Anda mungkin juga menyukai
- Ijhbr January 2018 23-30Dokumen8 halamanIjhbr January 2018 23-30farhanomeBelum ada peringkat
- Deep Venous Thrombosis After Percutaneous Insertion of Vena Caval FiltersDokumen9 halamanDeep Venous Thrombosis After Percutaneous Insertion of Vena Caval Filtersari kurniawanBelum ada peringkat
- Ijvm2014 531689 PDFDokumen6 halamanIjvm2014 531689 PDFReka HariskianaBelum ada peringkat
- Jurnal VaskularDokumen5 halamanJurnal VaskulardrelvBelum ada peringkat
- Tugas Praktikum SpssDokumen2 halamanTugas Praktikum SpssjunBelum ada peringkat
- Deep Vein Thrombosis (DVT) Is A Precursor of Potentially Fatal PulmonaryDokumen4 halamanDeep Vein Thrombosis (DVT) Is A Precursor of Potentially Fatal PulmonaryHatem ShafelBelum ada peringkat
- Early Follow-Up and Treatment Recommendations For Isolated Calf Deep Venous ThrombosisDokumen5 halamanEarly Follow-Up and Treatment Recommendations For Isolated Calf Deep Venous ThrombosisDr. Aditya ShindeBelum ada peringkat
- The Importance of Monophasic Doppler Waveforms in The Common Femoral VeinDokumen7 halamanThe Importance of Monophasic Doppler Waveforms in The Common Femoral Veindgina8800Belum ada peringkat
- LnnkomplikacijeDokumen8 halamanLnnkomplikacijeVinko GrubišićBelum ada peringkat
- Detection of Unsuspected Pelvic Dvts On Abdominopelvic CT Scans: A Potentially Life-Saving DiagnosisDokumen5 halamanDetection of Unsuspected Pelvic Dvts On Abdominopelvic CT Scans: A Potentially Life-Saving DiagnosisKumail KhandwalaBelum ada peringkat
- 2014 - Jonathan Caronia - Residentperformedtwopointcompressionultrasoundisin (Retrieved-2015!10!13)Dokumen5 halaman2014 - Jonathan Caronia - Residentperformedtwopointcompressionultrasoundisin (Retrieved-2015!10!13)Ali MullaBelum ada peringkat
- Venous Thromboembolism in Patients Discharged From The Emergency Department With Ankle FracturesDokumen13 halamanVenous Thromboembolism in Patients Discharged From The Emergency Department With Ankle FracturesSebastiano Della CasaBelum ada peringkat
- 2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathyDokumen9 halaman2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathybanupluBelum ada peringkat
- Dutta 2017Dokumen3 halamanDutta 2017Kartik DuttaBelum ada peringkat
- JHM 2112Dokumen4 halamanJHM 2112senkonenBelum ada peringkat
- 1 s2.0 S0378603X14001053 MainDokumen10 halaman1 s2.0 S0378603X14001053 MainAdrian PachecoBelum ada peringkat
- DVT in India PDFDokumen6 halamanDVT in India PDFKarthik KoneruBelum ada peringkat
- Arenas-Jiménez2000 Article EvaluationOfCTFindingsForDiagnDokumen10 halamanArenas-Jiménez2000 Article EvaluationOfCTFindingsForDiagnJulieta RGBelum ada peringkat
- Guidelines On Travel-Related Venous Thrombosis: GuidelineDokumen4 halamanGuidelines On Travel-Related Venous Thrombosis: GuidelineNourhan JamalBelum ada peringkat
- Deep Venous Thrombosis Diferential DiagnosisDokumen8 halamanDeep Venous Thrombosis Diferential DiagnosisBeby Dwi Lestari BajryBelum ada peringkat
- Fluid Complications: Malignant Pleural EffusionDokumen11 halamanFluid Complications: Malignant Pleural Effusiont4tranBelum ada peringkat
