Anda mungkin juga menyukai
- After The Class Students Will Be Able To Gain Knowledge About TriageDokumen3 halamanAfter The Class Students Will Be Able To Gain Knowledge About TriageRahul DamorBelum ada peringkat
- Synopsis FinalDokumen10 halamanSynopsis FinalGEORGE HONNALLIBelum ada peringkat
- Assignment On Burns 2Dokumen15 halamanAssignment On Burns 2Suby Beigh100% (2)
- International Journal of Trend in Scientific Research and Development (IJTSRD)Dokumen16 halamanInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDBelum ada peringkat
- Shift Work Disorder and Associated Health Problems Among Nursing Staffs Working in A Tertiary Health Centre, Chennai, South IndiaDokumen4 halamanShift Work Disorder and Associated Health Problems Among Nursing Staffs Working in A Tertiary Health Centre, Chennai, South IndiaInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- MSC Nursing Dissertation Synopsis: Era University LucknowDokumen19 halamanMSC Nursing Dissertation Synopsis: Era University LucknowNazia GulzarBelum ada peringkat
- Knowledge and Practice of Nurses Towards Peripheral Intravenous Cannulation in Pediatric Patients in Selected Public Hospitals Khartoum - SudanDokumen5 halamanKnowledge and Practice of Nurses Towards Peripheral Intravenous Cannulation in Pediatric Patients in Selected Public Hospitals Khartoum - SudanInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- A Study To Assess The Effectiveness of Structure Teaching Programme On Knowledge Regarding Prevention of Childhood Accidents Among Mothers of Under Five Children at Piparia, Vadodara.Dokumen8 halamanA Study To Assess The Effectiveness of Structure Teaching Programme On Knowledge Regarding Prevention of Childhood Accidents Among Mothers of Under Five Children at Piparia, Vadodara.International Organization of Scientific Research (IOSR)Belum ada peringkat
- Assesment For Burns and Fluid Calculation PDFDokumen10 halamanAssesment For Burns and Fluid Calculation PDFRagaviBelum ada peringkat
- College of Nursing Berhampur: Seminar ON Nightingale'S TheoryDokumen11 halamanCollege of Nursing Berhampur: Seminar ON Nightingale'S TheoryAmlan jyoti thanapatiBelum ada peringkat
- Assignment ON: S.G.R.D Institute of Nursing, Pandger, (Asr)Dokumen4 halamanAssignment ON: S.G.R.D Institute of Nursing, Pandger, (Asr)Charan0% (1)
- NCP On AppendicitisDokumen7 halamanNCP On Appendicitisshweta singhBelum ada peringkat
- SPRITUAL Synopsis. FinalDokumen14 halamanSPRITUAL Synopsis. Finalsapna chauhanBelum ada peringkat
- Time Specific Objective Content Teaching Learning Activities Evaluati ONDokumen20 halamanTime Specific Objective Content Teaching Learning Activities Evaluati ONAnnette BainesBelum ada peringkat
- Unit Time (HRS) Learning Objective Teaching Learning Activities EvaluationDokumen12 halamanUnit Time (HRS) Learning Objective Teaching Learning Activities EvaluationSAYMABANUBelum ada peringkat
- 2 5 17 991Dokumen6 halaman2 5 17 991Science JournalBelum ada peringkat
- ASSIGNMENT ON Distance by KaminiDokumen9 halamanASSIGNMENT ON Distance by Kaminikamini ChoudharyBelum ada peringkat
