Anda mungkin juga menyukai
- A Guide in Practical Psychrometrics for Students and EngineersDari EverandA Guide in Practical Psychrometrics for Students and EngineersBelum ada peringkat
- Kobelco SK235SRLC Service Manual - 16468890Dokumen1.092 halamanKobelco SK235SRLC Service Manual - 16468890AntBelum ada peringkat
- 9.1 Design Qualification Protocol For Dynamic Pass BoxDokumen10 halaman9.1 Design Qualification Protocol For Dynamic Pass BoxKeval Patel100% (1)
- Who HvacDokumen22 halamanWho HvacAnas Abandeh100% (1)
- Plenum Box Sizing PDFDokumen2 halamanPlenum Box Sizing PDFLe HieuBelum ada peringkat
- HVAC Design For Hospital and Health FacilitiesDokumen62 halamanHVAC Design For Hospital and Health FacilitiesmostafaabdelrazikBelum ada peringkat
- Assignment 1 Indoor Air QualityDokumen11 halamanAssignment 1 Indoor Air Qualitymohd zakiBelum ada peringkat
- Housekeeping Procedures For Hotel Guest RoomsDokumen9 halamanHousekeeping Procedures For Hotel Guest RoomsFreddielity Galcon100% (2)
- SOPMS31 Validation of Laminar Air FlowDokumen2 halamanSOPMS31 Validation of Laminar Air FlowRahul Patil100% (5)
- Hvac Design For Healthcare FacilitiesDokumen60 halamanHvac Design For Healthcare FacilitiesSubir Kumar BiswasBelum ada peringkat
- HVAC Design For Healthcare FacilitiesDokumen60 halamanHVAC Design For Healthcare Facilitiesaymanibrahim_71Belum ada peringkat
- Guidelines Based On VDI 6022 PDFDokumen7 halamanGuidelines Based On VDI 6022 PDFbauer_mendoza3510100% (2)
- Syed Musadiq Isolation Room Design FinalDokumen57 halamanSyed Musadiq Isolation Room Design FinalAhmed Nabil100% (1)
- Energy & Water Conservation Code 2016Dokumen25 halamanEnergy & Water Conservation Code 2016keanncruz0% (1)
- HVAC Design For Corrosive EnvironmentDokumen29 halamanHVAC Design For Corrosive Environmentطاہر رضاBelum ada peringkat
- HVAC Design For Healthcare Facilities: Course No: M06-011 Credit: 6 PDHDokumen60 halamanHVAC Design For Healthcare Facilities: Course No: M06-011 Credit: 6 PDHNelson VargasBelum ada peringkat
- Ultra Clean Operating TheatreDokumen6 halamanUltra Clean Operating Theatreyogi_rulz_4evaBelum ada peringkat
- Hospital HVAC Design A Challenge For IAQ, Energy Recovery and System Reliability - Issue Jul-Sep 2002Dokumen11 halamanHospital HVAC Design A Challenge For IAQ, Energy Recovery and System Reliability - Issue Jul-Sep 2002Go Tze FongBelum ada peringkat
- Differences Between HVAC For Hospitals and That For Other BuildingsDokumen29 halamanDifferences Between HVAC For Hospitals and That For Other BuildingsMostafa Elmaghraby 467Belum ada peringkat
- HVAC in Hospital PDFDokumen7 halamanHVAC in Hospital PDFMohammed Toema100% (1)
- Handbook of Air Pollution Prevention and ControlDari EverandHandbook of Air Pollution Prevention and ControlPenilaian: 5 dari 5 bintang5/5 (2)
- HOD - Handing Over ProcessDokumen4 halamanHOD - Handing Over Processfayaz khanBelum ada peringkat
- Conversion of Operating Theatre From Positive To Negative Pressure EnvironmentDokumen17 halamanConversion of Operating Theatre From Positive To Negative Pressure EnvironmentHARI BASUKIBelum ada peringkat
- Hvac Systems in Hospitals PDFDokumen4 halamanHvac Systems in Hospitals PDFJuliana Orjuela GarciaBelum ada peringkat