- Computer-Assisted Transcatheter Heart Valve Implantation in Valve-in-Valve ProceduresDokumen8 halamanComputer-Assisted Transcatheter Heart Valve Implantation in Valve-in-Valve ProceduresrédaBelum ada peringkat
- Jurnal VaskularDokumen5 halamanJurnal VaskulardrelvBelum ada peringkat
- Wetenschappelijk ArtikelDokumen7 halamanWetenschappelijk Artikel5rfffgfgBelum ada peringkat
- 2137 FullDokumen7 halaman2137 FullCourtneykdBelum ada peringkat
- 5 Sagban2015Dokumen7 halaman5 Sagban2015mihaelamocanBelum ada peringkat
- Hemoptisis 1Dokumen11 halamanHemoptisis 1habiba rositaBelum ada peringkat
- Fibrinolysis Shutdown Correlation With Thromboembolic Events in Severe COVID-19 InfectionDokumen12 halamanFibrinolysis Shutdown Correlation With Thromboembolic Events in Severe COVID-19 InfectionRia GandaBelum ada peringkat
- Diagnostic Assessment BeforeDokumen4 halamanDiagnostic Assessment BeforeBinod KumarBelum ada peringkat
- Deep Vein Thrombosis in Stroke Patients:: Eulogio R. SiosonDokumen6 halamanDeep Vein Thrombosis in Stroke Patients:: Eulogio R. SiosonDianti SuryonoBelum ada peringkat
- Pan Nucci 2011Dokumen8 halamanPan Nucci 2011Ana I. NevarezBelum ada peringkat
- Diagnosis of Deep Venous Thrombosis and Pulmonary EmbolismDokumen7 halamanDiagnosis of Deep Venous Thrombosis and Pulmonary EmbolismNataly VanesaBelum ada peringkat
- Transcatheter Coil Embolotherapy: A Safe and Evective Option For Major Colonic HaemorrhageDokumen7 halamanTranscatheter Coil Embolotherapy: A Safe and Evective Option For Major Colonic Haemorrhagemuhammad gagas sasongkoBelum ada peringkat
- Blom JW - Malignancies, Prothrombotic Mutations, and The Risk of Venous ThrombosisDokumen8 halamanBlom JW - Malignancies, Prothrombotic Mutations, and The Risk of Venous ThrombosisFarid RakhmanBelum ada peringkat
- 6514 23132 1 PBDokumen3 halaman6514 23132 1 PBdewminiBelum ada peringkat
- Prospective Evaluation of Factors Associated With Early Failure of Arteriovenous Fistulae in Hemodialysis PatientsDokumen5 halamanProspective Evaluation of Factors Associated With Early Failure of Arteriovenous Fistulae in Hemodialysis PatientsIvor WilopoBelum ada peringkat
- Pulmonary EmbolismDokumen53 halamanPulmonary EmbolismSultan Al-rabeahBelum ada peringkat
- Deep Venous Thrombosis After Orthopedic PDFDokumen7 halamanDeep Venous Thrombosis After Orthopedic PDFAnh Nguyen HuuBelum ada peringkat
- Mav-Vascularização Miometrial - 2020Dokumen7 halamanMav-Vascularização Miometrial - 2020joaogualda19Belum ada peringkat
- Safety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaDokumen9 halamanSafety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaSisca Dwi AgustinaBelum ada peringkat
- Pinch Off Syndrome - A Rare Complication of Chemo Port: Dr. C. Ramachandra, Dr. Pavan Kumar J, Dr. C. SrinivasDokumen4 halamanPinch Off Syndrome - A Rare Complication of Chemo Port: Dr. C. Ramachandra, Dr. Pavan Kumar J, Dr. C. SrinivasPavan JonnadaBelum ada peringkat
- Derrame PleuralDokumen8 halamanDerrame PleuralFelipeBelum ada peringkat
