Anda mungkin juga menyukai
- Unified Parkinson's Disease Rating Scale GuideDokumen8 halamanUnified Parkinson's Disease Rating Scale GuideHanny Novia RiniBelum ada peringkat
- Neurological EponymsDokumen403 halamanNeurological EponymsJesus7Rah100% (1)
- Parts of A Neuron: 1. Dendrites 2. Cell Body With Nucleus 3. Axon 4. Synaptic TerminalDokumen3 halamanParts of A Neuron: 1. Dendrites 2. Cell Body With Nucleus 3. Axon 4. Synaptic TerminalDonald KingBelum ada peringkat
- Application of The Sleep Disturbance Scale For Children (SDSC) in Preschool AgeDokumen9 halamanApplication of The Sleep Disturbance Scale For Children (SDSC) in Preschool AgeerikafebriyanarBelum ada peringkat
- Sleep Habits and Disturbances in Malaysian Children With EpilepsyDokumen5 halamanSleep Habits and Disturbances in Malaysian Children With EpilepsynoiBelum ada peringkat
- Sleep Studies in ChildrenDokumen12 halamanSleep Studies in ChildrenJHONATAN MATA ARANDABelum ada peringkat
- Actigrafia Na InfanciaDokumen6 halamanActigrafia Na InfanciaAlexPsrBelum ada peringkat
- Sleep patterns in children with autismDokumen7 halamanSleep patterns in children with autismpsicosmosBelum ada peringkat
- ajol-file-journals_414_articles_227458_submission_proof_227458-4933-553839-1-10-20220630Dokumen5 halamanajol-file-journals_414_articles_227458_submission_proof_227458-4933-553839-1-10-20220630daaktarsaabBelum ada peringkat
- Sleep, Chronotype, and Sleep Hygiene in Children With Attention Deficit/hyperactivity Disorder, Autism Spectrum Disorder, and ControlsDokumen13 halamanSleep, Chronotype, and Sleep Hygiene in Children With Attention Deficit/hyperactivity Disorder, Autism Spectrum Disorder, and ControlsAndrea Marcela Medina RBelum ada peringkat
- Sleep Interventions For Children With Attention Deficit Hyperactivity Disorder (ADHD) : A Systematic Literature ReviewDokumen12 halamanSleep Interventions For Children With Attention Deficit Hyperactivity Disorder (ADHD) : A Systematic Literature ReviewRamacil Afsan NotoprawiroBelum ada peringkat
- 2022 General Movements e Desenvolvimento Aos 2 AnosDokumen13 halaman2022 General Movements e Desenvolvimento Aos 2 AnosCibelle FormigaBelum ada peringkat
- PR 1Dokumen17 halamanPR 1ajgars175Belum ada peringkat
- Sleep-Related Disorders in Children With Attention-Deficit Hyperactivity Disorder: Preliminary Results of A Full Sleep Assessment StudyDokumen9 halamanSleep-Related Disorders in Children With Attention-Deficit Hyperactivity Disorder: Preliminary Results of A Full Sleep Assessment StudyPierluigi CongedoBelum ada peringkat
- Melatonin & Autism DisorderDokumen5 halamanMelatonin & Autism DisorderNeutron ZionBelum ada peringkat
- Related Literature PDFDokumen4 halamanRelated Literature PDFNathaniel Kent Amiril CruzBelum ada peringkat
- Tdah 1Dokumen8 halamanTdah 1Roberto Alexis Molina CampuzanoBelum ada peringkat
- CraniomanuscriptV3revisedmanuscript ForresearchgateDokumen19 halamanCraniomanuscriptV3revisedmanuscript ForresearchgatefelitaBelum ada peringkat
- Sleep Phenotypes in Attention Deficit Hyperactivity DisorderDokumen35 halamanSleep Phenotypes in Attention Deficit Hyperactivity DisorderPierluigi CongedoBelum ada peringkat
