Anda mungkin juga menyukai
- Breast TreatmentDokumen6 halamanBreast TreatmentzainabBelum ada peringkat
- Local Recurrence After Breast-Conserving Surgery and RadiotherapyDokumen6 halamanLocal Recurrence After Breast-Conserving Surgery and RadiotherapyLizeth Rios ZamoraBelum ada peringkat
- Local Recurrence After Breast-Conserving Surgery and RadiotherapyDokumen6 halamanLocal Recurrence After Breast-Conserving Surgery and RadiotherapyLizeth Rios ZamoraBelum ada peringkat
- Journal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardDokumen6 halamanJournal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardJethro ConcepcionBelum ada peringkat
- Management of Breast CADokumen22 halamanManagement of Breast CAAlma FarhanaBelum ada peringkat
- Treatment of Breast Cancer: DR - Syed Alam ZebDokumen51 halamanTreatment of Breast Cancer: DR - Syed Alam ZebSucipto HartonoBelum ada peringkat
- Malignant Melanoma Research PaperDokumen10 halamanMalignant Melanoma Research Paperapi-272931142Belum ada peringkat
- Endoscopic Management of Colorectal T1(SM) CarcinomaDari EverandEndoscopic Management of Colorectal T1(SM) CarcinomaShinji TanakaBelum ada peringkat
- Riker ABSITE ReviewDokumen36 halamanRiker ABSITE Reviewsgod34Belum ada peringkat
- Carcinoma of The Breast - Bailey & LoveDokumen5 halamanCarcinoma of The Breast - Bailey & LoveKeyshia Yazid100% (1)
- Breast Cancer: Presented By: Ola NemriDokumen46 halamanBreast Cancer: Presented By: Ola NemriHaitham Ahmed100% (1)
- EAU Pocket On Muscle Invasive and Metastatic Bladder Cancer 2022Dokumen17 halamanEAU Pocket On Muscle Invasive and Metastatic Bladder Cancer 2022Caio Vinicius SuartzBelum ada peringkat
- Case6. ERISGRUPtesticularcancerDokumen3 halamanCase6. ERISGRUPtesticularcancerJardee DatsimaBelum ada peringkat
- Principles of Management of Soft Tissue SarcomaDokumen33 halamanPrinciples of Management of Soft Tissue Sarcomabashiruaminu100% (1)
- 2011 Sun Myint Anal CAncer Follow-UpDokumen5 halaman2011 Sun Myint Anal CAncer Follow-UpgammasharkBelum ada peringkat
- Breast Cancer Protocol (Version Date 10-JAN-2018)Dokumen11 halamanBreast Cancer Protocol (Version Date 10-JAN-2018)Eugène NkusiBelum ada peringkat
- Case Studies in Advanced Skin Cancer Management: An Osce Viva ResourceDari EverandCase Studies in Advanced Skin Cancer Management: An Osce Viva ResourceBelum ada peringkat
- Carcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaDokumen63 halamanCarcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaBibek GhimireBelum ada peringkat
- EAU Pocket On Muscle Invasive Bladder Cancer 2024Dokumen19 halamanEAU Pocket On Muscle Invasive Bladder Cancer 2024nadaelhaousBelum ada peringkat
- AnalcancerpptDokumen46 halamanAnalcancerpptAnant KumarBelum ada peringkat
- Cancer - Nursing - ReviewerDokumen7 halamanCancer - Nursing - ReviewerDarius CrisostomoBelum ada peringkat
- Vaginal Cuff Removal in Endometrial Carcinoma: Dr. Hira SalmanDokumen38 halamanVaginal Cuff Removal in Endometrial Carcinoma: Dr. Hira SalmandrhirasalmanBelum ada peringkat
- Ovarian CA 450918 SHDokumen52 halamanOvarian CA 450918 SH180045Belum ada peringkat
- Shahan Mumraiz Khan-2017 076Dokumen48 halamanShahan Mumraiz Khan-2017 076zaminazzBelum ada peringkat
- Powerpoint: Breast CancerDokumen89 halamanPowerpoint: Breast Cancerj.doe.hex_8780% (5)
- Malignant Mixed Mullerian Tumor A Case SeriesDokumen7 halamanMalignant Mixed Mullerian Tumor A Case SeriesNico PlantadoBelum ada peringkat
- Journal: Nursing Leadership and ManagementDokumen9 halamanJournal: Nursing Leadership and ManagementdaliaBelum ada peringkat