- Embolization in The Management of Recurrent Secondary Post-Tonsillectomy Haemorrhage in ChildrenDokumen7 halamanEmbolization in The Management of Recurrent Secondary Post-Tonsillectomy Haemorrhage in ChildrenNicolás HenaoBelum ada peringkat
- Etiologies of Bilateral Pleural EffusionsDokumen8 halamanEtiologies of Bilateral Pleural EffusionsAlexander Lukky SugondoBelum ada peringkat
- Increased Minimum Vein Diameter On PreoperativeDokumen40 halamanIncreased Minimum Vein Diameter On PreoperativeMikael AngelooBelum ada peringkat
- Jurnal THTDokumen3 halamanJurnal THTValentina AdindaBelum ada peringkat
- HSHDDokumen193 halamanHSHDRianda AkmalBelum ada peringkat
- Artigo 3Dokumen7 halamanArtigo 3Lucas SantosBelum ada peringkat
- A 40 YearsDokumen9 halamanA 40 YearsDra Mariana Huerta CampaBelum ada peringkat
- Radial Artery Access For Peripheral Endovascular ProceduresDokumen6 halamanRadial Artery Access For Peripheral Endovascular Proceduresvam buddhaBelum ada peringkat
- Thromboprohylaxis and DVT in Surgical PRDokumen7 halamanThromboprohylaxis and DVT in Surgical PRAhmed MohammedBelum ada peringkat
- Primary and Staged Transposition Arteriovenous Fistulas (Superficialization)Dokumen5 halamanPrimary and Staged Transposition Arteriovenous Fistulas (Superficialization)Anonymous LnWIBo1GBelum ada peringkat
- Value of Red Blood Cell Distribution Width On Emergency Department Admission in Patients With Venous ThrombosisDokumen6 halamanValue of Red Blood Cell Distribution Width On Emergency Department Admission in Patients With Venous ThrombosisJicko Street HooligansBelum ada peringkat
- Doipdf10 11771358863X10391355Dokumen9 halamanDoipdf10 11771358863X10391355g2rpt6nzvnBelum ada peringkat
- Deep Venous Thrombosis After Total Joint ArthroplastyDokumen7 halamanDeep Venous Thrombosis After Total Joint ArthroplastyJesse CusterBelum ada peringkat
- Chandra 2013Dokumen5 halamanChandra 2013Jose YoveraBelum ada peringkat
- First-Line Arteriovenous Access and Risks of Hospitalization and Death in Patients Starting Hemodialysis - A Nationwide Cohort StudyDokumen34 halamanFirst-Line Arteriovenous Access and Risks of Hospitalization and Death in Patients Starting Hemodialysis - A Nationwide Cohort StudyJimenez-Espinosa JeffersonBelum ada peringkat
- Complications Associated With Ivanissevich PDFDokumen3 halamanComplications Associated With Ivanissevich PDFTahir TahirBelum ada peringkat
- Transcatheter Aortic Valve Replacement: A How-to Guide for Cardiologists and Cardiac SurgeonsDari EverandTranscatheter Aortic Valve Replacement: A How-to Guide for Cardiologists and Cardiac SurgeonsBelum ada peringkat
- Phlebology, Vein Surgery and Ultrasonography: Diagnosis and Management of Venous DiseaseDari EverandPhlebology, Vein Surgery and Ultrasonography: Diagnosis and Management of Venous DiseaseBelum ada peringkat
- Kimax HD03WF Product User Manual Hd03wfDokumen16 halamanKimax HD03WF Product User Manual Hd03wfdewasuryantoBelum ada peringkat
- Water Level Controller Using Arduino. Water Level Indicator Using ArduinoDokumen3 halamanWater Level Controller Using Arduino. Water Level Indicator Using Arduinodewasuryanto0% (1)
