Anda mungkin juga menyukai
- Nursing Research Exam SampleDokumen9 halamanNursing Research Exam SampleMarlchiel Nathan ArregladoBelum ada peringkat
- Family Nursing Care PlanDokumen5 halamanFamily Nursing Care PlanMarlchiel Nathan ArregladoBelum ada peringkat
- Session Module SampleDokumen18 halamanSession Module SampleMarlchiel Nathan ArregladoBelum ada peringkat
- Nursing Scenario Intervention SampleDokumen2 halamanNursing Scenario Intervention SampleMarlchiel Nathan ArregladoBelum ada peringkat
- Heart DiseaseDokumen21 halamanHeart DiseaseMarlchiel Nathan ArregladoBelum ada peringkat
- Session Module SampleDokumen18 halamanSession Module SampleMarlchiel Nathan ArregladoBelum ada peringkat
- Nursing Scenario SampleDokumen8 halamanNursing Scenario SampleMarlchiel Nathan ArregladoBelum ada peringkat
- Nursing Scenario ActivityDokumen12 halamanNursing Scenario ActivityMarlchiel Nathan ArregladoBelum ada peringkat
- Family Nursing Care PlanDokumen5 halamanFamily Nursing Care PlanMarlchiel Nathan ArregladoBelum ada peringkat
- Research Compiled As of January 26Dokumen133 halamanResearch Compiled As of January 26Marlchiel Nathan ArregladoBelum ada peringkat
- What Is Aseptic TechniqueDokumen11 halamanWhat Is Aseptic TechniqueMarlchiel Nathan ArregladoBelum ada peringkat
- Nutrition ConceptsDokumen1 halamanNutrition ConceptsMarlchiel Nathan ArregladoBelum ada peringkat
- BSN Quiz Mood DisorderDokumen22 halamanBSN Quiz Mood DisorderMarlchiel Nathan ArregladoBelum ada peringkat
- Induced AbortionDokumen11 halamanInduced AbortionMarlchiel Nathan ArregladoBelum ada peringkat
- St. Paul University Philippines: Summary of Findings, Conclusions and RecommendationsDokumen8 halamanSt. Paul University Philippines: Summary of Findings, Conclusions and RecommendationsMarlchiel Nathan ArregladoBelum ada peringkat
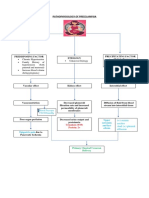
- Pathophysiology of PreeclampsiaDokumen1 halamanPathophysiology of PreeclampsiaMarlchiel Nathan ArregladoBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Cardiovascular SystemDokumen9 halamanCardiovascular SystemWild RiftBelum ada peringkat
- Physiology of Heart in DetailDokumen101 halamanPhysiology of Heart in Detailakanksha sharmaBelum ada peringkat
- PCCN PrepDokumen133 halamanPCCN Prepdaniel100% (2)
- Physical Examination of the Cardiovascular SystemDokumen26 halamanPhysical Examination of the Cardiovascular SystemJoseph De JoyaBelum ada peringkat
- A Soft Total Artificial Heart-First Concept Evaluation OnDokumen11 halamanA Soft Total Artificial Heart-First Concept Evaluation OnSeyit Hamza ÇavgaBelum ada peringkat
- Contrapulsatore Aortico Autocat 2 Wave Education MaterialsDokumen52 halamanContrapulsatore Aortico Autocat 2 Wave Education MaterialsJose Moreno100% (1)
- Heart Anatomy Jeopardy GameDokumen43 halamanHeart Anatomy Jeopardy GameLaura HajdukiewiczBelum ada peringkat
- ICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular HypertrophyDokumen5 halamanICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular Hypertrophysamir raflaBelum ada peringkat
- Integrated Cardiovascular Physiology: A Laboratory ExerciseDokumen70 halamanIntegrated Cardiovascular Physiology: A Laboratory ExercisefireworkrwBelum ada peringkat
- Cath Lab Essentials: Basic Hemodynamics For The Cath Lab and ICUDokumen38 halamanCath Lab Essentials: Basic Hemodynamics For The Cath Lab and ICUDr. TomBelum ada peringkat
- Congestive Cardiac FailureDokumen49 halamanCongestive Cardiac FailureHampson MalekanoBelum ada peringkat
- Clinical Case 1Dokumen31 halamanClinical Case 1reginaBelum ada peringkat
- Cardiovascular System Heart ReviewerDokumen8 halamanCardiovascular System Heart ReviewerImmanuel Cris PalasigueBelum ada peringkat
- Anatomy and Cardiovascular AssessmentDokumen52 halamanAnatomy and Cardiovascular AssessmentNaomi Anne AsuntoBelum ada peringkat
- 11 Biology Notes ch18 Body Fluids and Circulation PDFDokumen8 halaman11 Biology Notes ch18 Body Fluids and Circulation PDFSumit SinghalBelum ada peringkat
- Heart Failure Mechanisms and Assessment FindingsDokumen9 halamanHeart Failure Mechanisms and Assessment Findingssarasmith1988Belum ada peringkat
- Update - in AnestesiaDokumen200 halamanUpdate - in AnestesiaInês MendonçaBelum ada peringkat
- Timing Booklet enDokumen12 halamanTiming Booklet enanonBelum ada peringkat
- Pediatrics 1981 Versmold 607 13Dokumen9 halamanPediatrics 1981 Versmold 607 13Andrés AcevedoBelum ada peringkat
- CH 11 Cardiovascular-SystemDokumen113 halamanCH 11 Cardiovascular-SystemHazel Banday100% (1)
- Cardiology - Valvular Disease PDFDokumen2 halamanCardiology - Valvular Disease PDFPshtiwan MahmoodBelum ada peringkat
- Echocardiogrphy Instrumentasi and Color Doppler. 2023 Ir CahyoDokumen90 halamanEchocardiogrphy Instrumentasi and Color Doppler. 2023 Ir CahyoJalu PanjongkoBelum ada peringkat
- CardiacDokumen32 halamanCardiacAlli OmerBelum ada peringkat
- Cardiac Contractility: Factors Affecting Strength of Heart Muscle ContractionDokumen4 halamanCardiac Contractility: Factors Affecting Strength of Heart Muscle ContractionzaidBelum ada peringkat
- Cardiovascular Diseases and DengueDokumen242 halamanCardiovascular Diseases and DengueHazel Amador MasionBelum ada peringkat
- Lood Vessel Structure An Function: Objectives MaterialsDokumen9 halamanLood Vessel Structure An Function: Objectives MaterialsArthur HamadaBelum ada peringkat
- Heart AnatomyDokumen19 halamanHeart Anatomydeepika kushwahBelum ada peringkat
- Uterine Blood Flow During Supine Rest and Exercise in Late PregnancyDokumen9 halamanUterine Blood Flow During Supine Rest and Exercise in Late PregnancyMD Luthfy LubisBelum ada peringkat
- 2012 Wilderness Basics Course NotebookDokumen90 halaman2012 Wilderness Basics Course NotebookU8x58Belum ada peringkat
- Hemodynamic MonitoringDokumen10 halamanHemodynamic MonitoringDivya Joy100% (1)