Anda mungkin juga menyukai
- Nle Tips MS PDFDokumen11 halamanNle Tips MS PDFjthsBelum ada peringkat
- July 2012 Pnle Pearls of Success Part 5: Psychiatric NursingDokumen6 halamanJuly 2012 Pnle Pearls of Success Part 5: Psychiatric NursingLiezel CauilanBelum ada peringkat
- Tips Sa Board ExamsDokumen3 halamanTips Sa Board ExamsHarrison TallodBelum ada peringkat
- Nursing Research: Pentagon Professional Adjustment, Legal Management, Ethics & Research in NursingDokumen27 halamanNursing Research: Pentagon Professional Adjustment, Legal Management, Ethics & Research in NursingMellisa Faith Yebes GoBelum ada peringkat
- July 2012 Nle Tips-Chn and CDDokumen7 halamanJuly 2012 Nle Tips-Chn and CDJerome Asuncion67% (3)
- July PNLE 2011 PreBoard ExamDokumen9 halamanJuly PNLE 2011 PreBoard ExamRon KimBelum ada peringkat
- NP1 Dec 2006 NLEDokumen16 halamanNP1 Dec 2006 NLElibrebuk23100% (1)
- Nursing Practice V EdgeworthDokumen8 halamanNursing Practice V EdgeworthRichard Ines Valino100% (8)
- Nursing Practice II EdgeworthDokumen9 halamanNursing Practice II EdgeworthRichard Ines Valino100% (1)
- November 2008 PNLEDokumen78 halamanNovember 2008 PNLEDon MarcusBelum ada peringkat
- Nursing Practice 1 (Dec 2006)Dokumen12 halamanNursing Practice 1 (Dec 2006)ɹǝʍdןnos100% (1)
- Medical Surgical Nursing Bullets Nle NclexDokumen95 halamanMedical Surgical Nursing Bullets Nle NclexRichard Ines Valino100% (2)
- CHN&CDDokumen7 halamanCHN&CDDharline Abbygale Garvida AgullanaBelum ada peringkat
- Sample Questions PNLEDokumen12 halamanSample Questions PNLEErika NicaBelum ada peringkat
- PNLEDokumen3 halamanPNLEJonas Marvin AnaqueBelum ada peringkat
- Tips On How To Pass The NLE 2019Dokumen1 halamanTips On How To Pass The NLE 2019Anonymous xFCmP2K0D5Belum ada peringkat
- Board Exam Compilation Book 2 SampleDokumen11 halamanBoard Exam Compilation Book 2 SampleElizabella Henrietta TanaquilBelum ada peringkat
- Nle ReviewDokumen7 halamanNle ReviewRio BonifacioBelum ada peringkat
- NP1 Nursing Board Exam December 2006 Answer Key OKDokumen13 halamanNP1 Nursing Board Exam December 2006 Answer Key OKSam ParkBelum ada peringkat
- PNLE PreDokumen147 halamanPNLE PreRS Buenavista100% (8)
- 2019TOPNOTCHERDokumen27 halaman2019TOPNOTCHERjimboyBelum ada peringkat
- Nursing Practice IV EdgeworthDokumen9 halamanNursing Practice IV EdgeworthRichard Ines Valino100% (6)
- Pentagon Maternal and Child PDFDokumen38 halamanPentagon Maternal and Child PDFmarie89meBelum ada peringkat
- MS Review EdgeworthDokumen89 halamanMS Review EdgeworthRichard Ines Valino100% (7)
- Philippine Nursing Licensure ExaminationDokumen32 halamanPhilippine Nursing Licensure ExaminationVera100% (1)
- MS Compre 2015A Ans KeyDokumen8 halamanMS Compre 2015A Ans KeyPaul Lexus Gomez LorenzoBelum ada peringkat
- PNLEDokumen5 halamanPNLEBrian100% (2)
- Nle Nle Nle!!!!!!!Dokumen108 halamanNle Nle Nle!!!!!!!SohailashiBelum ada peringkat
- Pnle ExamsDokumen80 halamanPnle Examsgilissa100% (3)
- Toprank Review Pediatric Nursing NotesDokumen12 halamanToprank Review Pediatric Nursing NotesCose online shopBelum ada peringkat
- PNLEDokumen35 halamanPNLECharm TanyaBelum ada peringkat
- Intensive CHN TominesDokumen11 halamanIntensive CHN Tominesmark OrpillaBelum ada peringkat
- PNLE IV Nursing PracticeDokumen8 halamanPNLE IV Nursing PracticeDanielle KayeBelum ada peringkat
- PNLE: Maternal and Child Health Nursing Exam 2Dokumen6 halamanPNLE: Maternal and Child Health Nursing Exam 2Darnell Adrian EstobioBelum ada peringkat
- NP1Dokumen25 halamanNP1Andrea Franchesca DelaCruz Descalzo100% (2)
- NLE Pediatric Nursing Pentagon ReviewerDokumen65 halamanNLE Pediatric Nursing Pentagon Reviewerarcci balinas0% (1)