- Trane CDQDokumen8 halamanTrane CDQh2odavidBelum ada peringkat
- Hospital Diffusers EngineeringDokumen26 halamanHospital Diffusers Engineeringamechmar5935100% (1)
- Weiser 2018Dokumen10 halamanWeiser 2018Syahrul MuhammadiyahBelum ada peringkat
- Effective of Ventilation System in Healthcare Facilities During Handling With Pandemic COVID-19 in Egypt Effective of Ventilation System in Healthcare Facilities During Handling Wi..Dokumen7 halamanEffective of Ventilation System in Healthcare Facilities During Handling With Pandemic COVID-19 in Egypt Effective of Ventilation System in Healthcare Facilities During Handling Wi..Widarma Atmaja, I KomangBelum ada peringkat
- RR in orDokumen3 halamanRR in orIan Joel MacayanBelum ada peringkat
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDokumen6 halamanEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSBelum ada peringkat
- Sustainability 11 01493Dokumen16 halamanSustainability 11 01493Yonas KebedeBelum ada peringkat
- Indoor Air Quality in HospitalsDokumen8 halamanIndoor Air Quality in HospitalsSamiYousifBelum ada peringkat
- Review Operating Room VentilationDokumen7 halamanReview Operating Room VentilationnaimakrukBelum ada peringkat
- Jamda: Richard M. Lynch PHD, Reginald Goring BsDokumen2 halamanJamda: Richard M. Lynch PHD, Reginald Goring BsWidarma Atmaja, I KomangBelum ada peringkat
- Pressure Management Health CareDokumen6 halamanPressure Management Health CareTeo Pei SanBelum ada peringkat
- Dono Harm Protecting Iaq inDokumen5 halamanDono Harm Protecting Iaq inShirun DingBelum ada peringkat
- Ventilation Performance in The Operating Theatre Against Airborne Infection Numerical Study On An Ultra-Clean SystemDokumen10 halamanVentilation Performance in The Operating Theatre Against Airborne Infection Numerical Study On An Ultra-Clean SystemVL KohBelum ada peringkat
- CHAPTER 9 Room Ventilation SystemsDokumen6 halamanCHAPTER 9 Room Ventilation SystemsJuan IntriagoBelum ada peringkat
- A Numerical Investigation About The Air Quality in A Surgical Room at A HospitalDokumen135 halamanA Numerical Investigation About The Air Quality in A Surgical Room at A HospitalHoàn LộcBelum ada peringkat
- Presented by Heena KousarDokumen50 halamanPresented by Heena KousarSreejil RaveendranBelum ada peringkat
- Air Distribution Strategy Impact On Operating Room Infection ControlDokumen7 halamanAir Distribution Strategy Impact On Operating Room Infection ControlGokhanUNLUBelum ada peringkat
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDokumen6 halamanEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSBelum ada peringkat
- Indoor Air QualityDokumen10 halamanIndoor Air QualityTajudeen IbrahimBelum ada peringkat
- CRISIS Ventilator A 3D Printed Option For Ventilator Surge in Mass Respiratory PandemicsDokumen8 halamanCRISIS Ventilator A 3D Printed Option For Ventilator Surge in Mass Respiratory PandemicsdjaroslavskyBelum ada peringkat
- The HVAC Systems Role in Environmental Infection Control 1585330997Dokumen7 halamanThe HVAC Systems Role in Environmental Infection Control 1585330997Abdülhamit KayyaliBelum ada peringkat
- Sustainability 14 11537 v3Dokumen17 halamanSustainability 14 11537 v3Naqqash SajidBelum ada peringkat
