Roos, Karen L. Greenlee, John E. - Meningitis and Encephalitis
Diunggah oleh
Nadila Nur PratiwiJudul Asli
Hak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
Roos, Karen L. Greenlee, John E. - Meningitis and Encephalitis
Diunggah oleh
Nadila Nur PratiwiHak Cipta:
Format Tersedia
Review Article
Meningitis and
Address correspondence to
Dr John E. Greenlee, Clinical
Neuroscience Center, 175 N
Medical Drive E, 5th Floor, Salt
Lake City, UT 84132,
john.greenlee@hsc.utah.edu.
Relationship Disclosure:
Encephalitis
Dr Roos is the editor-in-chief Karen L. Roos, MD, FAAN; John E. Greenlee, MD, FAAN
of Seminars in Neurology and
has received compensation
for legal work. Dr Greenlee
has received personal ABSTRACT
compensation for activities
with Perseid Therapeutics Purpose of Review: Neurologists have a vital role in the recognition of meningitis and
as a consultant and has encephalitis, the accurate evaluation and interpretation of CSF studies, and the man-
served in an editorial capacity agement and prevention of the neurologic complications of CNS infectious diseases.
for Medlink.
Unlabeled Use of
Recent Findings: Although the tetravalent meningococcal glycoconjugate vaccine has
Products/Investigational decreased the incidence of meningococcal meningitis, the vaccine does not contain sero-
Use Disclosure: Dr Roos group B, which is responsible for one-third of cases of meningococcal disease. Thus, menin-
and Dr Greenlee report no
disclosure.
gitis due to Neisseria meningitidis is still a concern in a vaccinated individual. Empiric therapy
Copyright * 2011, for meningitis associated with sinusitis, otitis, or mastoiditis should include antibiotic therapy
American Academy of for anaerobes. An organism that classically causes a subacute or chronic meningitis, such as
Neurology. All rights Mycobacterium tuberculosis, may on occasion present with an acute onset of symptoms.
reserved.
Summary: Unlike most other diseases, the management of patients with suspected
meningitis or encephalitis begins with empiric therapy. The etiologic organism cannot
always be identified. The goal is to identify those that are treatable, provide supportive
care for those that are not, and, when possible, prevent the neurologic complications
of these infections.
Continuum Lifelong Learning Neurol 2011;17(5):1010–1023.
INTRODUCTION trauma or neurosurgical procedures or
Meningitis and encephalitis are neuro- through congenital or acquired defects
logic emergencies. In the hospital set- in the skull or spinal column. Meningitis
ting, the initial realization that a patient due to entry of organisms through
has a CNS infectious disease is usually congenital or acquired defects in the
made by the emergency department phy- skull or spinal column should be sus-
sician or, if the patient is already ad- pected in patients with recurrent epi-
mitted, by the primary service. For this sodes of meningitis. Acquired defects
reason, neurologic consultation may be are usually the result of closed head
delayed, and time is almost always of the trauma and occur at sites where the
essence in reaching an accurate diagno- bones of the skull are thinnest: over
sis and initiating treatment. the frontal, ethmoidal, or sphenoidal
sinuses or bony structures adjacent to
ACUTE MENINGITIS the middle ear or mastoid. Acquired
Bacterial Meningitis skull base defects may be accompanied
Bacterial meningitis is most commonly by CSF rhinorrhea or otorrhea if the
caused by hematogenous spread of meninges are breached, but not all skull
bacteria from a remote site of infection. base defects are associated with rhino-
Meningitis may also develop from the rrhea or otorrhea. It is important to
spread of organisms through emissary remember that an interval of many years
veins from infected sinuses, middle ear, may separate an episode of significant
or mastoid. Bacteria may enter the sub- closed head trauma and the onset of
arachnoid space following penetrating meningitis.
1010 www.aan.com/continuum October 2011
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
Causative agents of acute bacterial gram-negative bacilli, or anaerobes. S. h The most common
meningitis. The agents causing bacte- aureus is a common causative organ- causative organisms of
rial meningitis vary with the age of the ism in patients with penetrating head bacterial meningitis in
patient, the route by which infection is trauma. children and adults are
acquired, and the presence of associ- The organisms associated with bacte- Streptococcus
ated or predisposing conditions. rial meningitis in patients who are im- pneumoniae and
The most common etiologic organ- munocompromised vary with the type Neisseria meningitidis.
ism of bacterial meningitis in neonates of immune deficiency. Individuals with h The tetravalent
and infants is Streptococcus agalactiae defects of cell-mediated immunity, meningococcal
(group B streptococci), followed in order which includes very young infants, preg- glycoconjugate vaccine
of frequency by Escherichia coli, other nant woman, the elderly, and patients does not contain
gram-negative bacilli, and Listeria mono- who are immunocompromised as a re- serogroup B, which
cytogenes. Meningitis due to S. agalactiae sult of organ transplantation, malignancy, is responsible for
occurs at two points in time: within 48 AIDS, or immunosuppressive medica- one-third of cases of
meningococcal disease.
hours of the postnatal period or at 7 days tions, have an increased prevalence of
to 6 weeks of age. Cases occurring in the meningitis due to L. monocytogenes or h Meningitis associated
immediate postnatal period are due to ac- mycobacteria. Patients with defects of hu- with sinusitis,
quisition of the organism from the mother moral immune response (and patients otitis, or mastoiditis
may be due to
at the time of birth, and meningitis often who have undergone splenectomy) are at
streptococci, anaerobes,
occurs as part of a systemic infection. risk for fulminant meningitis with S.
Staphylococcus aureus,
Cases of S. agalactiae meningitis in older pneumoniae or, less frequently, N. men- Haemophilus, or
neonates are usually not accompanied by ingitidis. Patients with neutropenia are Enterobacteriaceae,
other evidence of systemic infection. susceptible to meningitis caused by Pseu- and empiric coverage
The most common causative organ- domonas aeruginosa and by gram- should include
isms of bacterial meningitis in children negative enteric bacteria. meropenem or
and adults are Streptococcus pneumo- Chronic meningitis presenting metronidazole.
niae and Neisseria meningitidis. The acutely. A number of etiologic organ- h Patients with defective
tetravalent meningococcal glycocon- isms that typically cause a subacute or cell-mediated
jugate vaccine has decreased the inci- chronic meningitis may on occasion immunity, such as
dence of meningococcal meningitis. present with acute onset of symptoms. infants, the elderly,
The vaccine does not contain serogroup This is especially true for tuberculous and individuals who are
B, which is responsible for one-third of meningitis but may occasionally occur immunosuppressed,
cases of meningococcal disease.1 with fungal meningitides due to Cryp- may develop meningitis
Meningitis associated with sinusitis, oti- tococcus neoformans, Histoplasma due to Listeria
monocytogenes.
tis, or mastoiditis may be due to strepto- capsulatum, Coccidioides immitis, or
cocci, anaerobes, Staphylococcus aureus, other agents. The most urgent of these is
Haemophilus, or Enterobacteriaceae. tuberculous meningitis, and presumptive
Meningitis in the postneurosurgical treatment should be initiated if the
patient may be due to staphylococci, condition is suspected (Case 3-1).