- Ultrasound Screening of Soft Tissue Masses in The Trunk and Extremity - A BSG Guide For Ultrasonographers and Primary CareDokumen5 halamanUltrasound Screening of Soft Tissue Masses in The Trunk and Extremity - A BSG Guide For Ultrasonographers and Primary CareOmer FarooqBelum ada peringkat
- Oesophageal Carcinoma: Dr. Malghalara Khan PGR, Surgical D Unit, KTHDokumen50 halamanOesophageal Carcinoma: Dr. Malghalara Khan PGR, Surgical D Unit, KTHMalgh Kh100% (2)
- Modified Radical MastectomyDokumen47 halamanModified Radical MastectomyErnie G. Bautista II, RN, MD86% (7)
- Ann Oncol 2012 Chan Vii83 5Dokumen3 halamanAnn Oncol 2012 Chan Vii83 5Fibrianti SeputriBelum ada peringkat
- Breast Cancer WHODokumen104 halamanBreast Cancer WHOGoh Dody100% (2)
- Breast Carcinoma in Axillary Tail of Spence: A Rare Case ReportDokumen4 halamanBreast Carcinoma in Axillary Tail of Spence: A Rare Case Reportrajesh domakuntiBelum ada peringkat
- Breast Malignancy 1Dokumen19 halamanBreast Malignancy 1Muhammad Mubashar HussainBelum ada peringkat
- EBM 2018 - Head and CancersDokumen136 halamanEBM 2018 - Head and CancersChandramohan SettyBelum ada peringkat
- Principles of Surgical Management of Cancer PatientDokumen63 halamanPrinciples of Surgical Management of Cancer PatientbashiruaminuBelum ada peringkat
- Radical Cystectomy: History of The ProcedureDokumen6 halamanRadical Cystectomy: History of The ProcedureIvy MinaBelum ada peringkat
- Practice Essentials: Signs and SymptomsDokumen20 halamanPractice Essentials: Signs and SymptomsrainbowshopBelum ada peringkat
- Five Emrcs NotesDokumen18 halamanFive Emrcs NotesDeen MohammadBelum ada peringkat
- The Big Four - Breast CA OLDDokumen36 halamanThe Big Four - Breast CA OLDfr4nc1s4ggr3yBelum ada peringkat
- The Future of External Beam Irradiation As Initial Treatment of Rectal CancerDokumen6 halamanThe Future of External Beam Irradiation As Initial Treatment of Rectal CancerMaxime PorcoBelum ada peringkat
- Case Study Breast CaDokumen32 halamanCase Study Breast Caapi-391376321Belum ada peringkat
- Breast GSUDokumen48 halamanBreast GSUAbdalla SamatarBelum ada peringkat
- London Cancer Head and Neck Radiotherapy Protocol March 2013Dokumen10 halamanLondon Cancer Head and Neck Radiotherapy Protocol March 2013handrionoBelum ada peringkat
- AJCC Cancer Staging Manual Stomach 7theditionDokumen3 halamanAJCC Cancer Staging Manual Stomach 7theditionCamelia CalugariciBelum ada peringkat
- Handbook Rhabdomyosarcoma Winter2018Dokumen14 halamanHandbook Rhabdomyosarcoma Winter2018Rizky AmaliahBelum ada peringkat
- 2010 Article 22Dokumen16 halaman2010 Article 22Andreas KrishnaputraBelum ada peringkat
- Uterine CancerDokumen10 halamanUterine CancerKristen Leigh MarianoBelum ada peringkat
- (Mama) Brady1977Dokumen7 halaman(Mama) Brady1977Gabriela Silva MartinsBelum ada peringkat
- Evaluation of Axillary Lymphadenopathy With Carcinoma BreastDokumen42 halamanEvaluation of Axillary Lymphadenopathy With Carcinoma BreastMashrufBelum ada peringkat
- Overview of Management of The Regional Lymph Nodes in Breast CancerDokumen32 halamanOverview of Management of The Regional Lymph Nodes in Breast CancerisahBelum ada peringkat
- Comparing Breast-Conserving Surgery With Radical MastectomyDokumen6 halamanComparing Breast-Conserving Surgery With Radical MastectomyRonald Cariaco FlamesBelum ada peringkat
- Guidelines On Testicular Cancer: (Limited Text Update March 2009)Dokumen18 halamanGuidelines On Testicular Cancer: (Limited Text Update March 2009)PJ CoBelum ada peringkat
- Neoadjuvant Chemoradiotherapy, Radiotherapy, and Chemotherapy For Rectal Adenocarcinoma - UpToDateDokumen27 halamanNeoadjuvant Chemoradiotherapy, Radiotherapy, and Chemotherapy For Rectal Adenocarcinoma - UpToDateRaíla SoaresBelum ada peringkat