- CFD Modeling For Ventilation System of A Hospital Room: Alireza Kermani, PH.D Veryst Engineering, LLCDokumen15 halamanCFD Modeling For Ventilation System of A Hospital Room: Alireza Kermani, PH.D Veryst Engineering, LLCIbnu SufajarBelum ada peringkat
- Importance in HospitalDokumen3 halamanImportance in Hospitalsec435678Belum ada peringkat
- Jurnal OK-CovidDokumen8 halamanJurnal OK-CovidAchmad FauzyBelum ada peringkat
- Facility and Engineering Controls Using Usp 800 GuidelinesDokumen18 halamanFacility and Engineering Controls Using Usp 800 GuidelinesSantiago FalusBelum ada peringkat
- CFD Modeling For Ventilation System of A Hospital Room: Alireza Kermani Veryst EngineeringDokumen5 halamanCFD Modeling For Ventilation System of A Hospital Room: Alireza Kermani Veryst EngineeringIbnu SufajarBelum ada peringkat
- Effect of Ventilation Strategies On Infection Control Inside Operating Theatres PDFDokumen17 halamanEffect of Ventilation Strategies On Infection Control Inside Operating Theatres PDFValerika GurschiBelum ada peringkat
- HVAC Design For Healthcare Facilities R1Dokumen60 halamanHVAC Design For Healthcare Facilities R1Sagar BahiratBelum ada peringkat
- Designing Effective Ventilation Strategy For An Airborne InfectionDokumen18 halamanDesigning Effective Ventilation Strategy For An Airborne InfectionShohei Namjoon LetoBelum ada peringkat
- HVAC Systems For Environmental Control To Minimize The COVID-19 InfectionDokumen7 halamanHVAC Systems For Environmental Control To Minimize The COVID-19 InfectionRAMESH KRISHNAN LBelum ada peringkat
- Simulation-Based Feasibility Study of Improved Air Conditioning Systems For Hospital Operating RoomDokumen8 halamanSimulation-Based Feasibility Study of Improved Air Conditioning Systems For Hospital Operating RoomAsmaa ObiedBelum ada peringkat
- ARTICLE David N Schurk The HVAC Systems Roll in Environmental Infection Control For Hospitals REV 4 4 20 PDFDokumen7 halamanARTICLE David N Schurk The HVAC Systems Roll in Environmental Infection Control For Hospitals REV 4 4 20 PDFSundar RamasamyBelum ada peringkat
- M 334 ContentDokumen62 halamanM 334 ContentvirtechBelum ada peringkat
- Hospitals and Healthcare Facilities Connectivity CSE EbookDokumen54 halamanHospitals and Healthcare Facilities Connectivity CSE EbooksriramshankarBelum ada peringkat
- Controled Clean Operating Room AreaDokumen3 halamanControled Clean Operating Room AreaAnonymous 73gEYyEtLBelum ada peringkat
- Prevention of Infection in OTDokumen12 halamanPrevention of Infection in OTniraj_sdBelum ada peringkat
- MainDokumen6 halamanMaintrikusumawatiBelum ada peringkat
- Hospital EnvironmentDokumen21 halamanHospital EnvironmentVictor GodwinBelum ada peringkat
- Laminar Flow in Orthopaedic Operations - Essential If You CanDokumen15 halamanLaminar Flow in Orthopaedic Operations - Essential If You CanSamiYousifBelum ada peringkat
- Environmental Control Including Ventilation in Hospitals: Hospital NotesDokumen4 halamanEnvironmental Control Including Ventilation in Hospitals: Hospital NotesManisha GuptaBelum ada peringkat
- Monitoring Mechanical Ventilation Using Ventilator WaveformsDari EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsBelum ada peringkat