Case 3-1
A 21-year-old Laotian woman presented to the emergency department with
severe headache, fever, confusion, and difficulty with gait. Examination
revealed confusion, nuchal rigidity, bilateral Babinski signs, and ataxia. CT
scan demonstrated basilar meningeal inflammation and a mild increase in
ventricular size. CSF analysis revealed 150 white blood cells/mm3, 45%
Continued on page 1012
Continuum Lifelong Learning Neurol 2011;17(5):1010–1023 www.aan.com/continuum 1011
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Meningitis and Encephalitis
KEY POINTS
h Empiric therapy for
tuberculous meningitis
Continued from page 1011
should be initiated in
polymorphonuclear leukocytes and 55% mononuclear cells, a protein of
patients with fever,
230 mg/dL, and a glucose of 30 mg/dL. No organisms were seen on Gram
headache, and stiff
stain, and both acid-fast smear and PCR for mycobacteria were negative.
neck; a CSF lymphocytic
The patient was treated with isoniazid (300 mg/d), rifampin (600 mg/d),
pleocytosis; and a mild
pyrazinamide (2 g/d), and ethambutol (2.5 g/d) on suspicion of tuberculous
to moderate decrease in
meningitis. CSF was obtained by high cervical puncture, and 3 weeks later
glucose concentration
Mycobacterium tuberculosis grew in culture. A chest x-ray demonstrated
(less than 40 mg/dL but
innumerable small pulmonary opacities consistent with miliary tuberculosis.
greater than 20 mg/dL).
Comment. Ancillary studies such as a chest radiograph are helpful in
h Cases of mycobacterial patients with CNS infections. Skin testing with purified protein derivative
or fungal meningitis may initially be negative but then become positive as the patient improves
presenting acutely may during the course of therapy. In patients with fungal or tuberculous
resemble bacterial meningitis, a high cervical puncture may demonstrate the organism when
meningitis. lumbar puncture does not.
Therapy for tuberculous meningitis is recommended in the patient with
fever, headache, and stiff neck, with or without cranial nerve deficits
associated with a CSF lymphocytic pleocytosis and a mild to moderately
decreased glucose concentration (less than 40 mg/dL but greater than
20 mg/dL). Evidence of basilar meningeal enhancement and hydrocephalus
on neuroimaging further supports the need for empiric therapy for
tuberculous meningitis.
Viral Meningitis young person may go to sleep with
Many of the viruses causing viral men- mild symptoms and never awaken.
ingitis have a seasonal distribution Typical symptoms are fever, headache,
(Table 3-1). Most cases of viral menin- photophobia, vomiting, and an altered
gitis are due to enteroviruses and occur level of consciousness (Case 3-2). Pa-
in summer or early autumn, although tients may or may not complain of neck
occasional cases may occur throughout stiffness. Seizures may occur early in
the year. Meningitis associated with meningitis in up to 40% of affected
West Nile virus has a similar seasonal children and may also occur in adults.
distribution, as does meningitis asso- Presentation with focal seizures or focal
ciated with other arthropodborne vi- neurologic symptoms, however, should
ruses. The exception to this rule is raise concern of brain abscess, cere-
Colorado tick fever, which tends to britis, or cerebrovascular complications.
occur in late spring or early summer. Cases of mycobacterial or fungal men-
ingitis presenting acutely may resemble
Clinical Presentation of bacterial meningitis. Patients with viral
Acute Meningitis meningitis are usually less overtly ill,
Bacterial meningitis may be preceded and they never have an altered level
by 3 to 5 days of insidiously progressive of consciousness or new-onset seizure
malaise, fever, irritability, or vomiting; activity unless encephalitis has devel-
develop over 1 to 2 days; or have a oped. Neurologists are critical in helping
fulminant presentation.2 Bacterial men- non-neurologists distinguish between a
ingitis remains one of the few condi- patient with bacterial meningitis, who
tions in which a previously healthy should be admitted to and observed in
1012 www.aan.com/continuum October 2011
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TABLE 3-1 Major Agents of Viral Meningitis
Mechanism
Family Genus Agents of Spread Peak Season
Picornaviridae Enterovirus Coxsackieviruses Fecal-oral Summer to
contamination early autumn
Echoviruses
Enterovirus 71 and other
numbered enteroviruses
Herpesviridae Herpesvirus Herpes simplex virus type 2a Human contact No seasonal
distribution
Togaviridae Flavivirus West Nile virus Mosquito Summer to
early autumn
St. Louis virus
Bunyaviridae Orthobunyavirus California virus/La Crosse virus Mosquito Summer to
early autumn
Reoviridae Orbivirus Colorado tick fever Tick Late spring to
early summer
Arenaviridae Arenavirus Lymphocytic choriomeningitis Airborneb Autumn and
virus winterb
Retroviridae HIV Human contactc No seasonal
distribution
a
Herpes simplex virus type 2 meningitis may occur as an isolated event or may be recurrent.
b
Lymphocytic choriomeningitis virus is classically associated with exposure to infected wild mice and is most common during autumn or
winter when mice tend to move indoors. Infection may also occur year-round after exposure to infected pet hamsters.
c
Meningitis in HIV usually has its onset early in the course of systemic infection, at the time of seroconversion.
the intensive care unit, and a patient alteration in consciousness, and nuchal
with viral meningitis, who is not at risk rigidity, keeping in mind that these
for additional complications. findings are not present in all patients.
Presentation in coma is an ominous
Bedside Diagnosis prognostic sign. The classic tests for
of Meningitis meningeal irritation are resistance to
Bacterial meningitis should be consid- passive flexion of the neck (nuchal
ered in any patient presenting with fever, rigidity), Kernig sign, and Brudzinski
Case 3-2
A 62-year-old woman had been in good health until 4 days prior to admission, when she reported shaking
chills, cough, and purulent sputum production to her husband. Two days prior to admission she reported
a headache. On the day of admission, her husband found her unresponsive in the early morning hours
and called an ambulance. She was brought first to an outlying facility and then transferred.
On examination, the patient was diaphoretic and unresponsive. Pulse was 108 beats/min, blood
pressure was 108/84 mm Hg, and temperature was 39.8-C (103.6-F). General physical examination was
unremarkable except for rales over the right lower lung field and nuchal rigidity with a positive
Brudzinski sign. Fundi showed flat disks but absent venous pulsations. Blood cultures were obtained,
and empiric therapy for bacterial meningitis and herpes simplex virus type 1 encephalitis was initiated
with dexamethasone, ceftriaxone, vancomycin, ampicillin, and acyclovir.
Continued on page 1014
Continuum Lifelong Learning Neurol 2011;17(5):1010–1023 www.aan.com/continuum 1013
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Meningitis and Encephalitis
Continued from page 1013
Complete blood count showed a white blood cell count of 15,000 2/L with 85% neutrophils and 5%
bands. CT scan was unremarkable. Lumbar puncture revealed an opening pressure of 430 mm H2O,
turbid fluid, 2290 white blood cells/mm3, 95% polymorphonuclear leukocytes, a protein of 410 mg/dL,
and a glucose of 28 mg/dL with a blood glucose of 125 mg/dL. Gram stain showed innumerable
polymorphonuclear leukocytes and occasional lancet-shaped gram-positive diplococci.
The patient was treated with dexamethasone, ceftriaxone, vancomycin, and ampicillin pending
cultures, and subsequently antimicrobial therapy was modified after Streptococcus pneumoniae was
isolated and antibiotic sensitivities demonstrated the organism was sensitive to ceftriaxone.