- Distance Measurement Using Arduino Ultrasonic Sensor - Code & Circuit DiagramDokumen6 halamanDistance Measurement Using Arduino Ultrasonic Sensor - Code & Circuit DiagramdewasuryantoBelum ada peringkat
- Smart Blind Stick Project Using Arduino and SensorsDokumen11 halamanSmart Blind Stick Project Using Arduino and SensorsdewasuryantoBelum ada peringkat
- Simple Ultrasonic Range Finder Using Arduino. Circuit Diagram, Program and TheoryDokumen4 halamanSimple Ultrasonic Range Finder Using Arduino. Circuit Diagram, Program and Theorydewasuryanto100% (1)
- NiMh and NiCd Battery Charger Circuit Circuit Diagram and InstructionsDokumen1 halamanNiMh and NiCd Battery Charger Circuit Circuit Diagram and InstructionsdewasuryantoBelum ada peringkat
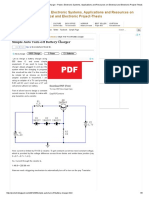
- Simple Auto Turn-Off Battery ChargerDokumen5 halamanSimple Auto Turn-Off Battery ChargerdewasuryantoBelum ada peringkat
- Automatic Water Tank Level Controller With Dry Pump Run Protection Using ArduinoDokumen17 halamanAutomatic Water Tank Level Controller With Dry Pump Run Protection Using Arduinodewasuryanto100% (1)
- High-Range Wireless PowerDokumen14 halamanHigh-Range Wireless PowerdewasuryantoBelum ada peringkat
- How To Build NiCd Battery Charger With Reverse Polarity ProtectionDokumen1 halamanHow To Build NiCd Battery Charger With Reverse Polarity ProtectiondewasuryantoBelum ada peringkat
- Mains Slave TriacDokumen2 halamanMains Slave Triacdewasuryanto100% (3)
- KUBE Electronics AG - Smart SwitchDokumen2 halamanKUBE Electronics AG - Smart SwitchdewasuryantoBelum ada peringkat
- K193 - Smart SLA Battery ChargerDokumen3 halamanK193 - Smart SLA Battery ChargerdewasuryantoBelum ada peringkat
- Battery ChargerDokumen5 halamanBattery ChargerdewasuryantoBelum ada peringkat
- Mains Slave Switcher - DIYDokumen2 halamanMains Slave Switcher - DIYdewasuryantoBelum ada peringkat
- Electronic Circuits, Transformerless Power Supply, LED Drivers, Battery Chargers, Solar Circuits - Automatic Simple 12V 100ma NiCd Battery Charger Circuit PDFDokumen2 halamanElectronic Circuits, Transformerless Power Supply, LED Drivers, Battery Chargers, Solar Circuits - Automatic Simple 12V 100ma NiCd Battery Charger Circuit PDFdewasuryanto100% (1)
- Dimmer Circuit Using SCR - TRIACDokumen10 halamanDimmer Circuit Using SCR - TRIACdewasuryantoBelum ada peringkat
- Current Activated Switch - DIYWikiDokumen5 halamanCurrent Activated Switch - DIYWikidewasuryantoBelum ada peringkat
- Kuliah Ante Natal Care DR Dhanasari UIDokumen21 halamanKuliah Ante Natal Care DR Dhanasari UIdewasuryantoBelum ada peringkat
- Hepatitis B Specimen Submission GuidelinesDokumen5 halamanHepatitis B Specimen Submission GuidelinesdewasuryantoBelum ada peringkat
- 7BBK Lec7 - ABO Discrepancies MQA 2019-09-26 08-14-44Dokumen26 halaman7BBK Lec7 - ABO Discrepancies MQA 2019-09-26 08-14-44gothai sivapragasamBelum ada peringkat
- Sowell ItemsDokumen7 halamanSowell ItemsbrawijayaBelum ada peringkat
- Mechanism of Blood Clotting Extensic Pathway Factors Affecting Blood ClottingDokumen18 halamanMechanism of Blood Clotting Extensic Pathway Factors Affecting Blood ClottingRaunak TripathiBelum ada peringkat
