Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- CASE STUDY 10 NCPDokumen46 halamanCASE STUDY 10 NCPRosemarie R. Reyes100% (8)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Child Protection Training ManualDokumen229 halamanChild Protection Training Manualbabuin1Belum ada peringkat
- Women and Mental HealthDokumen74 halamanWomen and Mental Healthmerin sunilBelum ada peringkat
- WHO Complete Hiv Report2009Dokumen150 halamanWHO Complete Hiv Report2009danayanto sumbungBelum ada peringkat
- ABC of Intensive CareDokumen49 halamanABC of Intensive CareCurro MirallesBelum ada peringkat
- Bab 198 Penggunaan Anti KoagulanDokumen4 halamanBab 198 Penggunaan Anti KoagulanRaja Alfian IrawanBelum ada peringkat
- Update On ART-2010Dokumen30 halamanUpdate On ART-2010danayanto sumbungBelum ada peringkat
- NVP Toxicity in Pregnant WomenDokumen5 halamanNVP Toxicity in Pregnant Womendanayanto sumbungBelum ada peringkat
- Art 1Dokumen11 halamanArt 1danayanto sumbungBelum ada peringkat
- 4-Mycobacterium Infection and HIVDokumen45 halaman4-Mycobacterium Infection and HIVdanayanto sumbungBelum ada peringkat
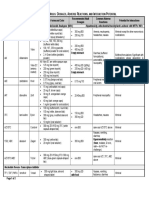
- Antiretroviral Drug Table - Dosages, Adverse Reactions, and Interaction PotentialDokumen2 halamanAntiretroviral Drug Table - Dosages, Adverse Reactions, and Interaction Potentialdanayanto sumbungBelum ada peringkat
- 15 High Rate of Early Virological FailureDokumen9 halaman15 High Rate of Early Virological Failuredanayanto sumbungBelum ada peringkat
- AIDS Clinical CareDokumen8 halamanAIDS Clinical Caredanayanto sumbungBelum ada peringkat
- 07 Antiretroviral Drug InteractionsDokumen14 halaman07 Antiretroviral Drug Interactionsdanayanto sumbungBelum ada peringkat
- 4-Mycobacterium Infection and HIVDokumen45 halaman4-Mycobacterium Infection and HIVdanayanto sumbungBelum ada peringkat
- Low Cost Thermal Camera For Use in Preclinical Detection of Diabetic PeripheralDokumen8 halamanLow Cost Thermal Camera For Use in Preclinical Detection of Diabetic PeripheralEDGAR ISMAEL REYES DEZABelum ada peringkat
- Plant Pathogens andDokumen3 halamanPlant Pathogens andPrashant Waghrulkar100% (1)
- Constipation 508Dokumen12 halamanConstipation 508Shishir Kumar SinghBelum ada peringkat
- Nu 712 Health DisparitiesDokumen5 halamanNu 712 Health Disparitiesapi-555218722Belum ada peringkat
- Surgery Toacs APRIL 2012: Hassaan Bari Aga Khan UniversityDokumen18 halamanSurgery Toacs APRIL 2012: Hassaan Bari Aga Khan UniversitySyedBelum ada peringkat
- What Are CarbohydratesDokumen36 halamanWhat Are CarbohydratesPINNACLE CAFEBelum ada peringkat
- Employers Guide - InteractiveDokumen24 halamanEmployers Guide - Interactiveapi-285398586Belum ada peringkat
- Rufenal EmulgelDokumen2 halamanRufenal EmulgelDr.2020Belum ada peringkat
- Hematologic Disorders: JeffreyDokumen582 halamanHematologic Disorders: JeffreyPalak GuptaBelum ada peringkat
- General Profile: - Pa - 6mos Old - Female - Filipino - Roman Catholic - Alang-Alang Mandaue CityDokumen18 halamanGeneral Profile: - Pa - 6mos Old - Female - Filipino - Roman Catholic - Alang-Alang Mandaue CityRj FornollesBelum ada peringkat
- Semey State Medical University: Department of Psychiatry Topic Schizophrenia Raja Ali HassanDokumen45 halamanSemey State Medical University: Department of Psychiatry Topic Schizophrenia Raja Ali HassanRaja HassanBelum ada peringkat
- Transforming Growth Factor Beta TGFBDokumen8 halamanTransforming Growth Factor Beta TGFBxxxxxxxBelum ada peringkat
- Msds Quik Gel Gold PDFDokumen10 halamanMsds Quik Gel Gold PDFBangun KartaBelum ada peringkat
- Encouraging TeenagersDokumen17 halamanEncouraging TeenagersTahBelum ada peringkat
- Rodríguez DinamometríaDokumen5 halamanRodríguez DinamometríaMariana Covarrubias SalazarBelum ada peringkat
- Hepatic Encephalopathy and DkaDokumen6 halamanHepatic Encephalopathy and Dkajames garciaBelum ada peringkat
- A Proposed Pediatric Medical Center Research ThesisDokumen3 halamanA Proposed Pediatric Medical Center Research ThesisMarielle AbanteBelum ada peringkat
- Adrenal FatigueDokumen40 halamanAdrenal FatigueNimmi Nims67% (3)
- Animal Genetic Engineering 110816 (1) Unit 4Dokumen29 halamanAnimal Genetic Engineering 110816 (1) Unit 4Rupal ChoudharyBelum ada peringkat
- Bioaktivni Ugljenihidrati PDFDokumen4 halamanBioaktivni Ugljenihidrati PDFmajabulatBelum ada peringkat
- Excel Dentistry 3rd Year Sample 2022Dokumen25 halamanExcel Dentistry 3rd Year Sample 2022Mohammed hisham khanBelum ada peringkat
- DNS ENT Case Write UpDokumen8 halamanDNS ENT Case Write UpShafiq ZahariBelum ada peringkat
- Circulatory Disease ProjectDokumen2 halamanCirculatory Disease Projectapi-517831630Belum ada peringkat
- Challenges of Catholic Doctors in The Changing World - 15th AFCMA Congress 2012Dokumen218 halamanChallenges of Catholic Doctors in The Changing World - 15th AFCMA Congress 2012Komsos - AG et al.Belum ada peringkat
- GB PerforationDokumen13 halamanGB Perforationmudasir61Belum ada peringkat
- # Category Image Product Name Producer Package Hs Code Remark Key FeaturesDokumen9 halaman# Category Image Product Name Producer Package Hs Code Remark Key Featuresiq_dianaBelum ada peringkat
- Artemisia Vulgaris MonographDokumen4 halamanArtemisia Vulgaris MonographEmer BonesBelum ada peringkat