Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Pulmonary Manifestations of Pediatric DiseasesDokumen356 halamanPulmonary Manifestations of Pediatric Diseasesmihaela_bondocBelum ada peringkat
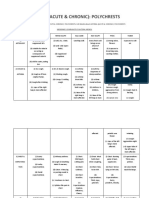
- Asthma (Acute & Chronic) : PolychrestsDokumen14 halamanAsthma (Acute & Chronic) : Polychrestss.s.r.k.m. guptaBelum ada peringkat
- Chest TraumaDokumen122 halamanChest TraumaMarina Maleș100% (1)
- Med Surg Respiratory SystemDokumen173 halamanMed Surg Respiratory Systembamfalcon100% (4)
- Plabable-Gems-31. Respiratory Plabable GemsDokumen68 halamanPlabable-Gems-31. Respiratory Plabable GemsHabo Habo100% (1)
- Pulmonary Function TestsDokumen9 halamanPulmonary Function TestsRick Frea0% (1)
- PB980 Brochure PDFDokumen12 halamanPB980 Brochure PDFTony Nava100% (1)
- Respiratory Quiz QuestionsDokumen5 halamanRespiratory Quiz Questionssv12b100% (2)
- Nursing Care Plan Chronic Obstructive Pulmonary Disease (COPD)Dokumen2 halamanNursing Care Plan Chronic Obstructive Pulmonary Disease (COPD)deric95% (41)
- An Assignment ON: Bronchial HygieneDokumen12 halamanAn Assignment ON: Bronchial Hygienesoniya joseph100% (1)
- Testing Children For Allergies Why, How, Who and When - Eigenmann - 2013 - Pediatric Allergy and Immunology - Wiley Online LibrDokumen1 halamanTesting Children For Allergies Why, How, Who and When - Eigenmann - 2013 - Pediatric Allergy and Immunology - Wiley Online LibrImanuel Far-FarBelum ada peringkat
- Asymptomatic Bacteriuria in PregnancyDokumen5 halamanAsymptomatic Bacteriuria in PregnancyImanuel Far-FarBelum ada peringkat
- Prevention and Treatment of Bacterial Meningitis.21Dokumen3 halamanPrevention and Treatment of Bacterial Meningitis.21Imanuel Far-FarBelum ada peringkat
- Epidemiologi Allergy PDFDokumen12 halamanEpidemiologi Allergy PDFImanuel Far-FarBelum ada peringkat
- Nitrit OptimizingDokumen6 halamanNitrit OptimizingImanuel Far-FarBelum ada peringkat
- Shortness of BreathDokumen4 halamanShortness of BreathImanuel Far-FarBelum ada peringkat
- Sob Ef M PDFDokumen3 halamanSob Ef M PDFraissaBelum ada peringkat
- Familial Forms of NS PDFDokumen12 halamanFamilial Forms of NS PDFImanuel Far-FarBelum ada peringkat
- Familial NSDokumen10 halamanFamilial NSImanuel Far-FarBelum ada peringkat
- Hypothyroid PIR 2009Dokumen10 halamanHypothyroid PIR 2009Imanuel Far-FarBelum ada peringkat
- Vaksinasi Pada Pasien ImmunosupresiDokumen12 halamanVaksinasi Pada Pasien ImmunosupresiImanuel Far-FarBelum ada peringkat
- Tolerance of Partially Hydrolyzed Whey Formula in Cow's Milk Allergic PatientsDokumen1 halamanTolerance of Partially Hydrolyzed Whey Formula in Cow's Milk Allergic PatientsImanuel Far-FarBelum ada peringkat
- Weaning to a Partially Hydrolyzed Whey Formula at Three Months of Age Protects Against the Later Development of Anti-Cow Milk IgE Antibodies in Comparison to Whole Cow's Milk or Extensively Hydrolyzed Whey FormulaDokumen1 halamanWeaning to a Partially Hydrolyzed Whey Formula at Three Months of Age Protects Against the Later Development of Anti-Cow Milk IgE Antibodies in Comparison to Whole Cow's Milk or Extensively Hydrolyzed Whey FormulaImanuel Far-FarBelum ada peringkat
- Comparison of Cervical Cancer Screening Strategies Incorporating Different CombinatioonDokumen11 halamanComparison of Cervical Cancer Screening Strategies Incorporating Different CombinatioonImanuel Far-FarBelum ada peringkat
- Fever in Children With ChemoteraphyDokumen23 halamanFever in Children With ChemoteraphyImanuel Far-FarBelum ada peringkat
- Economic Evaluation of A 100% Whey-BasedDokumen15 halamanEconomic Evaluation of A 100% Whey-BasedImanuel Far-FarBelum ada peringkat