- Community Health NursingDokumen16 halamanCommunity Health NursingFilipino Nurses Central67% (3)
- PNLE June 2007 With Key AnswersDokumen82 halamanPNLE June 2007 With Key AnswersJustin CubillasBelum ada peringkat
- OB Nursing Bullets PNLEDokumen25 halamanOB Nursing Bullets PNLEACBelum ada peringkat
- Republic of The Philippines Professional Regulation Commission ManilaDokumen3 halamanRepublic of The Philippines Professional Regulation Commission ManilaTheSummitExpress0% (1)
- NLE PrioritizationDokumen73 halamanNLE PrioritizationabcalagoBelum ada peringkat
- PNLE II Nursing PracticeDokumen16 halamanPNLE II Nursing PracticeIk-ik MiralBelum ada peringkat
- NP2 RationaleDokumen32 halamanNP2 RationaleCeejhaye TamangBelum ada peringkat
- Practice Test 4Dokumen15 halamanPractice Test 4Kira100% (9)
- Reviewer NLEDokumen197 halamanReviewer NLECon GallanoBelum ada peringkat
- Nle 2015 QuestionsDokumen4 halamanNle 2015 QuestionsJona Suarez100% (1)
- Top Up Training Center and Research Consultancy Communicable Disease NursingDokumen3 halamanTop Up Training Center and Research Consultancy Communicable Disease NursingSTEFFI GABRIELLE GOLEZBelum ada peringkat
- Board Exam Compilation Book 2 SampleDokumen10 halamanBoard Exam Compilation Book 2 SampleebookwholesellerBelum ada peringkat
- 2008 NP4Dokumen11 halaman2008 NP4Jeremiash Noblesala Dela CruzBelum ada peringkat
- Fundamentals of NursingDokumen3 halamanFundamentals of NursingFrancis James RigodonBelum ada peringkat
- Nursing ProcessDokumen4 halamanNursing ProcessTine GuibaoBelum ada peringkat
- PART 1 Health Assessment Lec Prelim TransesDokumen11 halamanPART 1 Health Assessment Lec Prelim TransesLoLiBelum ada peringkat
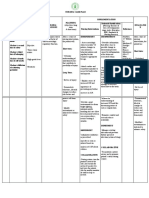
- 4 Nursing-Care-Plan SchizoDokumen6 halaman4 Nursing-Care-Plan SchizoJai GoBelum ada peringkat
- My NoteDokumen6 halamanMy NotePrincess Mae SabadoBelum ada peringkat
- Health Assessment Reviewer (Prelims)Dokumen9 halamanHealth Assessment Reviewer (Prelims)Frances Nicole Flores100% (1)
- NCP Pot Riskforinjury EncephalitisDokumen3 halamanNCP Pot Riskforinjury Encephalitisaila angBelum ada peringkat
- Four Ways of Knowing Nursing NotesDokumen2 halamanFour Ways of Knowing Nursing NotesJoker ParkBelum ada peringkat
- Health Assessment Lecture ReviewerDokumen18 halamanHealth Assessment Lecture ReviewerMinminkajaBelum ada peringkat
- FUNDAMENTALS OF NURSING NotesDokumen3 halamanFUNDAMENTALS OF NURSING Noteskwgchyrn1Belum ada peringkat
- Procedure Checklist Chapter 27: Inserting An Indwelling Urinary Catheter (Male)Dokumen4 halamanProcedure Checklist Chapter 27: Inserting An Indwelling Urinary Catheter (Male)jths100% (1)
- Moving Together As 1Dokumen10 halamanMoving Together As 1jthsBelum ada peringkat
- Mental Health Vs WorkDokumen77 halamanMental Health Vs WorkOktasari Dyah AnggrainiBelum ada peringkat
- Procedure Checklist Chapter 27: Collecting A Clean-Catch Urine SpecimenDokumen2 halamanProcedure Checklist Chapter 27: Collecting A Clean-Catch Urine SpecimenjthsBelum ada peringkat
- Procedure Checklist Chapter 27: Continuous Bladder IrrigationDokumen2 halamanProcedure Checklist Chapter 27: Continuous Bladder IrrigationjthsBelum ada peringkat
- Procedure Checklist Chapter 27: Inserting A Straight Urinary Catheter (Male)Dokumen4 halamanProcedure Checklist Chapter 27: Inserting A Straight Urinary Catheter (Male)jthsBelum ada peringkat
- Procedure Checklist Chapter 23: Using A Tandem (Secondary) SetDokumen2 halamanProcedure Checklist Chapter 23: Using A Tandem (Secondary) SetjthsBelum ada peringkat
- Procedure Checklist Chapter 23: Recapping Needles Using One-Handed TechniqueDokumen2 halamanProcedure Checklist Chapter 23: Recapping Needles Using One-Handed TechniquejthsBelum ada peringkat
