Anda mungkin juga menyukai
- Recommendations For Resistance Exercise in Cardiac Rehabilitation. Recommendations of The German FederationDokumen10 halamanRecommendations For Resistance Exercise in Cardiac Rehabilitation. Recommendations of The German FederationmaracioBelum ada peringkat
- 1 s2.0 S144395061501269X Main4Dokumen10 halaman1 s2.0 S144395061501269X Main4maracioBelum ada peringkat
- Comparison of Different Forms of Exercise Training in Patients With Cardiac Disease: Where Does High-Intensity Interval Training Fit?Dokumen10 halamanComparison of Different Forms of Exercise Training in Patients With Cardiac Disease: Where Does High-Intensity Interval Training Fit?maracioBelum ada peringkat
- Ni Hms 537812Dokumen15 halamanNi Hms 537812maracioBelum ada peringkat
- This Item Is The Archived Peer-Reviewed Author-Version ofDokumen48 halamanThis Item Is The Archived Peer-Reviewed Author-Version ofmaracioBelum ada peringkat
- Sharada Prasad Yadav, Aqeel Ahmad, Brijesh Kumar Pandey, Dharamsheela Singh, Neeta Asthana, Richa Verma, Raj Kamal Tripathi, Jimut Kanti GhoshDokumen13 halamanSharada Prasad Yadav, Aqeel Ahmad, Brijesh Kumar Pandey, Dharamsheela Singh, Neeta Asthana, Richa Verma, Raj Kamal Tripathi, Jimut Kanti GhoshmaracioBelum ada peringkat
- The Influence of Training Characteristics On The Effect of Exercise TrainingDokumen7 halamanThe Influence of Training Characteristics On The Effect of Exercise TrainingmaracioBelum ada peringkat
- This Item Is The Archived Peer-Reviewed Author-Version ofDokumen48 halamanThis Item Is The Archived Peer-Reviewed Author-Version ofmaracioBelum ada peringkat
- 1 s2.0 S2405587515300263 MainDokumen8 halaman1 s2.0 S2405587515300263 MainmaracioBelum ada peringkat
- Journal of Microscopy and Ultrastructure: Tapan Guha, Heena Kohad, Radhaballabh BharDokumen6 halamanJournal of Microscopy and Ultrastructure: Tapan Guha, Heena Kohad, Radhaballabh BharmaracioBelum ada peringkat
- Journal of Microscopy and Ultrastructure: Tapan Guha, Heena Kohad, Radhaballabh BharDokumen6 halamanJournal of Microscopy and Ultrastructure: Tapan Guha, Heena Kohad, Radhaballabh BharmaracioBelum ada peringkat
- Accelerated Boundary Integral Method For Multiphase Flow in Non-Periodic GeometriesDokumen54 halamanAccelerated Boundary Integral Method For Multiphase Flow in Non-Periodic GeometriesmaracioBelum ada peringkat
- Tumor Necrosis Factor-Alpha and Interleukin-6 Gene Polymorphisms in Iranian Patients With Ischemic Heart FailureDokumen5 halamanTumor Necrosis Factor-Alpha and Interleukin-6 Gene Polymorphisms in Iranian Patients With Ischemic Heart FailuremaracioBelum ada peringkat
- Journal of Microscopy and Ultrastructure: Tapan Guha, Heena Kohad, Radhaballabh BharDokumen6 halamanJournal of Microscopy and Ultrastructure: Tapan Guha, Heena Kohad, Radhaballabh BharmaracioBelum ada peringkat
- Biomarkers of Inflammation in Heart FailureDokumen1 halamanBiomarkers of Inflammation in Heart FailuremaracioBelum ada peringkat
- Biomarkers of Inflammation in Heart FailureDokumen1 halamanBiomarkers of Inflammation in Heart FailuremaracioBelum ada peringkat
- Petersen Et Al-2006-Congestive Heart FailureDokumen5 halamanPetersen Et Al-2006-Congestive Heart FailuremaracioBelum ada peringkat
- NIH Public AccessDokumen14 halamanNIH Public AccessmaracioBelum ada peringkat
- NIH Public AccessDokumen14 halamanNIH Public AccessmaracioBelum ada peringkat
- Cytokine S Sing The BluesDokumen9 halamanCytokine S Sing The BluesmaracioBelum ada peringkat
- Exercise Builds Brain Health Key Roles of Growth Factor Cascades and Inflammation PDFDokumen9 halamanExercise Builds Brain Health Key Roles of Growth Factor Cascades and Inflammation PDFmaracioBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Sahya Part 4Dokumen116 halamanSahya Part 4Homeopathy Torrents100% (1)