Comment. Empiric adjunctive and antimicrobial therapy is initiated for bacterial meningitis, herpes
simplex virus type 1 encephalitis, and tickborne bacterial infections (during the season when ticks are
biting) immediately after blood cultures are obtained and prior to CT and CSF analysis. Empiric therapy is
then modified when the results of CSF analysis and antimicrobial sensitivity testing are known.
sign. Kernig sign is present when resis- when other tests are negative. It is im-
tance to passive extension of the leg at portant to keep in mind that elderly
the knee is present. Although Brudzinski patients with extensive cervical spine
developed several tests to detect menin- disease may have neck stiffness, and
geal irritation, the maneuver most com- occasionally patients with influenza and
monly referred to as Brudzinski sign severe myalgias may also report neck
involves spontaneous flexion of the hips pain. In both groups of patients, pain
and knees when the neck is passively and resistance to movement usually oc-
flexed. Brudzinski sign is the more sen- cur not only upon flexion but also upon
sitive of the two. Both signs, when pres- lateral rotation. Patients with meningi-
ent, are strongly suggestive of meningeal tis, however, can usually turn the head
irritation; however, they were developed even if neck stiffness to flexion is pres-
in the preantibiotic era when meningitis ent. Particular attention should be paid
was frequently advanced at the time of to the presence of cutaneous rashes,
presentation and may not be detected petechiae, or purpura suggestive of me-
early in the course of infection. In awake ningococcemia; pulmonary consolida-
patients, a more sensitive test is to ask tion suggestive of pneumonia due to
patients to put their chin on their chest S. pneumoniae; or cardiac murmurs
with the mouth closed. Keeping the suggestive of endocarditis.
mouth closed is important, because
patients experiencing pain on flexion Atypical Presentations
may hold their neck still but touch their of Meningitis
chin to their chest by opening the jaw In neonates, bacterial meningitis may
widely. One of the most sensitive tests present with tachypnea, apneic spells,
of nuchal rigidity is a test that was de- changes in heart rate, atypical seizures,
veloped during the days of the polio or simply vague decline. Although a
epidemic and involves asking the pa- feeble, high-pitched cry in an infant has
tient to kiss his or her knee (in children, been said to suggest meningitis, this is
who consider this request perfectly not a reliable sign. Similarly, a bulging
reasonable) or, in adults, to touch the fontanelle is a late sign, indicating sig-
forehead to the knee. This test will of- nificantly increased intracranial pressure.
ten detect meningeal irritation at a time Individuals who are immunocompromised,
1014 www.aan.com/continuum October 2011
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
such as neonates, may not develop fever cose should also be sent to determine h The causative organisms
or nuchal rigidity. Patients with alcohol- the CSF:blood glucose ratio. Expedi- of bacterial meningitis
ism presenting in the setting of severe tious handing of CSF by the laboratory can often be detected in
inebriation may have meningitis without is important because cells may adhere blood cultures.
clearly detectable signs. Meningitis may to the collecting tube over time, result- h CSF should be
also be deceptively asymptomatic in the ing in lower CSF cell counts, and examined for white
elderly, and the only sign of meningitis leukocytes may lyse in extremely puru- blood cells within 90
may be confusion in a previously alert lent CSF.4 minutes of collection.
older patient or altered responsiveness in Typical CSF findings in bacterial h CSF glucose
a patient who already has dementia. In meningitis include elevated opening concentrations will be
these patients, as well as in neonates, the pressure, fluid that is often, but not higher in moderately to
threshold for CSF analysis should be low. always, turbid, elevated white blood cell severely hyperglycemic
However, patients with alcoholism and count consisting predominantly of poly- patients. In these
elderly patients are also at risk for falls and morphonuclear leukocytes, elevated patients, the CSF:blood
subdural hematomas. In such patients, protein concentration, and depressed glucose ratio should be
it is appropriate to begin antimicrobial CSF:blood glucose ratio. A CSF:blood used to determine the
therapy and obtain a head CT scan or MRI glucose ratio of less than 0.3 is highly true CSF glucose
before CSF analysis. The onset of bacterial correlated with bacterial meningitis. In concentration. The CSF
glucose concentration
meningitis following neurosurgical proce- evaluating CSF glucose concentrations,
is low when the
dures is often insidious, developing over it is important to remember that CSF
CSF:blood glucose ratio
hours or days. Patients in this setting are glucose values will be higher in moder- is less than 0.6.
at increased risk, as an alteration of ately to severely hyperglycemic patients
consciousness or neck stiffness may be and that changes in CSF glucose con- h CSF bacterial PCRs are
increasingly available.
attributed to the expected postoperative centrations may lag 30 to 120 minutes
Specific diagnosis of the
course. behind those in blood. Protein con- causative organism of
centrations in meningitis are a reflec- bacterial meningitis and
Laboratory Diagnosis tion of blood-brain barrier injury but determination of
of Meningitis usually range between 100 mg/dL and antibiotic sensitivity
Although bacterial meningitis is sus- 500 mg/dL.4 require bacterial culture.
pected on the basis of the clinical Specific identification of the infect-
presentation and physical examination ing organism involves Gram stain, cul-
findings, definitive diagnosis is made by ture, and PCR. Gram stain provides
analysis of the CSF. If intracranial pres- the most rapid initial identification of
sure is greatly increased, there is a risk of the organism. Detection of organisms
brain herniation independent of, but on Gram stain requires approximately
also associated with, lumbar puncture, 100,000 organisms/mm3.5 Errors in
and the likelihood of fatal herniation Gram stain may result from careless
cannot be reliably predicted from CT or handling of CSF, inadequate efforts to
MRI.3 In severely ill patients in whom resuspend bacteria if CSF has been
very high intracranial pressure is sus- allowed to settle, and errors in de-
pected, the most prudent course is to colorization or reading of the slide.
begin empiric therapy and wait until A 16S ribosomal RNA conserved se-
CSF pressure has been controlled be- quence broad-based bacterial PCR is
fore performing lumbar puncture. The routinely available in most hospital
organism can often be identified in laboratories. Additionally, a number
blood cultures. CSF should be sent for of meningeal-specific PCRs detect
cell count with differential, protein and N. meningitidis or S. pneumoniae nu-
glucose concentration, Gram stain, cul- cleic acid in CSF, as well as a number
ture, and PCR. Simultaneous blood glu- of other meningeal pathogens, but
Continuum Lifelong Learning Neurol 2011;17(5):1010–1023 www.aan.com/continuum 1015
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Meningitis and Encephalitis
TABLE 3-2 CSF Abnormalities in Acute Meningitis
Type of
Meningitis Cellsa Protein Glucose Specific Diagnosis
Bacterial Polymorphonuclear Elevated G50% of Gram stain
meningitis leukocytes blood
Bacterial culture
glucose
PCR
Tuberculous Variable pleocytosis, Elevated G50% of Acid-fast stainb
meningitis usually with blood
PCR
lymphocytes 9 glucose
polymorphonuclear Culture
leukocytes
Fungal Lymphocytes Elevated G50% of Cryptococcal polysaccharide antigen
meningitis blood
Histoplasma polysaccharide antigen Coccidioides
glucose
immitis complement fixation antibody
India ink and culture
c
Viral Lymphocytes Elevated 950% of Reverse transcriptase PCR for enteroviruses
meningitis blood
PCR herpes simplex virus type 2
glucose
Immunoglobulin M (West Nile or other arboviruses)
a
Cell count, glucose, and protein may be minimally abnormal in patients who are severely immunocompromised.
b
In tuberculous meningitis, diagnosis by CSF acid-fast smear has a low sensitivity, diagnostic reliability of PCR is only 50%, and culture
requires up to 7 weeks. For this reason, tuberculous meningitis is treated as described in Case 3-1.
c
CSF during the first 24 to 48 hours of viral meningitis may exhibit a mixed pleocytosis with predominance of polymorphonuclear leukocytes.
these are not routinely available. Speci- crobial sensitivity testing are known
fic diagnosis of the causative organism (Table 3-3).
of bacterial meningitis and determina- Therapy of chronic meningitis pre-
tion of antibiotic sensitivity require senting acutely. Specific diagnosis of
bacterial culture. Although this is rou- tuberculous meningitis can be difficult:
tine in most hospitals, it may be help- yield by PCR approaches 50%, and
ful to alert the laboratory in advance sensitivity of culture (which may take
if anaerobic infection or other un- up to 6 weeks) is only 70%.4 Thus, ther-
usual organisms or culture require- apy for tuberculous meningitis should
ments are anticipated. Yield on culture be initiated presumptively if the diagnosis
can be reduced by prior antibiotic ther- is suspected (Table 3-4). Treatment of
apy. Table 3-2 is a list of the expected fungal meningitis is usually not begun
CSF results in meningitis due to bac- empirically unless organisms are seen
teria, viruses, mycobacteria, and fungi. in CSF.