- Procedure Checklist Chapter 23: Mixing Medications in One Syringe, Using A Prefilled Cartridge and Single-Dose Vial - For Intravenous AdministrationDokumen2 halamanProcedure Checklist Chapter 23: Mixing Medications in One Syringe, Using A Prefilled Cartridge and Single-Dose Vial - For Intravenous AdministrationjthsBelum ada peringkat
- PC ch27-04Dokumen4 halamanPC ch27-04jthsBelum ada peringkat
- Procedure Checklist Chapter 26: Removing A Nasogastric or Nasoenteric TubeDokumen1 halamanProcedure Checklist Chapter 26: Removing A Nasogastric or Nasoenteric TubejthsBelum ada peringkat
- Checklist PDFDokumen4 halamanChecklist PDFnamithaBelum ada peringkat
- Procedure Checklist Chapter 27: Applying An External (Condom) CatheterDokumen2 halamanProcedure Checklist Chapter 27: Applying An External (Condom) CatheterjthsBelum ada peringkat
- PC ch23-21Dokumen2 halamanPC ch23-21jthsBelum ada peringkat
- Procedure Checklist Chapter 26: Administering Feedings Through Gastric and Enteric TubesDokumen3 halamanProcedure Checklist Chapter 26: Administering Feedings Through Gastric and Enteric TubesjthsBelum ada peringkat
- Procedure Checklist Chapter 23: Using A Volume-Control Administration Set (E.g., Buretrol, Volutrol, Soluset)Dokumen2 halamanProcedure Checklist Chapter 23: Using A Volume-Control Administration Set (E.g., Buretrol, Volutrol, Soluset)jthsBelum ada peringkat
- Procedure Checklist Chapter 26: Inserting Nasogastric and Nasoenteric TubesDokumen3 halamanProcedure Checklist Chapter 26: Inserting Nasogastric and Nasoenteric TubesjthsBelum ada peringkat
- PC ch23-24Dokumen2 halamanPC ch23-24jthsBelum ada peringkat
- Procedure Checklist Chapter 26 - Checking Fingerstick (Capillary) Blood Glucose LevelsDokumen2 halamanProcedure Checklist Chapter 26 - Checking Fingerstick (Capillary) Blood Glucose LevelsjthsBelum ada peringkat
- Procedure Checklist Chapter 23: Administering Intramuscular InjectionsDokumen3 halamanProcedure Checklist Chapter 23: Administering Intramuscular InjectionsjthsBelum ada peringkat
- Procedure Checklist Chapter 23: Mixing Medications in One Syringe, Using One Ampule and VialDokumen2 halamanProcedure Checklist Chapter 23: Mixing Medications in One Syringe, Using One Ampule and VialjthsBelum ada peringkat
- Procedure Checklist Chapter 23: Preparing and Drawing Up Medications From VialsDokumen2 halamanProcedure Checklist Chapter 23: Preparing and Drawing Up Medications From VialsjthsBelum ada peringkat
- PC ch23-20Dokumen2 halamanPC ch23-20jthsBelum ada peringkat
- PC ch23-10Dokumen1 halamanPC ch23-10jthsBelum ada peringkat
- Procedure Checklist Chapter 23: Inserting A Rectal SuppositoryDokumen1 halamanProcedure Checklist Chapter 23: Inserting A Rectal SuppositoryjthsBelum ada peringkat
- PC Ch23-14 VagivalDokumen2 halamanPC Ch23-14 Vagivalmacs_smacBelum ada peringkat
- PC ch23-06Dokumen2 halamanPC ch23-06jthsBelum ada peringkat
- Procedure Checklist Chapter 23: Administering Medications Through An Enteral TubeDokumen2 halamanProcedure Checklist Chapter 23: Administering Medications Through An Enteral Tubejths100% (1)
- Procedure Checklist Chapter 23: Administering Oral MedicationsDokumen2 halamanProcedure Checklist Chapter 23: Administering Oral Medicationsmacs_smacBelum ada peringkat
- Procedure Checklist Chapter 23: Administering IV Push Medications Through A Running Primary IV LineDokumen2 halamanProcedure Checklist Chapter 23: Administering IV Push Medications Through A Running Primary IV LineLiezel CauilanBelum ada peringkat
- Introductory Econometrics A Modern Approach Solutions Manual PDFDokumen9 halamanIntroductory Econometrics A Modern Approach Solutions Manual PDFAnonymous bzcYj42Ain0% (2)