- Autism SleepDokumen9 halamanAutism SleepdrimranmnooraniBelum ada peringkat
- Sleep Disorders in Adolescents: Sujay Kansagra, MDDokumen8 halamanSleep Disorders in Adolescents: Sujay Kansagra, MDMuliana DatuBelum ada peringkat
- Sleep-Wake Disorders in ChildhoodDokumen36 halamanSleep-Wake Disorders in Childhooddr.cidgutBelum ada peringkat
- Artigo 01Dokumen13 halamanArtigo 01Danielle CostaBelum ada peringkat
- 1617177589Dokumen9 halaman1617177589350southBelum ada peringkat
- Sleep in Children With Autism With and Without Autistic RegressionDokumen10 halamanSleep in Children With Autism With and Without Autistic RegressionpsicosmosBelum ada peringkat
- Research Article: Sleep Disturbance in ADHD Children: Prevalence, Clinical Profile and InfluencingDokumen10 halamanResearch Article: Sleep Disturbance in ADHD Children: Prevalence, Clinical Profile and InfluencingHoney M. LopezBelum ada peringkat
- Artigo 05Dokumen24 halamanArtigo 05Danielle CostaBelum ada peringkat
- Bruni-2004-Sleep Disturbances in As A Questionnaire StudyDokumen8 halamanBruni-2004-Sleep Disturbances in As A Questionnaire Studybappi11Belum ada peringkat
- Pediatric Sleep DisordersDokumen6 halamanPediatric Sleep DisordersAngela GuerreroBelum ada peringkat
- 10 11648 J CNN 20200402 12Dokumen4 halaman10 11648 J CNN 20200402 12inunBelum ada peringkat
- Nonpharmacologic Management of Excessive Daytime Sleepiness: Matthew R. EbbenDokumen9 halamanNonpharmacologic Management of Excessive Daytime Sleepiness: Matthew R. Ebbendoghat834Belum ada peringkat
- New Research Finds Prolonged-Release Melatonin Effective for Autism InsomniaDokumen14 halamanNew Research Finds Prolonged-Release Melatonin Effective for Autism InsomniaAlumno del Doctorado FarmacologiaBelum ada peringkat
- CSHQ Article PDFDokumen9 halamanCSHQ Article PDFmerawatidyahsepitaBelum ada peringkat
- Prognosis For Ambulation in Cerebral Palsy: A Population-Based StudyDokumen10 halamanPrognosis For Ambulation in Cerebral Palsy: A Population-Based StudyRania EBelum ada peringkat
- 18 01 031 20200804Dokumen7 halaman18 01 031 20200804christinaceciliaaBelum ada peringkat
- Biomedical Journal: SciencedirectDokumen8 halamanBiomedical Journal: SciencedirectCarlosToledoBelum ada peringkat
- Sleep Medicine: Jonathan Kushnir, Avi SadehDokumen5 halamanSleep Medicine: Jonathan Kushnir, Avi SadehCuidar para CrescerBelum ada peringkat
- Jurnal Keperawatan AnakDokumen7 halamanJurnal Keperawatan AnakMuhammad FirdausBelum ada peringkat
- Sleep Study InterpretationDokumen4 halamanSleep Study InterpretationgreenBelum ada peringkat
- Aindev 2012 12 004Dokumen10 halamanAindev 2012 12 004Gisele Elise MeninBelum ada peringkat
- Evaluation of Sleep Disturbances in Children With Epilepsy A Questionnaire BasedDokumen4 halamanEvaluation of Sleep Disturbances in Children With Epilepsy A Questionnaire BasednoiBelum ada peringkat
- Richdale - 1999 - Sleep Problems in Autism Prevalence, Cause, and IDokumen7 halamanRichdale - 1999 - Sleep Problems in Autism Prevalence, Cause, and IlinhhkngBelum ada peringkat