- Unit 7Dokumen228 halamanUnit 7ShekharBelum ada peringkat
- Chapter 16 BLOODDokumen2 halamanChapter 16 BLOODJennyBelum ada peringkat
- Formulir Surat Pengantar Pemeriksaan Kesehatan (SPPK)Dokumen2 halamanFormulir Surat Pengantar Pemeriksaan Kesehatan (SPPK)rachreinaldi49Belum ada peringkat
- ANAPHY Lec Session #14 - SAS (Agdana, Nicole Ken)Dokumen8 halamanANAPHY Lec Session #14 - SAS (Agdana, Nicole Ken)Nicole Ken AgdanaBelum ada peringkat
- Blood GroupDokumen14 halamanBlood GroupAnna Kay BrownBelum ada peringkat
- 1 Hema LecDokumen5 halaman1 Hema LecAngela ReyesBelum ada peringkat
- Transfusion For ChildrenDokumen5 halamanTransfusion For ChildrenKristine Mae AbrasaldoBelum ada peringkat
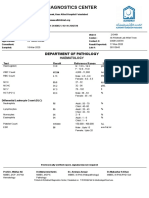
- Al-Khidmat Diagnostics Center: Department of PathologyDokumen1 halamanAl-Khidmat Diagnostics Center: Department of PathologyKiran HassanBelum ada peringkat
- Blood Banking: Answers To FaqsDokumen13 halamanBlood Banking: Answers To FaqsRMBelum ada peringkat
- Issue32 Blood PDFDokumen4 halamanIssue32 Blood PDFGemma CRBelum ada peringkat
- BLOODDokumen46 halamanBLOODLance CarandangBelum ada peringkat
- Hema I Chapter 12 - ESRDokumen30 halamanHema I Chapter 12 - ESRTesfaBelum ada peringkat
- Blood Sample ColectionDokumen17 halamanBlood Sample ColectionSherwan R ShalBelum ada peringkat
- Blood Summary NotesDokumen4 halamanBlood Summary NotesLaura FernandezBelum ada peringkat
- Adverse Transfusion ReactionDokumen38 halamanAdverse Transfusion Reactionmedical laboratoryBelum ada peringkat
- RPG Consent Checklist: Bodily Fluids, Byproducts, and WasteDokumen1 halamanRPG Consent Checklist: Bodily Fluids, Byproducts, and WasteAlfredo ReyesBelum ada peringkat
- Hematology 2Dokumen28 halamanHematology 2saad samyBelum ada peringkat
- Blood Donation:-A Social ResponsibilityDokumen4 halamanBlood Donation:-A Social ResponsibilityPavithraBelum ada peringkat
- Urinalysis, Fecalysis, & Complete Blood Count: NCM 112 Rle Ward ClassDokumen14 halamanUrinalysis, Fecalysis, & Complete Blood Count: NCM 112 Rle Ward ClassJabber PaudacBelum ada peringkat
- Maternal Lab ValuesDokumen1 halamanMaternal Lab ValuesMatthew Ryan100% (1)
- Analisis Hasil Led Pada Jam Pertama Dan Jam KeduaDokumen11 halamanAnalisis Hasil Led Pada Jam Pertama Dan Jam KeduavirafutmainnarBelum ada peringkat
- RH Grouping: James Pretencio Kate Febrian Dabuet Rey Angelo Z. Hidalgo Victor Francis A. SalvanaDokumen8 halamanRH Grouping: James Pretencio Kate Febrian Dabuet Rey Angelo Z. Hidalgo Victor Francis A. SalvanaMarj MendezBelum ada peringkat
- Blood Type Lab ReportDokumen7 halamanBlood Type Lab ReportMisayhui ChanBelum ada peringkat
- Polycythemia Vera and Cerebrovascular EventsDokumen67 halamanPolycythemia Vera and Cerebrovascular EventsChristian Gallardo, MD100% (1)
- Unit-3rd, HAP-1st, 1st Sem, PCI, Carewell PharmaDokumen23 halamanUnit-3rd, HAP-1st, 1st Sem, PCI, Carewell PharmaRithik ModiBelum ada peringkat
- 8.7 Case StudyDokumen2 halaman8.7 Case StudymaddisonBelum ada peringkat
- I - BloodDokumen9 halamanI - BloodKim NgọcBelum ada peringkat