Anda mungkin juga menyukai
- Basel Statements Implementation in Indonesia - RevDokumen37 halamanBasel Statements Implementation in Indonesia - Revtri lestari100% (2)
- Ch013 001-007 HypertensionDokumen7 halamanCh013 001-007 Hypertensiond_94100% (5)
- General Surgery Board-Final Written Exam Blueprint v.1Dokumen3 halamanGeneral Surgery Board-Final Written Exam Blueprint v.1Mohammed S. Al GhamdiBelum ada peringkat
- Performative Peritonitis PDFDokumen7 halamanPerformative Peritonitis PDFJACOB LEO SunnyBelum ada peringkat
- CCO Cytokine TX in MM ExpressPointsDokumen18 halamanCCO Cytokine TX in MM ExpressPointsveaceslav coscodanBelum ada peringkat
- Bionikk Lancet 2022 VanoDokumen13 halamanBionikk Lancet 2022 VanomarieBelum ada peringkat
- FTPDokumen5 halamanFTPHaya RihanBelum ada peringkat
- A Case Series of Metastatic Lateral Cervical LymphadenopathyDokumen5 halamanA Case Series of Metastatic Lateral Cervical LymphadenopathyKriti KumariBelum ada peringkat
- Original Research PaperDokumen4 halamanOriginal Research PaperDr SrigopalBelum ada peringkat
- Selvarajah 2013Dokumen7 halamanSelvarajah 2013Sol LakosBelum ada peringkat
- Journal Homepage: - : Manuscript HistoryDokumen10 halamanJournal Homepage: - : Manuscript HistoryIJAR JOURNALBelum ada peringkat
- Influence of Renal Function On The Pharmacokinetics of Piperacillin Tazobactam in Intensive CareDokumen10 halamanInfluence of Renal Function On The Pharmacokinetics of Piperacillin Tazobactam in Intensive CareLuciana OliveiraBelum ada peringkat
- Challenges of Viral Hepatitis Treatment in EthiopiaDokumen16 halamanChallenges of Viral Hepatitis Treatment in EthiopiaEleni HagosBelum ada peringkat
- A Study On The Efficacy of Immunotherapy With Purified Protein Derivative For The Treatment of Recalcitrant WartsDokumen5 halamanA Study On The Efficacy of Immunotherapy With Purified Protein Derivative For The Treatment of Recalcitrant WartsAlfian Faisal Abu JusufBelum ada peringkat
- Topalian JCDokumen30 halamanTopalian JCPhilippe PetitBelum ada peringkat
- Challenges in VH Treatment: Fmoh 2021Dokumen17 halamanChallenges in VH Treatment: Fmoh 2021Eleni HagosBelum ada peringkat
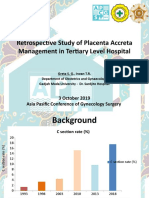
- 2.dr. Greta - Apcgs GreDokumen19 halaman2.dr. Greta - Apcgs GrecirererereBelum ada peringkat
- A Study of Haematological Profile of Malaria in A Tertiary Care Centre of Western Uttar Pradesh, IndiaDokumen5 halamanA Study of Haematological Profile of Malaria in A Tertiary Care Centre of Western Uttar Pradesh, IndiaramperoughBelum ada peringkat
- A Clinical Study of Abdominal Wound DehiscenceDokumen25 halamanA Clinical Study of Abdominal Wound DehiscenceKarthikeyan RBelum ada peringkat
- Jeevan Rekha - A Counter For Hepatitis C Epidemic in HaryanaDokumen41 halamanJeevan Rekha - A Counter For Hepatitis C Epidemic in HaryanaNeha Saluja100% (1)
- ACPGBI Anal CaDokumen16 halamanACPGBI Anal CaNevilleBelum ada peringkat
- Agnes Lee Thrombosis PresentationDokumen37 halamanAgnes Lee Thrombosis Presentationari naBelum ada peringkat