- cYCLIC ALTERNATING PATTERN IN INFNATS WITH CONGENITAL HYPOTHYROIDISM RAFA SANTANA GERARDO ALVARADODokumen6 halamancYCLIC ALTERNATING PATTERN IN INFNATS WITH CONGENITAL HYPOTHYROIDISM RAFA SANTANA GERARDO ALVARADOGerardo Alvarado RuizBelum ada peringkat
- ADHD Treatments Impact on SleepDokumen9 halamanADHD Treatments Impact on SleepAlberto José Correia RamosBelum ada peringkat
- Inoue (2012) - ADHD Hemodynamic Response Go:NoGo & FNIRSDokumen6 halamanInoue (2012) - ADHD Hemodynamic Response Go:NoGo & FNIRSddb5013Belum ada peringkat
- Excessive Daytime Sleepiness and Epilepsy A SystemDokumen10 halamanExcessive Daytime Sleepiness and Epilepsy A Systemkano bhavBelum ada peringkat
- Polysomnographic Aspects of Sleep Architecture On Self-Limited Epilepsy With Centrotemporal Spikes: A Systematic Review and Meta-AnalysisDokumen7 halamanPolysomnographic Aspects of Sleep Architecture On Self-Limited Epilepsy With Centrotemporal Spikes: A Systematic Review and Meta-AnalysisRezky 'kiki' Oktarianti SyahputriBelum ada peringkat
- Epilepsy Surgery in Children With Drug-Resistant Epilepsy, A Long-Term Follow-UpDokumen9 halamanEpilepsy Surgery in Children With Drug-Resistant Epilepsy, A Long-Term Follow-UpPutri IlhamiBelum ada peringkat
- CSHQDokumen11 halamanCSHQRiffq Rambu AnarkiBelum ada peringkat
- Protective and Risk Factors For Adolescent Sleep - A Meta-Analytic ReviewDokumen14 halamanProtective and Risk Factors For Adolescent Sleep - A Meta-Analytic ReviewJust a GirlBelum ada peringkat
- Sleep Problems in Children With Attention Deficit/Hyperactivity Disorder: Current Status of Knowledge and Appropriate ManagementDokumen9 halamanSleep Problems in Children With Attention Deficit/Hyperactivity Disorder: Current Status of Knowledge and Appropriate ManagementGisele Elise MeninBelum ada peringkat
- Medsci 06 00072Dokumen12 halamanMedsci 06 00072neiralejandroblpBelum ada peringkat
- The Relationship Between Sleep Problems and Neuropsychological FunctioningDokumen7 halamanThe Relationship Between Sleep Problems and Neuropsychological FunctioningnoiBelum ada peringkat
- J Ejpn 2016 07 004Dokumen13 halamanJ Ejpn 2016 07 004Gisele Elise MeninBelum ada peringkat
- Abnormal Sleep Physiology in Children With 15q11.2-13.1 Duplication (Dup15q) SyndromeDokumen14 halamanAbnormal Sleep Physiology in Children With 15q11.2-13.1 Duplication (Dup15q) SyndromeAmr Mohamed GalalBelum ada peringkat
- Co Sleeping Research PaperDokumen6 halamanCo Sleeping Research Paperh02ngq6c100% (1)
- life-14-00480Dokumen13 halamanlife-14-00480Shahmeer HassanBelum ada peringkat
- 1 s2.0 S1389945721002380 MainDokumen9 halaman1 s2.0 S1389945721002380 MainHafizhah AlhusnaBelum ada peringkat
- SMD in EpilepsyDokumen11 halamanSMD in EpilepsyAndriani KhairunnisaBelum ada peringkat
- Chine WU - 2017Dokumen8 halamanChine WU - 2017Wil HelmBelum ada peringkat
- UntitledDokumen19 halamanUntitledJOÃO PEDRO DE SOUSA PALMEIRABelum ada peringkat
- 1 s2.0 S1087079213000440 MainDokumen13 halaman1 s2.0 S1087079213000440 Mainm67arthaBelum ada peringkat
- Gale Researcher Guide for: Sleep Disorders and Their TreatmentDari EverandGale Researcher Guide for: Sleep Disorders and Their TreatmentBelum ada peringkat
