 halamanSCH PHealthSilas Yenbon SebireBelum ada peringkat
- Fourth Quarter ReviewDokumen51 halamanFourth Quarter ReviewshichishopBelum ada peringkat
- SDCEP Antibiotic Prophylaxis Implementation Advice PDFDokumen32 halamanSDCEP Antibiotic Prophylaxis Implementation Advice PDFNeil TannaBelum ada peringkat
- Research Methods - A Framework For Evidence-Based Clinical Practice-Wendy L. Hurley, Craig R.Dokumen450 halamanResearch Methods - A Framework For Evidence-Based Clinical Practice-Wendy L. Hurley, Craig R.DannyCespedes100% (1)
- Health Maintenance: Guidelines For AdultsDokumen6 halamanHealth Maintenance: Guidelines For AdultsgurneeBelum ada peringkat
- Hiv ProphylaxisDokumen193 halamanHiv ProphylaxisKiran MishraBelum ada peringkat
- Types and Forms of Tourism: Senior Lecturer Cornelia Elena Tureac, PHDDokumen12 halamanTypes and Forms of Tourism: Senior Lecturer Cornelia Elena Tureac, PHDFarhan100% (1)
- Sustainable Development Goals (SDGS) : Maria Imelda Tokan 03016089Dokumen19 halamanSustainable Development Goals (SDGS) : Maria Imelda Tokan 03016089Rilda TokanBelum ada peringkat
- Arega DegifeDokumen64 halamanArega DegifeFuad Nasir 0913Belum ada peringkat
- Epidemiology Course for Midwifery StudentsDokumen326 halamanEpidemiology Course for Midwifery StudentsYoseph KassaBelum ada peringkat
- pr2 Revised PaperDokumen57 halamanpr2 Revised PaperTo PakBelum ada peringkat
- Vap Poster WPB VaDokumen1 halamanVap Poster WPB VaJoe ThesecondmonthBelum ada peringkat
- 07.08 Einstein S Falls HonorsDokumen3 halaman07.08 Einstein S Falls Honorsjackson combassBelum ada peringkat
- (AIIMS May 2014) (MP 2004)Dokumen4 halaman(AIIMS May 2014) (MP 2004)Dr-Sanjay Singhania100% (1)
- DoctorsHanbook FullversionDokumen126 halamanDoctorsHanbook FullversioniseefurtheroBelum ada peringkat
- Haemophilia - 2022 - Carcao - Low Dose Prophylaxis and Antifibrinolytics Options To Consider With Proven Benefits ForDokumen9 halamanHaemophilia - 2022 - Carcao - Low Dose Prophylaxis and Antifibrinolytics Options To Consider With Proven Benefits FordavidBelum ada peringkat
- Gulifardo - Lab Worksheet 2 The C.A.R.S. Model and Data Extraction TableDokumen4 halamanGulifardo - Lab Worksheet 2 The C.A.R.S. Model and Data Extraction TableKarylle Ezra GulifardoBelum ada peringkat
- Association Between Prophylactic Oxytocin Use During Dilation and Evacuation and Estimated Blood LossDokumen6 halamanAssociation Between Prophylactic Oxytocin Use During Dilation and Evacuation and Estimated Blood LossJhon CBelum ada peringkat
- Primary Health Care ConceptsDokumen71 halamanPrimary Health Care ConceptsKeshia Joyce Lim100% (4)
- DGHS IPHS CommunityHealthCentresDokumen120 halamanDGHS IPHS CommunityHealthCentresSargam MahendruBelum ada peringkat
- Foundations For Population Health in Community Public Health Nursing 5th Edition Stanhope Test BankDokumen8 halamanFoundations For Population Health in Community Public Health Nursing 5th Edition Stanhope Test Bankhieudermotjm7w100% (28)
- Antibiotics in NeurosurgeryDokumen12 halamanAntibiotics in Neurosurgerylouglee9174100% (1)