- Palliative Surgery in Breast CancerDokumen38 halamanPalliative Surgery in Breast CancerIndonesian Journal of Cancer100% (1)
- Breast CaDokumen35 halamanBreast CaVincent SerBelum ada peringkat
- Breast Cancer Study Case PDFDokumen8 halamanBreast Cancer Study Case PDFLuna LinBelum ada peringkat
- BladderDokumen36 halamanBladderdrsumitavaBelum ada peringkat
- Journal Reading: "Endothelial Function and Inflammation in Coronary Artery Disease"Dokumen18 halamanJournal Reading: "Endothelial Function and Inflammation in Coronary Artery Disease"kadinfathiaBelum ada peringkat
- Materi RTD Bagian: Co-Ass AnestesiDokumen3 halamanMateri RTD Bagian: Co-Ass AnestesikadinfathiaBelum ada peringkat
- Bladder Carsinomas: Azif Zilal FauqiDokumen18 halamanBladder Carsinomas: Azif Zilal FauqikadinfathiaBelum ada peringkat
- Exogenous Ochronosis With Use of Low Potency Hydroquinone in A Caucasian PatientDokumen27 halamanExogenous Ochronosis With Use of Low Potency Hydroquinone in A Caucasian PatientkadinfathiaBelum ada peringkat
- Lower Respiratory SystemDokumen27 halamanLower Respiratory SystemkadinfathiaBelum ada peringkat
- OphthalmologyDokumen22 halamanOphthalmologykadinfathia0% (1)
- Translate Jurnal KeratitisDokumen7 halamanTranslate Jurnal KeratitiskadinfathiaBelum ada peringkat
- Tests of NormalityDokumen18 halamanTests of NormalitykadinfathiaBelum ada peringkat
- Sectional - This Study Used A Sample of 30 Midwives Based On Inclusion and Exclusion CriteriaDokumen1 halamanSectional - This Study Used A Sample of 30 Midwives Based On Inclusion and Exclusion CriteriakadinfathiaBelum ada peringkat
- Jurnal KulitDokumen24 halamanJurnal KulitkadinfathiaBelum ada peringkat
- Ipss PDFDokumen2 halamanIpss PDFFrida AnggaBelum ada peringkat
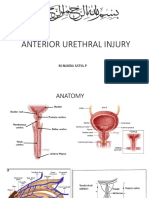
- Rupture Urethra Anterior DR Sule FixDokumen36 halamanRupture Urethra Anterior DR Sule FixkadinfathiaBelum ada peringkat
- Sensus Pasien Anak Rsud K.R.M.T Wongsonegoro: Belum Visite Sudah Visite Belum Visite Sudah VisiteDokumen2 halamanSensus Pasien Anak Rsud K.R.M.T Wongsonegoro: Belum Visite Sudah Visite Belum Visite Sudah VisitekadinfathiaBelum ada peringkat
- List Perpus RadiologiDokumen2 halamanList Perpus RadiologikadinfathiaBelum ada peringkat
- LBM 3 LI FathiaDokumen29 halamanLBM 3 LI FathiakadinfathiaBelum ada peringkat
- LBM 3 LI FathiaDokumen29 halamanLBM 3 LI FathiakadinfathiaBelum ada peringkat
- Definisi Epidemiologi Klasifikasi Etiologi & Faktor Risiko Manifestasi Klinis Diagnosis Sistem Staging TerapiDokumen37 halamanDefinisi Epidemiologi Klasifikasi Etiologi & Faktor Risiko Manifestasi Klinis Diagnosis Sistem Staging TerapikadinfathiaBelum ada peringkat
- Definisi Epidemiologi Klasifikasi Etiologi & Faktor Risiko Manifestasi Klinis Diagnosis Sistem Staging TerapiDokumen37 halamanDefinisi Epidemiologi Klasifikasi Etiologi & Faktor Risiko Manifestasi Klinis Diagnosis Sistem Staging TerapikadinfathiaBelum ada peringkat
- Modalitas Belajar Menjadi Pembelajar Multi Indrawi: Umatul KhoiriyahDokumen29 halamanModalitas Belajar Menjadi Pembelajar Multi Indrawi: Umatul KhoiriyahkadinfathiaBelum ada peringkat
- Speech About SDGs HealthDokumen2 halamanSpeech About SDGs HealthkadinfathiaBelum ada peringkat
- Seven Jump Dalam Diskusi TutorialDokumen39 halamanSeven Jump Dalam Diskusi TutorialkadinfathiaBelum ada peringkat
- Fathia K DinantiDokumen21 halamanFathia K DinantikadinfathiaBelum ada peringkat
- Female Genital Tract Cytopathology: PracticalDokumen26 halamanFemale Genital Tract Cytopathology: PracticalNgotelo FunwiBelum ada peringkat
- All India Ayush Post Graduate Entrance Test 2019 Question PaperDokumen24 halamanAll India Ayush Post Graduate Entrance Test 2019 Question PaperSoumitra BoseBelum ada peringkat