- Penetalaksanaan Syok (Rizki Devita Roshella)Dokumen9 halamanPenetalaksanaan Syok (Rizki Devita Roshella)rizki devta roshellaiBelum ada peringkat
- Dermatologic Therapy Volume Issue 2020 (Doi 10.1111 - dth.13488) Keeling, Elizabeth Daly, Selene McKenna, Dermot B. - Dermatology Patientsâ - Knowledge and Concerns Regarding Their ImmunomodulatoryDokumen8 halamanDermatologic Therapy Volume Issue 2020 (Doi 10.1111 - dth.13488) Keeling, Elizabeth Daly, Selene McKenna, Dermot B. - Dermatology Patientsâ - Knowledge and Concerns Regarding Their ImmunomodulatoryJoBelum ada peringkat
- Fphar 13 970978Dokumen7 halamanFphar 13 970978Claudiu PopescuBelum ada peringkat
- Early Breast Cancer Prognostic Options Including CanAssistDokumen49 halamanEarly Breast Cancer Prognostic Options Including CanAssistIndranil GhoshBelum ada peringkat
- Icu Clinical Audit of Month of April 2021 G.C: Prepared By:dr Nigat Endalamaw Emccr2 Moderator:Dr AyalewDokumen57 halamanIcu Clinical Audit of Month of April 2021 G.C: Prepared By:dr Nigat Endalamaw Emccr2 Moderator:Dr AyalewalexBelum ada peringkat
- Hodgkin LymphomaDokumen32 halamanHodgkin LymphomaAndi SusiloBelum ada peringkat
- Moderate and Extreme HypofractionationDokumen32 halamanModerate and Extreme HypofractionationsamuelfsjBelum ada peringkat
- Advanced-Stagehodgkinlymphoma: by Joseph M. Connors, MDDokumen5 halamanAdvanced-Stagehodgkinlymphoma: by Joseph M. Connors, MDJOHN LOPERABelum ada peringkat
- Ca SekumDokumen7 halamanCa SekumNely M. RosyidiBelum ada peringkat
- Rce0321 Diop Cinv Webinar - FinalDokumen48 halamanRce0321 Diop Cinv Webinar - Finalamaal ramadanBelum ada peringkat
- Drainage of Malignant Ascites: Patient Selection and PerspectivesDokumen16 halamanDrainage of Malignant Ascites: Patient Selection and PerspectivesimadearyBelum ada peringkat
- 1007-Article Text-2245-1-10-20200320Dokumen4 halaman1007-Article Text-2245-1-10-20200320Savitri IndrasariBelum ada peringkat
- Risk Factors and Clinical Evaluation of Haemorrhoids in A Rural Medical CollegeDokumen3 halamanRisk Factors and Clinical Evaluation of Haemorrhoids in A Rural Medical CollegenessBelum ada peringkat
- Comprehensive Surgical Staging For Endometrial Cancer: Management ReviewDokumen7 halamanComprehensive Surgical Staging For Endometrial Cancer: Management ReviewAji PatriajatiBelum ada peringkat
- Endoscopic Interventional Management Using Adrenaline-Normal Saline Injection For Actively Bleeding Peptic Ulcers in South Kashmir, IndiaDokumen6 halamanEndoscopic Interventional Management Using Adrenaline-Normal Saline Injection For Actively Bleeding Peptic Ulcers in South Kashmir, IndiaIJAR JOURNALBelum ada peringkat
- For Hepatocellular Carcinoma: Living Donor Liver TransplantationDokumen46 halamanFor Hepatocellular Carcinoma: Living Donor Liver TransplantationtasarimkutusuBelum ada peringkat
- Jumlah Kasus Preeklampsia Berat Di RSUD Raden Mattaher Jambi Tahun 2014 Dan 2015Dokumen17 halamanJumlah Kasus Preeklampsia Berat Di RSUD Raden Mattaher Jambi Tahun 2014 Dan 2015Iqlima Khairiyah PutriBelum ada peringkat
- Early Ovarian Cancer PDFDokumen5 halamanEarly Ovarian Cancer PDFAndreeaPopescuBelum ada peringkat