Treatment of viral meningitis. Most
Treatment of Acute Meningitis cases of viral meningitis resolve spon-
Antibiotic therapy for bacterial men- taneously. The headache may persist
ingitis. Antibiotic therapy for bacterial for months and can be managed with
meningitis is initially empiric and then amitriptyline and nonsteroidal anti-
specific once the pathogen has been inflammatory agents. Limited data sug-
identified and the results of antimi- gest that pleconaril may shorten the
1016 www.aan.com/continuum October 2011
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TABLE 3-3 Antibiotics for Empiric Therapy of Bacterial Meningitis
Age and Associated
Conditions Probable Organism Antibiotic Therapy
Preterm infants Staphylococcus aureus (nosocomial) Vancomycin plus ceftazidime
Gram-negative bacilli
Neonates Group B streptococci Ampicillin plus cefotaxime
Escherichia coli
Other gram-negative bacilli
Listeria monocytogenes
Children and adults Streptococcus pneumoniae Third-generation (ceftriaxone or
cefotaxime) or fourth-generation
Neisseria meningitidis
(cefepime) cephalosporin plus
vancomycin
Adults over the age of 55 S. pneumoniae Third-generation (ceftriaxone or
cefotaxime) or fourth-generation
L. monocytogenes
(cefepime) cephalosporin plus
Gram-negative bacilli vancomycin plus ampicillin
Haemophilus influenzae
Meningitis in the setting S. pneumoniae Third-generation (ceftriaxone or
of sinusitis, otitis, or known cefotaxime) or fourth-generation
Haemophilus
CSF leak (cefepime) cephalosporin plus
Gram-negative bacilli vancomycin plus meropenem or
metronidazole
Anaerobic or microaerophilic streptococci
Bacteroides fragilis
S. aureus
Head trauma, neurosurgical S. aureus Vancomycin plus ceftazidime or
procedures, shunt infections vancomycin plus meropenem
Staphylococcus epidermidis
Gram-negative bacilli
S. pneumoniae
States of impaired cellular L. monocytogenes Third-generation (ceftriaxone or
immunity, including AIDS cefotaxime) or fourth-generation
Gram-negative bacilli
(cefepime) cephalosporin plus
S. pneumoniae vancomycin plus ampicillin
H. influenzae
duration of headache in enteroviral Corticosteroid therapy in meningi-
meningitis, but the drug is not rou- tis. The realization that neurologic injury
tinely available.5 Acyclovir is efficacious in bacterial meningitis is due to the host
in treating herpes simplex virus type 2 inflammatory response has led to a focus
(HSV-2) meningitis, and prophylactic on controlling this aspect of men-
therapy with acyclovir, valacyclovir, or ingitis. Early studies in children with
famciclovir is efficacious in preventing Haemophilus influenzae meningitis
recurrent meningitis due to HSV-2. who were treated with cefotaxime plus
Continuum Lifelong Learning Neurol 2011;17(5):1010–1023 www.aan.com/continuum 1017
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Meningitis and Encephalitis
a
TABLE 3-4 Antimicrobial Therapy for Tuberculous Meningitis
Drug Usual Daily Dose Maximum Dose Duration
Isoniazid 5 mg/kg to 10 mg/kg 300 mg 6 to 9 months
Rifampin 10 mg/kg to 20 mg/kg 600 mg 6 months
Pyrazinamide 15 mg/kg to 30 mg/kg 2000 mg 2 months
Ethambutol 15 mg/kg to 25 mg/kg 2500 mg 2 months
Streptomycin 15 mg/kg 1000 mg 2 months
a
Multiple drug regimens (four or more) should be used when a high probability of drug resistance exists.
dexamethasone demonstrated an Other measures to treat cerebral
effect on the CSF inflammatory re- edema. Patients presenting with papil-
sponse and a decreased incidence of ledema or signs of impending brain
deafness compared with those treated herniation warrant emergent treatment
with cefotaxime alone.6 More recently, for increased intracranial pressure. Ele-
studies from EuropeVincluding a na- vation of the head of the bed to 30
tionwide prospective study from the degrees will often reduce pressure
Netherlands in which dexamethasone somewhat. Hyperventilation to a PCO2
was used in all patients above 16 years of 27 mm Hg to 30 mm Hg will cause
of age with pneumococcal meningitisV intracranial vasoconstriction and may be
demonstrated reduced mortality rates lifesaving over the short term. This
and neurologic sequelae in patients usually requires intubation and paraly-
with pneumococcal meningitis treated sis, and in some cases the patient will
with dexamethasone begun at the ini- already be hyperventilating to that level.
tiation of antibiotic therapy (class III In children, 0.5 g/kg to 2.0 g/kg of
evidence).7,8 Dexamethasone is given mannitol is given intravenously over 30
as 10 mg intravenously, beginning im- minutes and repeated as needed. The
mediately prior to or with the initial adult dosage is a 1.0 g/kg bolus re-
dose of antibiotics, followed by 10 mg peated as needed every 3 to 4 hours or
intravenously every 6 hours for 4 days. 0.25 g/kg every 2 to 3 hours. Pentobar-
Early institution of dexamethasone and bital coma has been used in extreme
antibiotic therapy appears to be cru- cases, but no controlled data exist for
cial, and dexamethasone has not been its use in meningitis. Decompressive
shown to be effective in less-developed craniectomy is not normally used in
countries where patients tend to pres- meningitis because the cerebral involve-
ent later in the course of their dis- ment is diffuse rather than focal. Surgery
ease.8 The role of dexamethasone in may be required, however, to drain an
tuberculous or fungal meningitides is accompanying brain abscess or para-
less well established. In tuberculous meningeal focus of infection. For more
meningitis, dexamethasone has been re- information, refer to the article ‘‘Eval-
ported to decrease mortality but not uation and Management of Increased
neurologic sequelae in survivors.9 As Intracranial Pressure’’ in this issue of
with bacterial meningitis, however, .
the utility of dexamethasone may de- Other complications of meningitis
pend on its use early in the course of requiring treatment. Bacterial menin-
infection. gitis may be accompanied by a variety
1018 www.aan.com/continuum October 2011
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
of neurologic and systemic complica- the presence and development of in- h In the patient with
tions, many of which may also occur in creased opening pressure. Opening basilar meningitis
tuberculous meningitis. Bacterial men- pressure should be measured at the with basal ganglia
ingitis arising from sinusitis or otitis may time of the initial lumbar puncture and ischemia or infarction,
be complicated by epidural abscess, any time a change in the neurologic ex- tuberculous meningitis
subdural empyema, brain abscess, or amination occurs. A time-honored prac- and cryptococcal
venous sinus thrombosis, any of which tice has been to perform daily lumbar meningitis should be
may require emergent surgery. Seizures punctures and reduce the opening pres- considered.
require emergent treatment with lora- sure by 50% using a manometer. In h In patients with
zepam, phenytoin (fosphenytoin), or reality, daily lumbar punctures are often bacterial, mycobacterial,
more aggressive therapy such as phe- not effective, and it is best to use a or fungal meningitis,
nobarbital or pentobarbital coma in ventriculostomy instead. prognosis is influenced
patients who fail to respond. Hypona- by the level of
tremia may be caused by cerebral salt Prognosis consciousness at the
time of presentation
wasting, the syndrome of inappropriate In most series, mortality has correlated
and the rapidity of
secretion of antidiuretic hormone, or IV with obtundation or coma. Factors as-
antimicrobial therapy
fluids. Subdural effusions are common sociated with poor prognosis include initiation.