- 2 Single Villa+1 Duplex Villa (G+1+PH) : DC1 MW-602Dokumen1 halaman2 Single Villa+1 Duplex Villa (G+1+PH) : DC1 MW-602ZeeshanBelum ada peringkat
- 300 2732 Cat File LangDokumen60 halaman300 2732 Cat File LangZeeshanBelum ada peringkat
- Technical Data: Main Features and MaterialsDokumen2 halamanTechnical Data: Main Features and MaterialsZeeshanBelum ada peringkat
- GROHE Specification Sheet 3947300HDokumen1 halamanGROHE Specification Sheet 3947300HZeeshanBelum ada peringkat
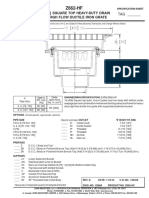
- 16 (406) Square Top Heavy-Duty Drain W/ High Flow Ductile Iron GrateDokumen1 halaman16 (406) Square Top Heavy-Duty Drain W/ High Flow Ductile Iron GrateZeeshanBelum ada peringkat
- PartsGuide Fall2020 WebDokumen61 halamanPartsGuide Fall2020 WebWilmar GuastiBelum ada peringkat
- Fumagalli Lights With CLX 15 Watt Lamp 3Dokumen1 halamanFumagalli Lights With CLX 15 Watt Lamp 3ZeeshanBelum ada peringkat
- Fumagalli Lights With CLX 15 Watt Lamp 1Dokumen1 halamanFumagalli Lights With CLX 15 Watt Lamp 1ZeeshanBelum ada peringkat
- Fumagalli Lights With CLX 15 Watt Lamp 2Dokumen1 halamanFumagalli Lights With CLX 15 Watt Lamp 2ZeeshanBelum ada peringkat
- Fumagalli Lights With CLX 15 Watt Lamp 4Dokumen1 halamanFumagalli Lights With CLX 15 Watt Lamp 4ZeeshanBelum ada peringkat
- Fumagalli Lights With CLX 15 Watt Lamp 5Dokumen1 halamanFumagalli Lights With CLX 15 Watt Lamp 5ZeeshanBelum ada peringkat
- Grundfosliterature 1580Dokumen284 halamanGrundfosliterature 1580ZeeshanBelum ada peringkat
- Construction Contracts - Law and Management (2015) 54Dokumen1 halamanConstruction Contracts - Law and Management (2015) 54ZeeshanBelum ada peringkat
- Karamura Time SwitchDokumen1 halamanKaramura Time SwitchZeeshan100% (2)
- TRANE Product Report - ERTAF 355 HE - 5.6 - 11.2Dokumen1 halamanTRANE Product Report - ERTAF 355 HE - 5.6 - 11.2ZeeshanBelum ada peringkat
- Construction Contracts - Law and Management (2015) 55Dokumen1 halamanConstruction Contracts - Law and Management (2015) 55ZeeshanBelum ada peringkat
- Construction Contracts - Law and Management (2015) 60Dokumen1 halamanConstruction Contracts - Law and Management (2015) 60ZeeshanBelum ada peringkat
- Concrete Plinths On Roof-ModelDokumen1 halamanConcrete Plinths On Roof-ModelZeeshanBelum ada peringkat
- Construction Contracts - Law and Management (2015) 58Dokumen1 halamanConstruction Contracts - Law and Management (2015) 58ZeeshanBelum ada peringkat
- Construction Contracts - Law and Management (2015) 56Dokumen1 halamanConstruction Contracts - Law and Management (2015) 56ZeeshanBelum ada peringkat
- Construction Contracts - Law and Management (2015) 59Dokumen1 halamanConstruction Contracts - Law and Management (2015) 59ZeeshanBelum ada peringkat
- Bionik: The Brushless Automated Barrier With Digital ThinkingDokumen10 halamanBionik: The Brushless Automated Barrier With Digital ThinkingZeeshanBelum ada peringkat
- Construction Contracts - Law and Management (2015) 61Dokumen1 halamanConstruction Contracts - Law and Management (2015) 61ZeeshanBelum ada peringkat
- Grundfosliterature 5564731Dokumen90 halamanGrundfosliterature 5564731Jeremias Villafañe100% (1)
- TemperzoneCLEVERAHU DaveSmithDokumen57 halamanTemperzoneCLEVERAHU DaveSmithZeeshanBelum ada peringkat