- A Study to Assess the Effectiveness of Video Assisted Teaching Module on Knowledge Regarding Myocardial Infarction and its Prevention among the Patients Attending Diabetic Clinic at BVV Sangha’s HSK Hospital and Research Centre, BagalkotDokumen3 halamanA Study to Assess the Effectiveness of Video Assisted Teaching Module on Knowledge Regarding Myocardial Infarction and its Prevention among the Patients Attending Diabetic Clinic at BVV Sangha’s HSK Hospital and Research Centre, BagalkotInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Lesson Plan of BurnsDokumen24 halamanLesson Plan of BurnsjrkedridgemwanakalandoBelum ada peringkat
- Demostration of Wound DressingDokumen10 halamanDemostration of Wound DressingDanish00rizviBelum ada peringkat
- International Journal of Trend in Scientific Research and Development (IJTSRD)Dokumen4 halamanInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDBelum ada peringkat
- ScoringDokumen53 halamanScoringKaran SinghBelum ada peringkat
- Pathophysiology On ArrhythmiaDokumen34 halamanPathophysiology On ArrhythmiaYhr Yh100% (1)
- Hemorrhage and ShockDokumen22 halamanHemorrhage and ShockaparnaBelum ada peringkat
- Care Plan Pneumonia CompressDokumen18 halamanCare Plan Pneumonia CompressAahad AmeenBelum ada peringkat
- Geriatric Considerations IN Nursing: Seminar ONDokumen52 halamanGeriatric Considerations IN Nursing: Seminar ONSree LathaBelum ada peringkat
- Demonstration On ParacentesisDokumen10 halamanDemonstration On ParacentesisDeepika PrajapatiBelum ada peringkat
- TRACHEOSTOMY CARE (Repaired) (Repaired)Dokumen18 halamanTRACHEOSTOMY CARE (Repaired) (Repaired)DhAiRyA ArOrABelum ada peringkat
- Synopsis Proforma For Registration of Subjects For DissertationDokumen16 halamanSynopsis Proforma For Registration of Subjects For DissertationJyotiBelum ada peringkat
- Assissment of A.V AidsDokumen10 halamanAssissment of A.V AidsPriyaBelum ada peringkat
- LESSON PLAN On Paedritric Nurse RolesDokumen3 halamanLESSON PLAN On Paedritric Nurse Rolesbuhari rabiuBelum ada peringkat
- Effectiveness of Structured Teaching Programme On Knowledge Regarding Acid Peptic Disease and Its Prevention Among The Industrial WorkersDokumen6 halamanEffectiveness of Structured Teaching Programme On Knowledge Regarding Acid Peptic Disease and Its Prevention Among The Industrial WorkersIJAR JOURNALBelum ada peringkat
- 'MUHS RESEARCH - Final - 1-1Dokumen31 halaman'MUHS RESEARCH - Final - 1-1Reshma rsrBelum ada peringkat
- Seminar On Education and TrainingDokumen20 halamanSeminar On Education and TrainingScott MonroeBelum ada peringkat
- Master Rotation Plan For ANM (As Per Revised Syllabus 2013)Dokumen10 halamanMaster Rotation Plan For ANM (As Per Revised Syllabus 2013)akritiBelum ada peringkat
- Treatment Aspects in Perioperative NursingDokumen51 halamanTreatment Aspects in Perioperative NursingShibin Jacob100% (2)
- 4302 M.Sc. OBSTETRIC AND GYNAECOLOGICAL NURSINGDokumen89 halaman4302 M.Sc. OBSTETRIC AND GYNAECOLOGICAL NURSINGSteny Ann VargheseBelum ada peringkat
- Bedside ClinicDokumen35 halamanBedside ClinicJoanna RachelBelum ada peringkat
- Assessment of Respiratory SystemDokumen23 halamanAssessment of Respiratory Systemjrflores1284Belum ada peringkat
- Document 1management of Nursing Educational InstitutionDokumen13 halamanDocument 1management of Nursing Educational InstitutionHardeep Kaur100% (1)
- PHILOSOPHY of EducationDokumen2 halamanPHILOSOPHY of EducationJisna AlbyBelum ada peringkat
- Child AbuseDokumen19 halamanChild Abuseshivani dasBelum ada peringkat
- Master Rotation Plan - BSNDokumen5 halamanMaster Rotation Plan - BSNPreeti ChouhanBelum ada peringkat
- Front&6 THDokumen196 halamanFront&6 THselbalBelum ada peringkat