- Artikel Bahan Ujian PraktikumDokumen10 halamanArtikel Bahan Ujian PraktikumTakiaGenjiBelum ada peringkat
- Case Report: Perioperative Management of A Patient With Secreting Paraganglioma Undergoing Cesarean SectionDokumen3 halamanCase Report: Perioperative Management of A Patient With Secreting Paraganglioma Undergoing Cesarean SectionYolanda FitrianiBelum ada peringkat
- Discover Health PompleteDokumen2 halamanDiscover Health PompletenawabBelum ada peringkat
- Oceanic Question Bank Year 4Dokumen358 halamanOceanic Question Bank Year 4maryBelum ada peringkat
- Crohn Vs ColitisDokumen5 halamanCrohn Vs Colitiswbarnes7Belum ada peringkat
- 14 - UveitisDokumen4 halaman14 - UveitisSpislgal PhilipBelum ada peringkat
- 3 ACC Prevention Blood PressureDokumen69 halaman3 ACC Prevention Blood PressureMelissa Delgado100% (1)
- A A To Raco AbdominalDokumen64 halamanA A To Raco AbdominalYgor AlbuquerqueBelum ada peringkat
- Time in Time Out: Temperature Monitoring Log Sheet For The Month of February 2019Dokumen6 halamanTime in Time Out: Temperature Monitoring Log Sheet For The Month of February 2019Waqas VickyBelum ada peringkat
- DONOR SELECTION (Deferral) - BBDokumen5 halamanDONOR SELECTION (Deferral) - BBMaikka IlaganBelum ada peringkat
- Should Covid Vaccination Really Needs To Be Mandatory?Dokumen2 halamanShould Covid Vaccination Really Needs To Be Mandatory?ElenizelBelum ada peringkat
- Mycobacterium Tuberculosis: Paper Esm MicrobiologyDokumen15 halamanMycobacterium Tuberculosis: Paper Esm MicrobiologyMuhammad KurniawanBelum ada peringkat
- Astigmidwife Vlogs Online Tutorial: All Rights Are Reserved. No Part of This Publication May Be ReproducedDokumen12 halamanAstigmidwife Vlogs Online Tutorial: All Rights Are Reserved. No Part of This Publication May Be ReproducedLynden BulanBelum ada peringkat
- TESDA COVID-19 Test (Answer Keys)Dokumen12 halamanTESDA COVID-19 Test (Answer Keys)ash mizushiBelum ada peringkat
- Ateneo de Zamboanga University: College of Nursing Nursing Skills Output (Nso) Week Biopsy I. DescritptionDokumen4 halamanAteneo de Zamboanga University: College of Nursing Nursing Skills Output (Nso) Week Biopsy I. DescritptionHaifi HunBelum ada peringkat
- Acupuncture 123Dokumen3 halamanAcupuncture 123Romi Brener83% (6)
- Geriatric OtolaryngologyDokumen26 halamanGeriatric OtolaryngologySari RakhmawatiBelum ada peringkat
- Assessment of The Effect of Epidural Steroid Injection in Patient Having Lumbar RadiculopathyDokumen5 halamanAssessment of The Effect of Epidural Steroid Injection in Patient Having Lumbar RadiculopathyIJAR JOURNALBelum ada peringkat
- Obstructive JaundiceDokumen13 halamanObstructive JaundiceJeevan VijayBelum ada peringkat
- General Properties of CestodesDokumen42 halamanGeneral Properties of CestodesNicole NipasBelum ada peringkat
- Holoxan Pi PDFDokumen18 halamanHoloxan Pi PDFKarol IonasBelum ada peringkat
- Treatment of Hemophilia A and B PDFDokumen268 halamanTreatment of Hemophilia A and B PDFYusry SuryawiraBelum ada peringkat
- I-Choose The Correct Answer of The Following Sentences:: Palestine College of NursingDokumen9 halamanI-Choose The Correct Answer of The Following Sentences:: Palestine College of NursingHasan A AsFourBelum ada peringkat
- Autonomic Self AssessmentDokumen8 halamanAutonomic Self AssessmentElisa ValdésBelum ada peringkat
- 53 Coronary Artery AnomaliesDokumen5 halaman53 Coronary Artery AnomaliesVictor PazBelum ada peringkat
- Medial Medullary Syndrome - WikipediaDokumen8 halamanMedial Medullary Syndrome - WikipediaArun KumarBelum ada peringkat
- EmergencyDokumen7 halamanEmergencymedodiabBelum ada peringkat
- AUH Travel Declaration FormDokumen2 halamanAUH Travel Declaration FormAbdul RahmanBelum ada peringkat