- MRM ArticleDokumen5 halamanMRM ArticleRekha Tulsi KhatriBelum ada peringkat
- Standard Treatment Guidelines Oncology: Ministry of Health & Family Welfare Govt. of IndiaDokumen138 halamanStandard Treatment Guidelines Oncology: Ministry of Health & Family Welfare Govt. of IndiaTIRUCHANURUBelum ada peringkat
- 0850 Adam MED BdImYaK YG - OipkDokumen66 halaman0850 Adam MED BdImYaK YG - OipkFlaviusBelum ada peringkat
- Awad 2016Dokumen8 halamanAwad 2016PopyBelum ada peringkat
- The Study of Clinico-Aetiological Profile of Pancytopenia in Elderly PDFDokumen3 halamanThe Study of Clinico-Aetiological Profile of Pancytopenia in Elderly PDFKaye Antonette AntioquiaBelum ada peringkat
- 10 Mcqs in Epidemiology: Anish Dhakal (Aryan)Dokumen13 halaman10 Mcqs in Epidemiology: Anish Dhakal (Aryan)lmoiefrBelum ada peringkat
- Diagnosis and Features of Hospital-Acquired Pneumonia: A Retrospective Cohort StudyDokumen7 halamanDiagnosis and Features of Hospital-Acquired Pneumonia: A Retrospective Cohort Studytitan dheaBelum ada peringkat
- The Impact of Absolute CD4 Count and Percentage Discordance On Pneumocystis Jirovecii Pneumonia Prophylaxis in HIV-Infected PatientsDokumen4 halamanThe Impact of Absolute CD4 Count and Percentage Discordance On Pneumocystis Jirovecii Pneumonia Prophylaxis in HIV-Infected PatientsNazliah SyarbinBelum ada peringkat
- CPG Gyne VulvarDokumen9 halamanCPG Gyne Vulvarpuji arisBelum ada peringkat
- Recidiva in Tumorile LaringieneDokumen9 halamanRecidiva in Tumorile LaringieneAlex VesaBelum ada peringkat
- Study of Clinical Profile, Risk-Factors and Management of Post Partum Haemorrhage in A Tertiary Care CentreDokumen5 halamanStudy of Clinical Profile, Risk-Factors and Management of Post Partum Haemorrhage in A Tertiary Care CentreIJAR JOURNALBelum ada peringkat
- Berapa Lama Follow UpDokumen6 halamanBerapa Lama Follow UparifBelum ada peringkat
- Volume4 Issue3 May Jun No.450 426 432Dokumen7 halamanVolume4 Issue3 May Jun No.450 426 432Yoga ABelum ada peringkat
- If HP Cancer Guide BMT ManualDokumen363 halamanIf HP Cancer Guide BMT ManualZardar KBelum ada peringkat
- Surgical Treatment of Intrahepatic Cholangiocarcinoma: A Retrospective Cohort StudyDokumen21 halamanSurgical Treatment of Intrahepatic Cholangiocarcinoma: A Retrospective Cohort StudyHendry DimasBelum ada peringkat
- Jco 2005 06 084Dokumen6 halamanJco 2005 06 084Nurul SafitriBelum ada peringkat
- Weledji 2020Dokumen7 halamanWeledji 2020Felipe CarmonaBelum ada peringkat
- Guidelines For The Diagnosis and Management of Vulval CarcinomaDokumen35 halamanGuidelines For The Diagnosis and Management of Vulval CarcinomaThar Htay SanBelum ada peringkat
- 1 s2.0 S2049080122014534 MainDokumen5 halaman1 s2.0 S2049080122014534 MainEleonore Marcelle Akissi Agni Ola SourouppPBelum ada peringkat
- Outcome of Patients Undergoing Amputation For Diabetic Foot UlcerDokumen4 halamanOutcome of Patients Undergoing Amputation For Diabetic Foot UlcerrischaBelum ada peringkat
- Top Trials in Gastroenterology & HepatologyDari EverandTop Trials in Gastroenterology & HepatologyPenilaian: 4.5 dari 5 bintang4.5/5 (7)