- Fire Hydrant 20 PsiDokumen2 halamanFire Hydrant 20 PsiZeeshanBelum ada peringkat
- Water Heater Section DrawingDokumen1 halamanWater Heater Section DrawingZeeshanBelum ada peringkat
- List Air-Changes PurificationDokumen109 halamanList Air-Changes PurificationHZM PCCWBelum ada peringkat
- Ansi - Ahri 850 2004Dokumen12 halamanAnsi - Ahri 850 2004mpwasaBelum ada peringkat
- 01 Mag NAPure LCOperators ManualDokumen204 halaman01 Mag NAPure LCOperators Manual章洪建100% (1)
- SHARP PCI Humidifiers Product BrochureDokumen8 halamanSHARP PCI Humidifiers Product BrochurerfbruneiBelum ada peringkat
- STRATEGIC ACTION PLAN - Step by StepDokumen4 halamanSTRATEGIC ACTION PLAN - Step by StepBERNADETTE GUERRABelum ada peringkat
- CASE 2 Philips India Launch of New Air Purifiers PDFDokumen15 halamanCASE 2 Philips India Launch of New Air Purifiers PDFHarshit 2207Belum ada peringkat
- Cleanrooms & Air Quality - A Risk-Based Approach - Tim SandleDokumen13 halamanCleanrooms & Air Quality - A Risk-Based Approach - Tim SandleHubert BonamisBelum ada peringkat
- Infection Control Risk Assessment (ICRA) : Precaution ClassDokumen2 halamanInfection Control Risk Assessment (ICRA) : Precaution ClassFaozan FikriBelum ada peringkat
- MM - 4a.pdf BREAK SYSTEME AXEL TECH PDFDokumen16 halamanMM - 4a.pdf BREAK SYSTEME AXEL TECH PDFRachid SmailiBelum ada peringkat
- ICRA Form v08.07Dokumen5 halamanICRA Form v08.07Indra Juang Putra HarefaBelum ada peringkat
- LindeTechnology 1-04 Biotechnology EngDokumen6 halamanLindeTechnology 1-04 Biotechnology EngTarif_87Belum ada peringkat
- OilMistSmoke ODR2000Dokumen2 halamanOilMistSmoke ODR2000Mandrak FantomBelum ada peringkat
- Storm AP-1516D - Individual Brochure FlipbookDokumen8 halamanStorm AP-1516D - Individual Brochure FlipbookAlvina David SelvamBelum ada peringkat
- Silent Killers Mold-Free Home ChecklistDokumen7 halamanSilent Killers Mold-Free Home ChecklistpsymahBelum ada peringkat
- Aaf Brochure High Purity Housings and Hepa Ulpa Filters en OnlineDokumen28 halamanAaf Brochure High Purity Housings and Hepa Ulpa Filters en OnlineJose BalaguerBelum ada peringkat
- Evaluation of Air Assay Media by The Monodisperse DOP (Dioctyl Phthalate) Smoke TestDokumen5 halamanEvaluation of Air Assay Media by The Monodisperse DOP (Dioctyl Phthalate) Smoke TestShaker QaidiBelum ada peringkat
- New HEPA Al SepDokumen2 halamanNew HEPA Al Seppham hoang quanBelum ada peringkat
- Item # Hd18, Hepa Pleat Ii: Air Otek, IncDokumen3 halamanItem # Hd18, Hepa Pleat Ii: Air Otek, IncDylan UnrauBelum ada peringkat
- Chemcap Clearview and Pro2 BrochureDokumen6 halamanChemcap Clearview and Pro2 BrochureSheila Rose Bacerra-VillafloresBelum ada peringkat
- MSFC STD 246eDokumen91 halamanMSFC STD 246eJoseph DavidBelum ada peringkat
- Iso 29463-1-2017Dokumen24 halamanIso 29463-1-2017Amr Mohamed ElbhrawyBelum ada peringkat
- User's Manual: Labconco CorporationDokumen62 halamanUser's Manual: Labconco CorporationCeleynes RTBelum ada peringkat
- Air Filtration in HVAC SystemsDokumen9 halamanAir Filtration in HVAC SystemsusamaBelum ada peringkat
- Technical Guide For Kevlar® in Mechanical Rubber Goods PDFDokumen21 halamanTechnical Guide For Kevlar® in Mechanical Rubber Goods PDFpurnashBelum ada peringkat