in children with meningitis; these do age older than 60 years, concomitant
not usually require drainage and may be debilitating diseases, low Glasgow
followed by CT or MRI. Patients may Coma Scale score on admission, focal
develop cerebral vasculitis, stroke, or neurologic deficits, and low CSF cell
spontaneous intracranial hemorrhage.10 count.10Y12 Seizures have predicted a
Myelitis, although not usually consid- worse outcome in some studies, as has
ered a complication of bacterial men- low CSF:serum glucose ratio.11 Mortal-
ingitis, has been reported in 2.3% of ity in tuberculous meningitis is in the
patients with pneumococcal meningi- range of 25%, with good recovery in
tis.10 Bacterial sepsis and shock may be only 50% of patients.13 As in bacterial
present, as may disseminated in- meningitis, prognosis is significantly
travascular coagulation, and, in the influenced by the level of conscious-
case of N. meningitidis, Waterhouse- ness on presentation and the rapid
Friderichsen syndrome with wide- institution of appropriate therapy. Viral
spread hemorrhage and adrenal failure. meningitis is usually self-limited.
Cases of meningitis associated with
S. aureus and, less often, S. pneumo- ENCEPHALITIS
niae may be a complication of bacterial In patients with an altered level of
endocarditis. Meningitis in the presence consciousness or an acute confusional
of S. pneumoniae endocarditis is often state, the first question to ask is
accompanied by rapid destruction of whether the patient has encephalitis
the aortic valve. Basilar meningitis with or an encephalopathy. If the patient has
basal ganglia ischemia or infarction can encephalitis, the next question to ask is
occur in both tuberculous meningitis and whether he or she has encephalitis that
cryptococcal meningitis. The basilar men- can be treated with antimicrobial agents
ingitis that occurs in tuberculous menin- or encephalitis that is treated with sup-
gitis may produce obstructive rather than portive care only (Case 3-3).
communicating hydrocephalus.
Fungal meningitis. Recommenda- Etiology
tions for the antimicrobial therapy of The presence of fever and headache
fungal meningitis are readily available, with an altered level of consciousness
but neurologists must be vigilant about makes encephalitis more likely than
Continuum Lifelong Learning Neurol 2011;17(5):1010–1023 www.aan.com/continuum 1019
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Meningitis and Encephalitis
KEY POINTS
h The most common
identifiable etiologic
Case 3-3
A 20-year-old college junior was brought to the emergency department by
organisms of
her boyfriend because of a 3-day history of fever, headache, and
encephalitis are
intermittent confusion. On examination, she had a temperature of 38-C
herpesviruses
(100.4-F), was oriented to self but not to date or place, and had difficulty
(eg, herpes simplex
following commands. The boyfriend denied alcohol or illicit drug use.
virus type 1 or
Complete blood count with differential was normal. Noncontrast cranial
varicella-zoster virus),
CT scan was normal. CSF analysis demonstrated 100 white blood cells/mm3,
a tickborne bacterial
lymphocytic predominance, 700 red blood cells/mm3, a glucose
infection, or an
concentration of 47 mg/dL, and a protein concentration of 56 mg/dL.
arthropodborne virus.
The patient was treated empirically with acyclovir for herpes simplex virus
h Neuroinvasive disease (HSV) encephalitis based on her clinical presentation and CSF analysis. CSF
due to West Nile virus, PCR for HSV-1 DNA was obtained as well as serum and CSF immunoglobulin G
St. Louis encephalitis (IgG) antibodies to determine a serum:CSF antibody ratio.
virus, or Japanese Comment. The CSF PCR should be positive, as she is 3 days into her illness,
encephalitis virus but it is likely too early to detect the intrathecal synthesis of antibodies.
may present with Antibodies do not appear in CSF until 8 days after symptom onset but may
encephalitis, a flaccid, be detectable for up to 3 months. HSV IgG on serum and CSF should be
weak limb (a obtained. A serum:CSF ratio of less than 20:1 is diagnostic of HSV encephalitis.
poliomyelitis syndrome), Fluid-attenuated inversion recovery (FLAIR) sequences and diffusion-weighted
or parkinsonian imaging (DWI) magnetic resonance scans are indicated and would be
features. expected to demonstrate an area of increased signal intensity in the temporal
lobe. In 90% of adults with HSV encephalitis, an area of increased signal
intensity is seen in the temporal lobe on T2-weighted images, FLAIR
sequences, and DWI within 48 hours of symptom onset.
encephalopathy. The etiologic organ- Nile virus, and rabies have been trans-
ism of the encephalitis can be predicted mitted from organ donor to recipient.
based on the following: (1) the time of
year, (2) prodromal symptoms (eg, Clinical Presentation
flulike illness in West Nile virus infec- Patients with encephalitis have fever
tion), (3) area of residence, (4) travel and headache and one or more of the
and occupational and recreational activ- following: confusion, behavioral ab-
ities, (5) rash (eg, varicella, meningo- normalities, depressed level of con-
coccemia, Rocky Mountain spotted sciousness, focal neurologic deficits,
fever), (6) contact with animals, and and new-onset seizure activity.
(7) immunosuppression from medica- Certain features, or a combination
tions, malignancy, chronic corticoste- of features, suggest a specific etiology.
roid use, or organ transplantation.14 Patients with West Nile virus may have a
The most common identifiable etio- tremor, a history of diarrhea, or a macu-
logic organisms of encephalitis are lopapular rash. The three most clini-
the reactivation of a latent herpesvirus cally significant flaviviruses (West Nile
infection (eg, HSV-1 or varicella-zoster virus, St. Louis encephalitis virus, and
virus), a tickborne bacterial infection, or Japanese encephalitis virus) may present
an arthropodborne virus. with a flaccid, weak limb (a poliomyelitis
In the organ transplant recipient, it is syndrome) or parkinsonian features.
critical to obtain the donor history from Confusion and word-finding difficulty
the donor’s file. Cytomegalovirus, West are common in HSV-1 encephalitis.
1020 www.aan.com/continuum October 2011
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
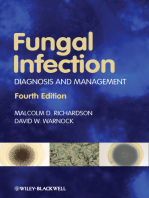
Varicella-zoster virus presents with focal covery (FLAIR) sequences, and diffusion-
neurologic deficits due to ischemic and weighted imaging MR scan within 48
hemorrhagic infarctions. Although vari- hours of symptom onset (Figure 3-1).
cella-zoster virus encephalitis may follow CSF analysis demonstrates a lympho-
shingles, encephalitis due to varicella- cytic pleocytosis with a normal glucose
zoster virus may occur in the absence of concentration. Red blood cells or xan-
a history of shingles. The rash of Rocky thochromia may be seen in the CSF as
Mountain spotted fever typically begins this is hemorrhagic, necrotic encepha-
on the wrists and ankles and then litis. The CSF PCR may be falsely
spreads centrally to the face, chest, and negative in the first 72 hours of HSV
abdomen. This is in contrast to the rash encephalitis symptoms, and detection
of an enterovirus, which begins on the rates decrease 10 days after the onset
face and chest and then spreads to the of symptoms. Serum and CSF HSV IgG
limbs. Borrelia burgdorferi, the causa- antibodies should be obtained to de-
tive spirochete of Lyme disease in North termine whether intrathecal synthesis
America, does not cause encephalitis. of antibodies is present. A serum:CSF
Thus, the appearance of a single erythe- ratio of less than 20:1 is diagnostic of
matous lesion on the trunk or extrem- HSV encephalitis. It takes at least 8
ities is not a clue to the etiologic agent. days for antibodies to be detected in
CSF, and antibodies may be detectable
Diagnosis for up to 3 months. The EEG demon-
Although the specific tests for encepha- strates periodic sharp-and-slow wave
litis are magnetic resonance (MR) scan, complexes occurring at regular 1- to
CSF analysis, blood cultures, and com- 3-second intervals. These abnormalities
plete blood count with differential and are most typically seen between the
serologies, routine tests for encephal- second and fifteenth days of illness.
opathy should be sent as well, including For HSV-1 encephalitis, CSF PCR
serum electrolytes, glucose, creatinine, for HSV-1 and CSF and serum anti-
liver function test, ammonia, and serum bodies should be sent.
and urine toxicology screens. An MR
scan is more sensitive than a CT scan for
encephalitis.