- On CPRDokumen32 halamanOn CPRPiyush Dutta100% (1)
- CMS Survey ProcessDokumen16 halamanCMS Survey Processyanuar esthoBelum ada peringkat
- Catheter WiresDokumen56 halamanCatheter WiresSaud ShirwanBelum ada peringkat
- Cardiac Rehab NewDokumen12 halamanCardiac Rehab NewRudra Das100% (1)
- Vital SignsDokumen10 halamanVital SignsBiway RegalaBelum ada peringkat
- The Vijayanagar Empire History Project Class 12 C 2Dokumen4 halamanThe Vijayanagar Empire History Project Class 12 C 2vanshchitkara2Belum ada peringkat
- Ventricular Septal Defects in AdultsDokumen13 halamanVentricular Septal Defects in AdultsМихаил НеболеевBelum ada peringkat
- The Effects of Noise Pollution To Your HealthDokumen8 halamanThe Effects of Noise Pollution To Your HealthMr UIBelum ada peringkat
- Orthostatic ToleranceDokumen3 halamanOrthostatic Tolerancehajar ahmadBelum ada peringkat
- Measuring BPDokumen39 halamanMeasuring BPMaaz KhanBelum ada peringkat
- Amlodipine Drug StudyDokumen1 halamanAmlodipine Drug Studyjuan carlosBelum ada peringkat
- Rotarex IFUDokumen5 halamanRotarex IFURemon NassimBelum ada peringkat
- Pat Physical Readiness QuestionareDokumen1 halamanPat Physical Readiness Questionarejohn jaycoh veranoBelum ada peringkat
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDokumen1 halamanAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityChris LeeBelum ada peringkat
- Focus:: Canossa CollegeDokumen23 halamanFocus:: Canossa CollegeZyrene RiveraBelum ada peringkat
- Examenul Clinic Al MainiiDokumen33 halamanExamenul Clinic Al MainiiAdina Botez100% (2)
- Damage Control ResuscitationDokumen32 halamanDamage Control Resuscitationrima oktariniBelum ada peringkat
- Acute Stroke ManagementDokumen8 halamanAcute Stroke ManagementГурам ЧахвадзеBelum ada peringkat
- Acute Coronary SyndromeDokumen8 halamanAcute Coronary SyndromeAb90 SBelum ada peringkat
- Pulmonary EmbolismDokumen23 halamanPulmonary EmbolismBianca Dizon0% (1)
- Keywords:-STS Score, MACE, CABGDokumen6 halamanKeywords:-STS Score, MACE, CABGInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Republic of Iraq: Medical DevicesDokumen5 halamanRepublic of Iraq: Medical Devicesالحارث فخري فياض احمدBelum ada peringkat
- Hs Ts PALSDokumen1 halamanHs Ts PALSTeresa GonzálezBelum ada peringkat
- Heart BlockDokumen17 halamanHeart Blocklitan dasBelum ada peringkat
- Atrial Fibrillation Case PresentationDokumen12 halamanAtrial Fibrillation Case PresentationSweet HusainBelum ada peringkat
- Rigel Uni Sim Lite DatasheetDokumen5 halamanRigel Uni Sim Lite Datasheetmailalexmd.vrn.ruBelum ada peringkat
- Coronary Artery Disease & Hypertension Practice Quiz (50 Questions)Dokumen18 halamanCoronary Artery Disease & Hypertension Practice Quiz (50 Questions)Erica Veluz LuyunBelum ada peringkat
- ECG Test ProcedureDokumen3 halamanECG Test ProcedureDede IyyaBelum ada peringkat
- Writing A Simulation Scenario: A Step-By-Step Guide: Deborah Bambini, PHD, WHNP-BC, Cne, ChseDokumen10 halamanWriting A Simulation Scenario: A Step-By-Step Guide: Deborah Bambini, PHD, WHNP-BC, Cne, ChseEsteban RamosBelum ada peringkat