- Sllep AssessmenDokumen5 halamanSllep AssessmenSyairah Banu DjufriBelum ada peringkat
- ECON2020 Brochure 20190731 02 PDFDokumen8 halamanECON2020 Brochure 20190731 02 PDFSyairah Banu DjufriBelum ada peringkat
- Medicine As Our Liberal Arts: Gilberto Ka Kit LeungDokumen2 halamanMedicine As Our Liberal Arts: Gilberto Ka Kit LeungSyairah Banu DjufriBelum ada peringkat
- Choi2012 SLEDokumen7 halamanChoi2012 SLESyairah Banu DjufriBelum ada peringkat
- Why a Liberal Arts Education Teaches You to Think, Learn, and See the WholeDokumen9 halamanWhy a Liberal Arts Education Teaches You to Think, Learn, and See the WholeSyairah Banu DjufriBelum ada peringkat
- CN 3 4 6Dokumen4 halamanCN 3 4 6Syairah Banu DjufriBelum ada peringkat
- Activacion de Office 2016Dokumen1 halamanActivacion de Office 2016Luz VasquezBelum ada peringkat
- Vertigo - p244Dokumen8 halamanVertigo - p244familyman80Belum ada peringkat
- SDSC Eng ColourDokumen2 halamanSDSC Eng ColourmerawatidyahsepitaBelum ada peringkat
- Across The Consciousness Continuum-From Unresponsive Wakefulness To SleepDokumen15 halamanAcross The Consciousness Continuum-From Unresponsive Wakefulness To SleepSyairah Banu DjufriBelum ada peringkat
- OutputDokumen1 halamanOutputSyairah Banu DjufriBelum ada peringkat
- DataSet1Dokumen30 halamanDataSet1Syairah Banu DjufriBelum ada peringkat
- DataSet1Dokumen30 halamanDataSet1Syairah Banu DjufriBelum ada peringkat
- Antimikroba StrategiDokumen13 halamanAntimikroba StrategiSyairah Banu DjufriBelum ada peringkat
- Deep Tendon ReflexesDokumen9 halamanDeep Tendon ReflexesSyairah Banu DjufriBelum ada peringkat
- Which Electroencephalogram Patterns Are Commonly Misread As Epileptiform?Dokumen4 halamanWhich Electroencephalogram Patterns Are Commonly Misread As Epileptiform?Syairah Banu DjufriBelum ada peringkat
- Lumbosacral Spinalcord CompressionDokumen13 halamanLumbosacral Spinalcord CompressionSyairah Banu DjufriBelum ada peringkat
- Movement DisordersDokumen5 halamanMovement DisordersSyairah Banu DjufriBelum ada peringkat
- Principle of The Head Impulse (Thrust) Test or Halmagyi Head Thrust Test (HHTT)Dokumen3 halamanPrinciple of The Head Impulse (Thrust) Test or Halmagyi Head Thrust Test (HHTT)Syairah Banu DjufriBelum ada peringkat
- Use Seat Belts to Stay SafeDokumen5 halamanUse Seat Belts to Stay SafeSyairah Banu DjufriBelum ada peringkat
- BMJB 5569Dokumen7 halamanBMJB 5569Syairah Banu DjufriBelum ada peringkat
- Intensive Care Med-The Berlin Definition of ARDSDokumen10 halamanIntensive Care Med-The Berlin Definition of ARDSSyairah Banu DjufriBelum ada peringkat
- Treatment Completion and Costs of A Randomized Trial of Rifampin For 4 Months Versus Isoniazid For 9 MonthsDokumen5 halamanTreatment Completion and Costs of A Randomized Trial of Rifampin For 4 Months Versus Isoniazid For 9 MonthsSyairah Banu DjufriBelum ada peringkat
- Hyper Tiro I DismDokumen25 halamanHyper Tiro I DismSyairah Banu DjufriBelum ada peringkat
- ANS Evidence Based Guidelines Rev-4Dokumen7 halamanANS Evidence Based Guidelines Rev-4Syairah Banu DjufriBelum ada peringkat