The importance of serologies (acute
phase immunoglobulin M [IgM] and
acute and convalescent immunoglobu-
lin G [IgG] titers) cannot be overstated.
One of the biggest impacts that PCR has
had on the diagnosis of neurologic in-
fectious diseases has been the increased
awareness of other serum and CSF tests
that have been available for years but
were often overlooked because of the
emphasis on neuroimaging abnormali-
ties in diagnosing encephalitis.
Herpes simplex virus type 1. In 90%
of adults with HSV encephalitis, an area FIGURE 3-1 T2-weighted MRI demonstrating
of increased signal intensity is seen a hyperintensity in the left
temporal lobe in a patient with
in the temporal lobe on T2-weighted herpes simplex virus type 1 encephalitis.
images, fluid-attenuated inversion re-
Continuum Lifelong Learning Neurol 2011;17(5):1010–1023 www.aan.com/continuum 1021
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Meningitis and Encephalitis
KEY POINTS
h To diagnose herpes Varicella-zoster virus. The best diag- CSF PCR for cytomegalovirus nucleic
simplex virus type 1 nostic test for varicella-zoster virus en- acid should be sent.
encephalitis, CSF PCR cephalitis is the detection of varicella-
for herpes simplex virus zoster virus IgM in CSF. Therapy
type 1 and CSF and Mosquitoborne viruses. In encepha- HSV-1 encephalitis is treated with
serum antibodies should litis due to any of the flaviviruses, hy- 10 mg/kg of IV acyclovir every 8 hours
be obtained. perintense lesions may be seen in the for 3 weeks. Varicella-zoster virus ence-
h The best diagnostic thalami, substantia nigra, and basal gan- phalitis is treated with 10 mg/kg of IV
test for varicella-zoster glia on T2-weighted and FLAIR sequen- acyclovir every 8 hours for 10 to 14 days.
virus encephalitis ces. The best test for West Nile virus Acyclovir is not recommended for EBV
is the detection of encephalitis is the detection of CSF IgM encephalitis, as it is felt to provide
varicella-zoster virus antibodies specific for the virus. Serum little or no benefit.15 Rocky Mountain
immunoglobulin M IgM and IgG antibodies cannot be used spotted fever is treated with 100 mg of
in CSF. to diagnose neuroinvasive disease. doxycycline twice daily for at least
For the other mosquitoborne viral en- 3 days after the patient becomes afe-
cephalitides, acute and convalescent serol- brile. Cytomegalovirus encephalitis is
ogy remain the mainstay of diagnosis. treated with a combination of 60 mg/kg
Epstein-Barr virus. Diagnosis of of IV foscarnet every 8 hours and 5 mg/kg
Epstein-Barr virus (EBV) depends on a of IV ganciclovir every 12 hours.
combination of serology and CSF PCR.
If serology demonstrates a positive vi- Noninfectious Encephalitis
rus capsid antigen (VCA) and negative Patients with noninfectious encephalitis
Epstein-Barr nuclear antigen (EBNA) and have headache, confusion, behavioral
the CSF PCR for EBV DNA is positive, abnormalities, gait abnormalities, and
a diagnosis of EBV encephalitis can be involuntary movements. CSF analysis
made. If serology demonstrates a neg- demonstrates a lymphocytic pleocytosis
ative VCA IgM and a positive EBNA and with an increased protein concentration
the CSF PCR is positive, a diagnosis of and a normal glucose concentration.
EBV encephalitis cannot be made, as the The hyperintensity in the temporal lobe
CSF PCR may be positive for EBV nucleic on T2-weighted and FLAIR MR images
acid in an immunocompetent individual of paraneoplastic limbic encephalitis has
in any inflammatory CNS disorder. a similar appearance to that of HSV-1
Rocky Mountain spotted fever. The encephalitis. Serology and CSF should
serologic tests for the rickettsial infec- be sent for antineuronal antibodies, and,
tions have a low sensitivity early in the when positive, diagnostic studies should
disease. It is important to biopsy any skin be performed for the malignancy asso-
lesions that are present and to repeatedly ciated with the antineuronal antibody.
send serology. A number of different Nonvasculitic autoimmune inflam-
serologic tests are available, including the matory meningoencephalitis (NAIM)
indirect fluorescent antibody test, ELISA, steroid-responsive encephalopathy
and flow immunoassays. (previously referred to as Hashimoto
Progressive multifocal leukoence- encephalopathy) has been associated
phalopathy. The CSF should be non- with a number of antibodies, including
inflammatory. To diagnose progressive thyroperoxidase antibodies, thyroid
multifocal leukoencephalopathy, CSF microsomal antibodies, thyroglobulin
PCR should be sent for JC virus DNA; antibodies, extractable nuclear anti-
sensitivity may only be around 60%. gen antibodies, antistriatal antibodies,
Cytomegalovirus encephalitis. To antinuclear antibodies, antiphospholi-
diagnose cytomegalovirus encephalitis, pid antibodies, and gliadin antibodies.
1022 www.aan.com/continuum October 2011
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NAIM is treated with 1000 mg of IV adjunctive dexamethasone therapy for
pneumococcal meningitis. Neurology
methylprednisolone for 5 days followed 2010;75(17):1533Y1539.
by oral prednisone therapy.
8. Brouwer MC, McIntyre P, de Gans J,
et al. Corticosteroids for acute bacterial
REFERENCES meningitis. Cochrane Database Syst Rev
2010;8(9):CD004405.
1. Gardner P. Clinical practice. Prevention of
meningococcal disease. N Engl J Med 9. Thwaites GE, Nguyen DB, Nguyen HD, et al.
2006;355(14):1466Y1473. Dexamethasone for the treatment of
tuberculous meningitis in adolescents
2. Radetsky M. Duration of symptoms and
and adults. N Engl J Med 2004;351(17):
outcome in bacterial meningitis: an analysis
1741Y1751.
of causation and the implications of a delay
in diagnosis. Pediatr Infect Dis J 1992;11(9): 10. Kastenbauer S, Pfister HW. Pneumococcal
694Y698. meningitis in adults: spectrum of complications
and prognostic factors in a series of 87 cases.
3. Winkler F, Kastenbauer S, Yousry TA, et al.
Brain 2003;126(pt 5):1015Y1025.
Discrepancies between brain CT imaging
and severely raised intracranial pressure 11. de Jonge RC, van Furth AM, Wassenaar M,
proven by ventriculostomy in adults with et al. Predicting sequelae and death after
pneumococcal meningitis. J Neurol 2002; bacterial meningitis in childhood: a
249(9):1292Y1297. systematic review of prognostic studies.
BMC Infect Dis 2010;10:232.
4. Greenlee JE, Carroll KC. Cerebrospinal fluid
in central nervous system infections. In: 12. Aguilar J, Urday-Cornejo V, Donabedian S,
Scheld WM, Whitley RJ, Marra CM, eds. et al. Staphylococcus aureus meningitis: case
Infections of the central nervous system. series and literature review. Medicine
3rd edition. Philadelphia: Lippincott (Baltimore) 2010;89(2):117Y125.
