Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
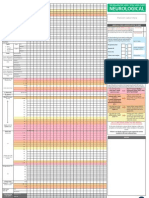
- Adult Early Warning Score Observation Chart For Neurosurgical UnitDokumen1 halamanAdult Early Warning Score Observation Chart For Neurosurgical UnitalexipsBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Clinical Volume 11 ISBAR Handover/Communication PolicyDokumen4 halamanClinical Volume 11 ISBAR Handover/Communication PolicyArive Haruzz BizzaBelum ada peringkat
- Family vital signs chartDokumen2 halamanFamily vital signs chartbasheBelum ada peringkat
- Hospital Rapid Response TeamDokumen9 halamanHospital Rapid Response TeamjamieBelum ada peringkat
- Adult Early Warning Score Observation Chart For Wellington HospitalDokumen1 halamanAdult Early Warning Score Observation Chart For Wellington HospitalalexipsBelum ada peringkat
- National Early Warning Score (NEWS)Dokumen47 halamanNational Early Warning Score (NEWS)Anonymous odb9XJWL0Belum ada peringkat
- RSU SWASTA MONTELLA: Kesembuhan pasien kebanggaan kamiDokumen3 halamanRSU SWASTA MONTELLA: Kesembuhan pasien kebanggaan kamijuliansyahjuventusBelum ada peringkat
- Hubungan Antara Pola Makan Dengan Kadar Asam Urat Darah Pada Wanita Postmenopause Di Posyandu Lansia Wilayah Kerja Puskesmas DR Soetomo SurabayaDokumen7 halamanHubungan Antara Pola Makan Dengan Kadar Asam Urat Darah Pada Wanita Postmenopause Di Posyandu Lansia Wilayah Kerja Puskesmas DR Soetomo SurabayaAlfinda Diah AjengBelum ada peringkat
- Leaflet SadariDokumen2 halamanLeaflet SadarijuliansyahjuventusBelum ada peringkat
- Puskesmas Marabahan - Community Health CenterDokumen2 halamanPuskesmas Marabahan - Community Health CenterjuliansyahjuventusBelum ada peringkat
- Tabel Kadar As UratDokumen1 halamanTabel Kadar As UratjuliansyahjuventusBelum ada peringkat
- Piis0161642014003893 PDFDokumen10 halamanPiis0161642014003893 PDFZhakiAlAsrorBelum ada peringkat
- 1824 7288 39 18Dokumen8 halaman1824 7288 39 18Justy GuavaBelum ada peringkat
- How Is Infection Treated in People With CancerDokumen3 halamanHow Is Infection Treated in People With CancerjuliansyahjuventusBelum ada peringkat
- Field Study Semester 1Dokumen7 halamanField Study Semester 1juliansyahjuventusBelum ada peringkat
- Dengue Update - WHO2009 Guideline REVISEDDokumen29 halamanDengue Update - WHO2009 Guideline REVISEDMedico Nol DelaphanBelum ada peringkat
- EWS for NewbornsDokumen6 halamanEWS for NewbornsElizeus HaninditoBelum ada peringkat
- CCrISP 1 IntroductionDokumen19 halamanCCrISP 1 Introductionpioneer92Belum ada peringkat
- Modified Early Warning Score (MEWS) Observation Chart: Clinical ProtocolDokumen4 halamanModified Early Warning Score (MEWS) Observation Chart: Clinical ProtocolElena DolcanBelum ada peringkat
- Impact of Health Informatics TechnologyDokumen11 halamanImpact of Health Informatics TechnologyhiijjournalBelum ada peringkat
- Mews ScoreDokumen13 halamanMews Score2009nicoleta100% (2)
- Early Warning Score RosalinaDokumen18 halamanEarly Warning Score RosalinaRosalina LubisBelum ada peringkat
- Adult Early Warning Score Observation Chart For Cardiothoracic UnitDokumen1 halamanAdult Early Warning Score Observation Chart For Cardiothoracic UnitalexipsBelum ada peringkat
- RONAK Research ProposalDokumen29 halamanRONAK Research ProposalRonak PatidarBelum ada peringkat
- National Early Warning Score (NEWS)Dokumen4 halamanNational Early Warning Score (NEWS)mutiara rizkiBelum ada peringkat
- Workshop On Early Warning Score System - Ali HaedarDokumen61 halamanWorkshop On Early Warning Score System - Ali HaedarGede Kevin Adhitya SaputraBelum ada peringkat
- Stretch 2020Dokumen7 halamanStretch 2020Caio OliveiraBelum ada peringkat
- Modified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2Dokumen9 halamanModified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2indirinoor5Belum ada peringkat
- Aplication Progress of Modified Early Warning Score in General DepartmentsDokumen10 halamanAplication Progress of Modified Early Warning Score in General DepartmentsFemyLealBelum ada peringkat
- Daftar PustakaDokumen4 halamanDaftar PustakaKharisma AnjarBelum ada peringkat
- Adult vital signs monitoring chartDokumen2 halamanAdult vital signs monitoring chartHilal Mohamed NorBelum ada peringkat
- 4612 Early Warning Score (June 2013)Dokumen8 halaman4612 Early Warning Score (June 2013)Safiqulatif AbdillahBelum ada peringkat
- An Integrative Review of Pediatric Early Warning System ScoresDokumen10 halamanAn Integrative Review of Pediatric Early Warning System ScoresKarma SetiyawanBelum ada peringkat
- New Zealand Early Warning Score Vital Sign Chart User Guide 2017Dokumen19 halamanNew Zealand Early Warning Score Vital Sign Chart User Guide 2017Darma YantieBelum ada peringkat
- Hubungan Tingkat Pengetahuan Dengan Kepatuhan Perawat Dalam Menjalankan Early Warning Score Di Rumah Sakit Bimc KutaDokumen8 halamanHubungan Tingkat Pengetahuan Dengan Kepatuhan Perawat Dalam Menjalankan Early Warning Score Di Rumah Sakit Bimc KutatarsonBelum ada peringkat
- Daftar Pustaka: M. DERI RAMADHAN, Dr. Sri Setiyarini, S.KP., M.Kes Uki Noviana, S.Kep., NS., MN - SC., PH.DDokumen4 halamanDaftar Pustaka: M. DERI RAMADHAN, Dr. Sri Setiyarini, S.KP., M.Kes Uki Noviana, S.Kep., NS., MN - SC., PH.DDesinta BungaBelum ada peringkat
- L. Artikel EWSSDokumen9 halamanL. Artikel EWSSmuchtarBelum ada peringkat
- 137c PDFDokumen221 halaman137c PDFSimonBelum ada peringkat
- Adult Early Warning Score Observation Chart For Cardiology UnitDokumen1 halamanAdult Early Warning Score Observation Chart For Cardiology UnitalexipsBelum ada peringkat
- 09 Ra Early Warning ScoringDokumen3 halaman09 Ra Early Warning ScoringREZBelum ada peringkat