- Criminalistic 4 :)Dokumen47 halamanCriminalistic 4 :)William Bryle PertosBelum ada peringkat
- ART 1 AkimaDokumen8 halamanART 1 AkimaNat LesBelum ada peringkat
- Anatomy and Physiology Assignment 1Dokumen8 halamanAnatomy and Physiology Assignment 1api-238869728Belum ada peringkat
- The Adaptations To Strength Training - Morphological and Neurological Contributions To Increased Strength PDFDokumen24 halamanThe Adaptations To Strength Training - Morphological and Neurological Contributions To Increased Strength PDFLeonBelum ada peringkat
- Effect of Endurance Trainingg On Parameters of Aerobic FitnessDokumen14 halamanEffect of Endurance Trainingg On Parameters of Aerobic FitnessClaudia LoughnaneBelum ada peringkat
- MMMDokumen182 halamanMMMAlastair Harris100% (2)
- Physiological Effects of MassageDokumen1 halamanPhysiological Effects of MassagehannahBelum ada peringkat
- The Muscle Pump Potential Mechanisms and ApplicationsDokumen6 halamanThe Muscle Pump Potential Mechanisms and ApplicationsDan InsignaresBelum ada peringkat
- Chad Waterbury - Muscle RevolutionDokumen293 halamanChad Waterbury - Muscle RevolutionBigNat777486% (7)
- DAFTAR PUSTAKA NeuroDokumen3 halamanDAFTAR PUSTAKA NeuroAtikacahyanipBelum ada peringkat
- Russian Current 2011Dokumen14 halamanRussian Current 2011Faisal Qureshi100% (1)
- MCAT Content MasterlistDokumen24 halamanMCAT Content MasterlistTrang LamBelum ada peringkat
- Anatomy and Physiology Notes For Exam 3Dokumen58 halamanAnatomy and Physiology Notes For Exam 3mike921gold100% (2)
- Demands in Ice HockeyDokumen16 halamanDemands in Ice Hockeysara_damato10Belum ada peringkat
- Chemical Wizardry CompleteDokumen132 halamanChemical Wizardry CompleteSaeed Khushal100% (5)
- Differential Effects of Attentional Focus Strategies During Long-Term Resistance TrainingDokumen10 halamanDifferential Effects of Attentional Focus Strategies During Long-Term Resistance TrainingMiklós BalatinczBelum ada peringkat
- Exercise Programs: Training Guidelines, Fitt Principles, Endurance, Muscle and Bone-Strengthening Activities: Team Sports (Basketball)Dokumen15 halamanExercise Programs: Training Guidelines, Fitt Principles, Endurance, Muscle and Bone-Strengthening Activities: Team Sports (Basketball)Heroe SedicoBelum ada peringkat
- IndividualityDokumen2 halamanIndividualityMiyangBelum ada peringkat
- Pe 11 Module 6weeks6Dokumen11 halamanPe 11 Module 6weeks6Ailyn RoncalesBelum ada peringkat
- S6 Biology SB August 2018Dokumen421 halamanS6 Biology SB August 2018UMUFASHA Ange Justifiee100% (1)
- Pex 02 03 PDFDokumen6 halamanPex 02 03 PDFCourtney Sims83% (6)
- Anatomy, physiology & kinesiology worksheet for exercise healthDokumen22 halamanAnatomy, physiology & kinesiology worksheet for exercise healthLuiz Henrique MacielBelum ada peringkat
- Chap09 Strength TrainingDokumen43 halamanChap09 Strength Trainingdivesh pandeyBelum ada peringkat
- Training & Nutrition Insider Secrets For A Lean-BodyDokumen65 halamanTraining & Nutrition Insider Secrets For A Lean-BodyfredaBelum ada peringkat
- Cell Specialization LabDokumen19 halamanCell Specialization LabKayseri PersaudBelum ada peringkat
- Cristhian Thibaudeau - Black Book of Training SecretsDokumen222 halamanCristhian Thibaudeau - Black Book of Training Secretskfox0918Belum ada peringkat
- Multiple-Choice Test Chapter 11: Respiration and Gas ExchangeDokumen2 halamanMultiple-Choice Test Chapter 11: Respiration and Gas ExchangesybejoboBelum ada peringkat
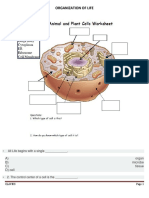
- Organization of LifeDokumen6 halamanOrganization of LifeVina SihombingBelum ada peringkat
- Soft Tissue Therapy EmagDokumen29 halamanSoft Tissue Therapy EmagSE TanBelum ada peringkat