Williams & Wilkins, 2004:5Y30.
13. Anderson NE, Somaratne J, Mason DF,
5. Desmond RA, Accortt NA, Talley L, et al. et al. A review of tuberculous meningitis
Enteroviral meningitis: natural history and at Auckland City Hospital, New Zealand.
outcome of pleconaril therapy. Antimicrob J Clin Neurosci 2010;17(8):1018Y1022.
Agents Chemother 2006;50(7):2409Y2414.
14. Tunkel Ar, Glaser CA, Bloch KC, et al.
6. Odio CM, Faingezicht I, Paris M, et al. The The management of encephalitis: clinical
beneficial effects of early dexamethasone practice guidelines by the Infectious Diseases
administration in infants and children with Society of America. Clin Infect Dis 2008;
bacterial meningitis. N Engl J Med 1991; 47(3):303Y327.
325(23):1525Y1531.
15. Sejvar JJ. The evolving epidemiology of viral
7. Brouwer MC, Heckenberg SG, de Gans J, encephalitis. Curr Opin Neurol 2006;19(4):
et al. Nationwide implementation of 350Y357.
Continuum Lifelong Learning Neurol 2011;17(5):1010–1023 www.aan.com/continuum 1023
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Anda mungkin juga menyukai
- Medication, Toxic, and Vitamin-Related NeuropathiesDokumen22 halamanMedication, Toxic, and Vitamin-Related Neuropathiessatyagraha84Belum ada peringkat
- Urogenital Symptoms in Neurologic Patients.14Dokumen20 halamanUrogenital Symptoms in Neurologic Patients.14Fawad JanBelum ada peringkat
- GNRH Agonist in Fertility PracticesDokumen31 halamanGNRH Agonist in Fertility Practiceswidya AudistiBelum ada peringkat
- SepsisDokumen16 halamanSepsisDaniela100% (1)
- Critical Appraisal RCTDokumen7 halamanCritical Appraisal RCTAisya FikritamaBelum ada peringkat
- Approach To The Child With Anemia - UpToDateDokumen41 halamanApproach To The Child With Anemia - UpToDateDaniel Enrique CardenasBelum ada peringkat
- FIQ - Focal and Diffuse Choroidal and Retinal InflammationDokumen34 halamanFIQ - Focal and Diffuse Choroidal and Retinal InflammationHikban FiqhiBelum ada peringkat
- PCOS Guidelines 1Dokumen14 halamanPCOS Guidelines 1Angelie Therese ChuaBelum ada peringkat
- Ulkus DekubitusDokumen34 halamanUlkus DekubitusKim LeenBelum ada peringkat
- Jurnal UrolithiasisDokumen6 halamanJurnal UrolithiasisAliimah KhairiyahBelum ada peringkat
- Managing Tuberculosis in PregnancyDokumen1 halamanManaging Tuberculosis in PregnancyAndi Tenri Ola Oddang IIBelum ada peringkat
- Antikoagulan JurnalDokumen5 halamanAntikoagulan JurnalansyemomoleBelum ada peringkat
- Ejhg 2014145Dokumen6 halamanEjhg 2014145Frank Harry LampardBelum ada peringkat
- Papilledema: Epidemiology, Etiology, and Clinical ManagementDokumen11 halamanPapilledema: Epidemiology, Etiology, and Clinical ManagementAita Utsukushi HyuugaBelum ada peringkat
- Sumber CPDokumen9 halamanSumber CPArie RezaBelum ada peringkat
- Congenital Adrenal HyperplasiaDokumen2 halamanCongenital Adrenal HyperplasiaesyBelum ada peringkat
- Endometriosis Boletin PracticoDokumen14 halamanEndometriosis Boletin PracticoNoreenPalenciaBelum ada peringkat
- Polydactyly - A Review IjirrDokumen4 halamanPolydactyly - A Review IjirrDewi AlfiyaniBelum ada peringkat
- PEROTONITISDokumen68 halamanPEROTONITISChloie Marie RosalejosBelum ada peringkat
- Sepsis Sirs Sofa 2018Dokumen18 halamanSepsis Sirs Sofa 2018graciasBelum ada peringkat
- Modul 1 2&3 Pendekatan Berpusat Pada Pasien PDFDokumen29 halamanModul 1 2&3 Pendekatan Berpusat Pada Pasien PDFHadi YantoBelum ada peringkat
- Mind MapDokumen3 halamanMind MapaziemBelum ada peringkat
- Understanding Cerebral PalsyDokumen22 halamanUnderstanding Cerebral PalsyJay SorianoBelum ada peringkat
- Arthritis, Suppurative Arthritis) : Pyogenic Arthritis (Septic Arthritis, InfectiveDokumen4 halamanArthritis, Suppurative Arthritis) : Pyogenic Arthritis (Septic Arthritis, InfectiveRajveerBelum ada peringkat
- EMedicine - Oral Hemangiomas - Article by Steven Brett SloanDokumen19 halamanEMedicine - Oral Hemangiomas - Article by Steven Brett SloanDr Monal YuwanatiBelum ada peringkat
- AnaphylaxisDokumen37 halamanAnaphylaxisDenis Qosja100% (1)
- Neurofibromatosis 1Dokumen10 halamanNeurofibromatosis 1Minelle Sanchez InsoBelum ada peringkat
- HYPER IgE SYNDROME POST ORIF PLATE AND SCREW REMOVALDokumen2 halamanHYPER IgE SYNDROME POST ORIF PLATE AND SCREW REMOVALRiko JumattullahBelum ada peringkat
- Central Nervous System Infections Complicating Immunosuppression and TransplantationDokumen27 halamanCentral Nervous System Infections Complicating Immunosuppression and Transplantationnight.shadowBelum ada peringkat
- Kuliah Periodic Paralysis Akibat TirotoksikosisDokumen14 halamanKuliah Periodic Paralysis Akibat TirotoksikosisFarnida JamhalBelum ada peringkat
- Olanzapine Vs AripiprazoleDokumen8 halamanOlanzapine Vs AripiprazoleDivaviyaBelum ada peringkat
- Hamed2016Dokumen4 halamanHamed2016Franknanda D'enzieroX-zhirawaxaveriuz PutrascreamoDark-nataseBelum ada peringkat
- Facts About Angelman SyndromeDokumen33 halamanFacts About Angelman Syndromederylove100% (1)
- Kasabach Merritt SyndromeDokumen33 halamanKasabach Merritt SyndromeAndrew Arnold David VillanuevaBelum ada peringkat
- Human Papilloma Virus: Incubation PeriodDokumen4 halamanHuman Papilloma Virus: Incubation PeriodArabelle GOBelum ada peringkat
- Extrapiramidal Symptom Rating Scale PDFDokumen11 halamanExtrapiramidal Symptom Rating Scale PDFsisca satyaBelum ada peringkat
- Septic Abortion PDFDokumen4 halamanSeptic Abortion PDFmariachrismayaniBelum ada peringkat
- AUB Current Update (Malam Keakraban PAOGI)Dokumen36 halamanAUB Current Update (Malam Keakraban PAOGI)armillaraissyaBelum ada peringkat
- 2008 - Neurofibromatoses - KaufmnanDokumen203 halaman2008 - Neurofibromatoses - KaufmnanPablo Antonio Antonio100% (1)
- Reaksi AnafilaksisDokumen29 halamanReaksi AnafilaksisoliviafabitaBelum ada peringkat
- Pathfast PresepsinDokumen6 halamanPathfast PresepsinWulan Ervinna SimanjuntakBelum ada peringkat
- NN Jaundice - MoteeDokumen70 halamanNN Jaundice - MoteeMhmBelum ada peringkat