- Global University Rankings and Their ImpactDokumen85 halamanGlobal University Rankings and Their ImpactКино ФильмBelum ada peringkat
- Appeal For Exclusion COA For An Act Committed in Good FaithDokumen13 halamanAppeal For Exclusion COA For An Act Committed in Good FaithPj Tigniman100% (6)
- Kerala University PHD Course Work Exam SyllabusDokumen4 halamanKerala University PHD Course Work Exam Syllabuslozuzimobow3100% (2)
- IM4PBDokumen518 halamanIM4PBJagdish HathiBelum ada peringkat
- Ethical Hacking and Penetration Testing Guide - Baloch, RafayDokumen2 halamanEthical Hacking and Penetration Testing Guide - Baloch, RafayAyush PoptaniBelum ada peringkat
- Robin Desharnais ResumeDokumen2 halamanRobin Desharnais Resumeapi-281112719Belum ada peringkat
- Lecture05e Anharmonic Effects 2Dokumen15 halamanLecture05e Anharmonic Effects 2Saeed AzarBelum ada peringkat
- The Council of Nicaea and The History of The Invention of ChristianityDokumen10 halamanThe Council of Nicaea and The History of The Invention of Christianitybearhunter001Belum ada peringkat
- NLS Arabic and French Issue R12.1.3Dokumen7 halamanNLS Arabic and French Issue R12.1.3Anil RawatBelum ada peringkat
- Junto, Brian Cesar S.Dokumen1 halamanJunto, Brian Cesar S.Brian Cesar JuntoBelum ada peringkat
- Ansari Ibnarabdoctrine 1999Dokumen45 halamanAnsari Ibnarabdoctrine 1999JYOTI PALBelum ada peringkat
- Oracle Database Performance Tuning Advanced Features and Best Practices For DbasDokumen303 halamanOracle Database Performance Tuning Advanced Features and Best Practices For Dbassss pppBelum ada peringkat
- 112-1 中英筆譯Dokumen15 halaman112-1 中英筆譯beenbenny825Belum ada peringkat
- Test 2A AP StatisticsDokumen5 halamanTest 2A AP StatisticssnarkjazzoBelum ada peringkat
- CHAPTER 1 Final OkDokumen43 halamanCHAPTER 1 Final Okroneldayo62Belum ada peringkat
- The Law of Attraction Work For YouDokumen7 halamanThe Law of Attraction Work For YouBambang PrasetyoBelum ada peringkat
- Breast Stimulation Susilowati 2004138Dokumen11 halamanBreast Stimulation Susilowati 2004138Ahmad SaifuddinBelum ada peringkat
- 08 Subsurface Sucker-Rod Pumps PDFDokumen10 halaman08 Subsurface Sucker-Rod Pumps PDFBanda ClaretBelum ada peringkat
- Ecdis-24 01Dokumen4 halamanEcdis-24 01Leandro PintoBelum ada peringkat
- Choral Speaking - Our School LifeDokumen4 halamanChoral Speaking - Our School LifeAINA AZMINA BINTI ANUAR KPM-GuruBelum ada peringkat
- 4TH Semester B.A., LL.B B.A., LL.B (H)Dokumen14 halaman4TH Semester B.A., LL.B B.A., LL.B (H)BISTIRNA BARUABelum ada peringkat
- G.R. No. 92735 Monarch V CA - DigestDokumen2 halamanG.R. No. 92735 Monarch V CA - DigestOjie Santillan100% (1)
- Daily Lesson LogDokumen6 halamanDaily Lesson LogNicoleMortelBelum ada peringkat
- Cover Letter-Alexis ReedDokumen1 halamanCover Letter-Alexis Reedapi-252291947Belum ada peringkat
- PHD 2020 21 List of Shortlisted Candidates For InterviewDokumen6 halamanPHD 2020 21 List of Shortlisted Candidates For InterviewAnkesh Kumar SrivastavaBelum ada peringkat
- A Written Report in Pure Monopoly: Submitted ToDokumen12 halamanA Written Report in Pure Monopoly: Submitted ToEd Leen ÜBelum ada peringkat
- 2008-12-16Dokumen32 halaman2008-12-16CoolerAdsBelum ada peringkat
- All IL Corporate Filings by The Save-A-Life Foundation (SALF) Including 9/17/09 Dissolution (1993-2009)Dokumen48 halamanAll IL Corporate Filings by The Save-A-Life Foundation (SALF) Including 9/17/09 Dissolution (1993-2009)Peter M. HeimlichBelum ada peringkat
- Module 5 Network Design in The Supply ChainDokumen15 halamanModule 5 Network Design in The Supply ChainstraheelBelum ada peringkat