- Refractive ErrorDokumen6 halamanRefractive Errortri erdiansyahBelum ada peringkat
- Geriatric Considerations in Nursing: Priyanka. T M SC Nursing 1 YearDokumen70 halamanGeriatric Considerations in Nursing: Priyanka. T M SC Nursing 1 Yearsanthiyasandy100% (1)
- B M W M: IO Edical Aste AnagementDokumen23 halamanB M W M: IO Edical Aste AnagementJishnu JohnBelum ada peringkat
- Common Paediatric Skin Conditions & BirthmarksDokumen10 halamanCommon Paediatric Skin Conditions & Birthmarksdr.nadia sharifBelum ada peringkat
- CRT On RTMDokumen16 halamanCRT On RTMNithiya Nadesan0% (1)
- Physical Examination 2003Dokumen39 halamanPhysical Examination 2003Gayatri MudliyarBelum ada peringkat
- B.SC Nursing - 2018 - Question Papers - Third Year - Child Health Nursing FR 16Dokumen1 halamanB.SC Nursing - 2018 - Question Papers - Third Year - Child Health Nursing FR 16SAGAR ADHAOBelum ada peringkat
- Women &mental HealthDokumen16 halamanWomen &mental HealthDhAiRyA ArOrABelum ada peringkat
- D. Thulasimani: The Tamilnadu DR MGR Medical UniversityDokumen121 halamanD. Thulasimani: The Tamilnadu DR MGR Medical UniversitymeenaBelum ada peringkat
- Case Study 2Dokumen37 halamanCase Study 2api-391842100Belum ada peringkat
- Aswi Editted Copy ProjectDokumen127 halamanAswi Editted Copy ProjectVasantha KumariBelum ada peringkat
- Assertiveness: Presented by Maj Mercy Jacob 1 Year M SC Trainee OfficerDokumen24 halamanAssertiveness: Presented by Maj Mercy Jacob 1 Year M SC Trainee OfficerMercy JacobBelum ada peringkat
- Warning Signs of Various DiseasesDokumen44 halamanWarning Signs of Various DiseasesamsabavanBelum ada peringkat
- Assignment On Pharamcological Aspects - BY KAMINI2Dokumen9 halamanAssignment On Pharamcological Aspects - BY KAMINI2kamini ChoudharyBelum ada peringkat
- Independent Practice IssuesDokumen40 halamanIndependent Practice IssuesHarish Kumar KumawatBelum ada peringkat
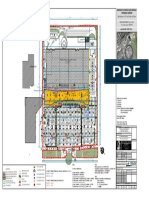
- Calea Bucuresti, Nr. 107, Mun. Brasov, Jud. Brasov: Modernizare Si Extindere Galerii Comerciale Hypermarket CarrefourDokumen1 halamanCalea Bucuresti, Nr. 107, Mun. Brasov, Jud. Brasov: Modernizare Si Extindere Galerii Comerciale Hypermarket CarrefourBogdan UrsuBelum ada peringkat
- Minnesota Burn Surge Education: Emergency Preparedness and ResponseDokumen95 halamanMinnesota Burn Surge Education: Emergency Preparedness and ResponseBogdan UrsuBelum ada peringkat
- Burn Injury Model of Care PDFDokumen61 halamanBurn Injury Model of Care PDFAde AnugerahBelum ada peringkat
- 67 Pediatric Burn Injuries in The Developing World FINAL PDFDokumen57 halaman67 Pediatric Burn Injuries in The Developing World FINAL PDFBogdan UrsuBelum ada peringkat
- Slides AdvancedDokumen8 halamanSlides AdvancedBogdan UrsuBelum ada peringkat
- Burn Injury Model of CareDokumen29 halamanBurn Injury Model of CareBogdan UrsuBelum ada peringkat
- Burn Injury Model of Care PDFDokumen61 halamanBurn Injury Model of Care PDFAde AnugerahBelum ada peringkat
- 67 Pediatric Burn Injuries in The Developing World FINALDokumen10 halaman67 Pediatric Burn Injuries in The Developing World FINALBogdan UrsuBelum ada peringkat
- Proforma For Registration of Subject ForDokumen27 halamanProforma For Registration of Subject ForBogdan UrsuBelum ada peringkat
- WOHLFARTH C. - CRC Handbook of Thermodynamic Data of Polymer Solutions at Elevated Pressures - (CRC PRESS 2005 648 P) PDFDokumen648 halamanWOHLFARTH C. - CRC Handbook of Thermodynamic Data of Polymer Solutions at Elevated Pressures - (CRC PRESS 2005 648 P) PDFdavidnps100% (1)