- Pseudomonad GroupDokumen18 halamanPseudomonad GroupNikita MarieBelum ada peringkat
- Recent Update in The Management of Invasive Fungal InfectionDokumen30 halamanRecent Update in The Management of Invasive Fungal Infectionanoop61100% (2)
- Antiepileptic Drugs Continuum 2016Dokumen25 halamanAntiepileptic Drugs Continuum 2016Habib G. Moutran BarrosoBelum ada peringkat
- Diksha SepsisDokumen67 halamanDiksha SepsisDiksha SinghBelum ada peringkat
- APSDokumen18 halamanAPSNadya NovianiBelum ada peringkat
- Keratitis PPT 1 SUB ENGLISHDokumen33 halamanKeratitis PPT 1 SUB ENGLISHarif rhBelum ada peringkat
- VOD - SOS in HSCTDokumen25 halamanVOD - SOS in HSCTKim-Thinh Nguyen ThiBelum ada peringkat
- Evidence-Based Management Of: EpilepsyDokumen240 halamanEvidence-Based Management Of: Epilepsykhalid balshaBelum ada peringkat
- (Aipki) Soal To Regio III Batch 1 2018Dokumen66 halaman(Aipki) Soal To Regio III Batch 1 2018Ali Arridha MolahellaBelum ada peringkat
- Karakteristik Gangguan Tidur Pada Penyakit Parkinson Berdasarkan Parkinson Disease SleepDokumen8 halamanKarakteristik Gangguan Tidur Pada Penyakit Parkinson Berdasarkan Parkinson Disease SleepAfifa NingrumBelum ada peringkat
- Referat - JiaDokumen38 halamanReferat - Jiaira danasasmitaBelum ada peringkat
- Febrile Convulsion & EpilepsyDokumen17 halamanFebrile Convulsion & EpilepsyprajwalBelum ada peringkat
- KDIGO Guideline for Diagnosis and Treatment of CKD-MBDDokumen65 halamanKDIGO Guideline for Diagnosis and Treatment of CKD-MBDCitra DessyBelum ada peringkat
- Komplikasi Stroke PDFDokumen7 halamanKomplikasi Stroke PDFJose Hady PuteraBelum ada peringkat
- MYELITISDokumen8 halamanMYELITISFebrina RamadhaniBelum ada peringkat
- Congenital Tuberculosis A Review ArticleDokumen5 halamanCongenital Tuberculosis A Review ArticleMasita RochsalehaBelum ada peringkat
- Modul Wound Bed Preparation DR Ardianto SucintaDokumen37 halamanModul Wound Bed Preparation DR Ardianto SucintaArdianto SucintaBelum ada peringkat
- Workshop3 PDFDokumen3 halamanWorkshop3 PDFNadila Nur PratiwiBelum ada peringkat
- Treating Acute Angle Closure GlaucomaDokumen3 halamanTreating Acute Angle Closure GlaucomaNadila Nur PratiwiBelum ada peringkat
- Preparing Timetable For IITJEEDokumen4 halamanPreparing Timetable For IITJEEsujsamBelum ada peringkat
- Pediatricreferencecard 04Dokumen2 halamanPediatricreferencecard 04yesumovsBelum ada peringkat
- Budget Planner For EsakalDokumen7 halamanBudget Planner For Esakalapi-19417993Belum ada peringkat
- Adaptor Retea, HH-CM01, OmronDokumen8 halamanAdaptor Retea, HH-CM01, OmronpaspargiliusBelum ada peringkat
- 10 1016@j Psep 2020 05 034Dokumen82 halaman10 1016@j Psep 2020 05 034Kevin SalvatierraBelum ada peringkat
- Rynes Gerhart ParksDokumen33 halamanRynes Gerhart ParksRichard YeongBelum ada peringkat
- Electric Vehicle Safety SheetDokumen2 halamanElectric Vehicle Safety SheetRob NikolewskiBelum ada peringkat
- Free Movie Star Chef Recipes!Dokumen7 halamanFree Movie Star Chef Recipes!jonathanBelum ada peringkat
- Martines Krista Sum2015Dokumen26 halamanMartines Krista Sum2015Ariel Carl Angelo BalletaBelum ada peringkat
- Autoclaved Aerated Concrete BricksDokumen24 halamanAutoclaved Aerated Concrete BricksRazil RomBelum ada peringkat
- BandhaDokumen3 halamanBandhaMouli ChandraBelum ada peringkat
- Syedna's Zulm On SH Sajjad Husein SarangpuriDokumen44 halamanSyedna's Zulm On SH Sajjad Husein SarangpuriMuddasar Ali ZariBelum ada peringkat
- Blockchain SystemDokumen12 halamanBlockchain Systemkhairina100% (1)
- (Ebook) - Piers Anthony - GhostDokumen116 halaman(Ebook) - Piers Anthony - GhostChandresh KothariBelum ada peringkat
- Ensto Voltage Controller: Answer For Today S Power Quality ProblemsDokumen6 halamanEnsto Voltage Controller: Answer For Today S Power Quality ProblemsTBS Máy Phát ĐiệnBelum ada peringkat
- An Overview of The Rabbit Industry in The PhilippinesDokumen3 halamanAn Overview of The Rabbit Industry in The Philippinesallan variasBelum ada peringkat
- Chapter 7 - Muscuar SystemDokumen17 halamanChapter 7 - Muscuar SystemM GarciaBelum ada peringkat
- QUES3Dokumen10 halamanQUES3Múrtåzâ LãxmīdhârBelum ada peringkat
- System No. W-L-2199 Firestop SystemDokumen2 halamanSystem No. W-L-2199 Firestop SystemDatBelum ada peringkat
- Pulkit PPT Steam Turbine3Dokumen42 halamanPulkit PPT Steam Turbine3Abhishek KumarBelum ada peringkat
- Homoeo News - October 09Dokumen2 halamanHomoeo News - October 09noidahomoeopathyBelum ada peringkat
- Atividades 1Dokumen3 halamanAtividades 1Ana Paula DaniloBelum ada peringkat
- Middle Course of River PowerpointDokumen5 halamanMiddle Course of River Powerpointapi-26597187Belum ada peringkat
- Female Genital Mutilation (FGM)Dokumen7 halamanFemale Genital Mutilation (FGM)Karishma RajputBelum ada peringkat
- Occurrence and Use of Hallucinogenic MusDokumen125 halamanOccurrence and Use of Hallucinogenic MusKevin Huamán AvilésBelum ada peringkat
- Iaslc 8th Posters 24x36 2018 Final Version 1Dokumen1 halamanIaslc 8th Posters 24x36 2018 Final Version 1Faskanita NadapdapBelum ada peringkat
- Manfaat Yang Didapatkan Mahasiswa Dalam Mengikuti: Interprofessional Education (Ipe) Dengan Pendekatan Case StudyDokumen5 halamanManfaat Yang Didapatkan Mahasiswa Dalam Mengikuti: Interprofessional Education (Ipe) Dengan Pendekatan Case StudyganditBelum ada peringkat
- MBT Appliance: Mclaughlin Bennett TrevisiDokumen247 halamanMBT Appliance: Mclaughlin Bennett TrevisiJustFine DolittleBelum ada peringkat
- Nielsen Shopper Insights - Retailers Segment - Client 051115 PDFDokumen63 halamanNielsen Shopper Insights - Retailers Segment - Client 051115 PDFn0isyb0yBelum ada peringkat
- Daftar Nama DistributorDokumen12 halamanDaftar Nama DistributorAny Moneta SariBelum ada peringkat
- FORESTRY-WPS OfficeDokumen6 halamanFORESTRY-WPS OfficeJoshua Arboleda de VeraBelum ada peringkat
- Hardiness and Career Adaptability of StudentsDokumen214 halamanHardiness and Career Adaptability of Studentseva pandanaBelum ada peringkat