- ARIAReport 2010Dokumen153 halamanARIAReport 2010Syairah Banu DjufriBelum ada peringkat
- N C C N D: Ursing ARE OF Lients With Eurologic IsordersDokumen96 halamanN C C N D: Ursing ARE OF Lients With Eurologic IsordersMatt Lao DionelaBelum ada peringkat
- Neurotransmitter ChartDokumen1 halamanNeurotransmitter ChartEduardo LauandeBelum ada peringkat
- MS2 - Neurologic Disorder My ReportDokumen30 halamanMS2 - Neurologic Disorder My ReportNeil Lansang BallobanBelum ada peringkat
- Chirp ABR - Gsi James HallDokumen42 halamanChirp ABR - Gsi James HallPamela Tamara Fernández EscobarBelum ada peringkat
- Faktor PICODokumen1 halamanFaktor PICOAlldo SaodalaBelum ada peringkat
- Kochi EchsDokumen10 halamanKochi EchsDeepak KarnavarBelum ada peringkat
- CRANIOTOMYDokumen59 halamanCRANIOTOMYJhay LawrenceBelum ada peringkat
- Anatomy of Ear.Dokumen14 halamanAnatomy of Ear.Shimmering MoonBelum ada peringkat
- Fracp Past Papers - NeurologyDokumen21 halamanFracp Past Papers - NeurologyLakshya J BasumataryBelum ada peringkat
- Restless Leg SyndromeDokumen2 halamanRestless Leg Syndromeshinobi200Belum ada peringkat
- The OSCE OrientationDokumen25 halamanThe OSCE OrientationginadaisluBelum ada peringkat
- Hypothalamus, Limbic System, and Memory RegulationDokumen71 halamanHypothalamus, Limbic System, and Memory RegulationvinodksahuBelum ada peringkat
- Eye Movement Control and the Role of the Superior ColliculiDokumen10 halamanEye Movement Control and the Role of the Superior ColliculiDavis KallanBelum ada peringkat
- The Neuropsychiatry of EpilepsyDokumen361 halamanThe Neuropsychiatry of Epilepsypablo_zabala100% (3)
- VEDA Patient Medical History Form - LongDokumen3 halamanVEDA Patient Medical History Form - LongyaddBelum ada peringkat
- Empanelled HospitalsDokumen14 halamanEmpanelled HospitalsSwaroopVishnuBelum ada peringkat
- Geriatric OSCE Stroke ExamDokumen2 halamanGeriatric OSCE Stroke ExamAmi FebrizaBelum ada peringkat
- Neurologic Music Therapy in Cognitive RehabilitationDokumen7 halamanNeurologic Music Therapy in Cognitive Rehabilitationisaacelias2509Belum ada peringkat
- 31.1 The NeuronDokumen33 halaman31.1 The Neuronmoniaguayo98Belum ada peringkat
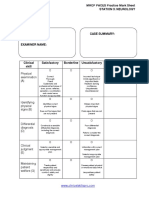
- Station 3 Neurology MRCP PACES Mark SheetDokumen1 halamanStation 3 Neurology MRCP PACES Mark SheetdoctorebrahimBelum ada peringkat
- Handbook of Neurologic Rating Scales 2nd EdnDokumen2 halamanHandbook of Neurologic Rating Scales 2nd Ednsivag1451999Belum ada peringkat
- Nervous System Chapter EssentialsDokumen19 halamanNervous System Chapter EssentialsAeren RhosenBelum ada peringkat
- PG Prospectus 2021Dokumen41 halamanPG Prospectus 2021Amy LalringhluaniBelum ada peringkat
- Chapter 5neonatal Seizures and Neonatal SyndromesDokumen10 halamanChapter 5neonatal Seizures and Neonatal SyndromesArista RiskaBelum ada peringkat
- Cervical Dystonia Supplement - Summer 08Dokumen8 halamanCervical Dystonia Supplement - Summer 08Kelly PhillipsBelum ada peringkat
- Physical Disability LearnersDokumen25 halamanPhysical Disability LearnersChristian Luis De GuzmanBelum ada peringkat
- CholesteatomaDokumen13 halamanCholesteatomaKing KaruBelum ada peringkat