- 23 - Eave StrutsDokumen2 halaman23 - Eave StrutsTuanQuachBelum ada peringkat
- Lens NeutralisationDokumen3 halamanLens Neutralisationzahra aliBelum ada peringkat
- Business Description: Apollo TyresDokumen4 halamanBusiness Description: Apollo TyresSrijit SahaBelum ada peringkat
- Rangtong Shentong ViewDokumen19 halamanRangtong Shentong Viewlongjim31100% (1)
- Watch Out For Flying Pumpkins: BOE Member PromotedDokumen16 halamanWatch Out For Flying Pumpkins: BOE Member PromotedelauwitBelum ada peringkat
- Unit 1 - Theoretical Framework PDFDokumen67 halamanUnit 1 - Theoretical Framework PDFMeli EujaniánBelum ada peringkat
- Polymer Structures: Issues To Address..Dokumen34 halamanPolymer Structures: Issues To Address..Eugene Embalzado Jr.Belum ada peringkat
- STPM Mathematics T Past Year Question P1 P2 P3Dokumen19 halamanSTPM Mathematics T Past Year Question P1 P2 P3Sou Voyage0% (3)
- MEC Threads ChartDokumen12 halamanMEC Threads ChartenricoBelum ada peringkat
- Marshall Abby - Chess Cafe - The Openings Explained - 1-63, 2015-OCR, 682pDokumen682 halamanMarshall Abby - Chess Cafe - The Openings Explained - 1-63, 2015-OCR, 682pArtur MałkowskiBelum ada peringkat
- REE0913ra LegazpiDokumen6 halamanREE0913ra LegazpiScoopBoyBelum ada peringkat
- Proposed Revisions To Usp Sterile Product - Package Integrity EvaluationDokumen56 halamanProposed Revisions To Usp Sterile Product - Package Integrity EvaluationDarla Bala KishorBelum ada peringkat
- Session 1Dokumen4 halamanSession 1Vidhi VermaBelum ada peringkat
- R K Konodia Civil Gate Previous Year - by EasyEngineering - Net 1 PDFDokumen214 halamanR K Konodia Civil Gate Previous Year - by EasyEngineering - Net 1 PDFDaante VermaBelum ada peringkat
- 0900-9914 I1 201012 PDFDokumen132 halaman0900-9914 I1 201012 PDFIvan Arjona50% (2)
- AidsDokumen22 halamanAidsVicky Singh100% (2)
- Worktips 01 Priming of PavementsDokumen2 halamanWorktips 01 Priming of PavementsDilhara WickramaarachchiBelum ada peringkat
- Enzymes MCQsDokumen2 halamanEnzymes MCQsNobody's PerfectBelum ada peringkat
- P1 - Duct Design IntroductionDokumen30 halamanP1 - Duct Design IntroductionAndryx MartinezBelum ada peringkat
- Stephane Moses The Angel of History Rosenzweig Benjamin Scholem PDFDokumen196 halamanStephane Moses The Angel of History Rosenzweig Benjamin Scholem PDFlivehuman100% (3)
- Off-Line Programming Techniques For Multirobot Cooperation SystemDokumen17 halamanOff-Line Programming Techniques For Multirobot Cooperation SystemShaw MxBelum ada peringkat
- Advent of SkyscrapersDokumen27 halamanAdvent of SkyscrapersJoshua AlboBelum ada peringkat
- Mungbean 03india PDFDokumen194 halamanMungbean 03india PDFSrujana PatelBelum ada peringkat
- System Substation Commissioning TestsDokumen8 halamanSystem Substation Commissioning TestsCvijayakumar100% (1)
- G 10 ICT WorkSheetc 2.2 English MDokumen8 halamanG 10 ICT WorkSheetc 2.2 English MMohamaad SihatthBelum ada peringkat
- Key-Sentence Writing 1Dokumen23 halamanKey-Sentence Writing 1Thảo VyBelum ada peringkat
- BR Safetymatrix enDokumen12 halamanBR Safetymatrix enHamidreza MoaddeliBelum ada peringkat
- Marine Upholstery SpecsDokumen1 halamanMarine Upholstery SpecsRezza KurniawanBelum ada peringkat
- School of Chemical Engineering - 20Dokumen372 halamanSchool of Chemical Engineering - 20biroutiBelum ada peringkat