- Cow Milk AllergyDokumen8 halamanCow Milk AllergyImanuel Far-FarBelum ada peringkat
- Cost-Effectiveness of Partially Hydrolyzed Whey Protein in FilipinoDokumen12 halamanCost-Effectiveness of Partially Hydrolyzed Whey Protein in FilipinoImanuel Far-FarBelum ada peringkat
- Familial Forms of NSDokumen12 halamanFamilial Forms of NSImanuel Far-FarBelum ada peringkat
- Cohort Study ContraceptionDokumen10 halamanCohort Study ContraceptionCitra KristiBelum ada peringkat
- Dengue Infection in PregnancyDokumen8 halamanDengue Infection in PregnancyImanuel Far-FarBelum ada peringkat
- HEMOPHILIA GuidelinesDokumen76 halamanHEMOPHILIA Guidelinesmarco_jacinto1103197Belum ada peringkat
- Dhar, 2016 Food Allergy in Atopic DermatitisDokumen6 halamanDhar, 2016 Food Allergy in Atopic DermatitisImanuel Far-FarBelum ada peringkat
- CHATTERTON, Anti-Inflammatory Mechanisms of Bioactive Milk Proteins in TheDokumen18 halamanCHATTERTON, Anti-Inflammatory Mechanisms of Bioactive Milk Proteins in TheImanuel Far-FarBelum ada peringkat
- Behaviour Change Techniques and Contraceptive Use in Low and Middle Income CountryDokumen8 halamanBehaviour Change Techniques and Contraceptive Use in Low and Middle Income CountryImanuel Far-FarBelum ada peringkat
- CHEN, Analysis of A-Lactalbumin-, B-Lactoglobulin-, andDokumen7 halamanCHEN, Analysis of A-Lactalbumin-, B-Lactoglobulin-, andImanuel Far-FarBelum ada peringkat
- CUCU, Effect of Partial Hydrolysis On The Hazelnut and Soybean Protein Detectability PDFDokumen7 halamanCUCU, Effect of Partial Hydrolysis On The Hazelnut and Soybean Protein Detectability PDFImanuel Far-FarBelum ada peringkat
- CASTRO-JUNIOR, Oral Tolerance Correlates With High Levels of Lymphocyte ActivityDokumen11 halamanCASTRO-JUNIOR, Oral Tolerance Correlates With High Levels of Lymphocyte ActivityImanuel Far-FarBelum ada peringkat
- CANANI, Formula Selection For Management of Children With Cow's MilkDokumen8 halamanCANANI, Formula Selection For Management of Children With Cow's MilkImanuel Far-FarBelum ada peringkat
- Impaired Gas Exchange NCPDokumen3 halamanImpaired Gas Exchange NCPRomel BaliliBelum ada peringkat
- Bronchitis 2nd YrDokumen14 halamanBronchitis 2nd YrridijaBelum ada peringkat
- GKNM Hospital ReportDokumen33 halamanGKNM Hospital ReportKarthi KeyanBelum ada peringkat
- Bts Guideline For Oxygen Use in Adults in Healthcare and Emergency SettingsDokumen100 halamanBts Guideline For Oxygen Use in Adults in Healthcare and Emergency SettingsalbarkatBelum ada peringkat
- 07.03.53 Mechanical VentilationDokumen3 halaman07.03.53 Mechanical VentilationSapna thakurBelum ada peringkat
- Short Diagnosis Report: PatientDokumen6 halamanShort Diagnosis Report: PatientCarmen JurcoaneBelum ada peringkat
- Sced 3204B LDokumen3 halamanSced 3204B LEllen Grace Dela PeñaBelum ada peringkat
- Test Bank For Mechanical Ventilation 2nd Edition Macintyre Isbn 10 1416031413 Isbn 13 9781416031413Dokumen14 halamanTest Bank For Mechanical Ventilation 2nd Edition Macintyre Isbn 10 1416031413 Isbn 13 9781416031413calliopesilasaagyBelum ada peringkat
- Resmed - Philips Script Convert.Dokumen28 halamanResmed - Philips Script Convert.Diabestes-stuff100% (1)
- Airway Clearance TechniquesDokumen14 halamanAirway Clearance TechniquesKhushboo DurejaBelum ada peringkat
- Ineffective Airway ClearanceDokumen9 halamanIneffective Airway ClearanceMarissa AsimBelum ada peringkat
- Hospital Paneld 18 November 20191 PDFDokumen88 halamanHospital Paneld 18 November 20191 PDFHarish prajapatBelum ada peringkat
- Cheat Sheets For Ventilation 5Dokumen19 halamanCheat Sheets For Ventilation 5Syed Shahrul Naz Syed100% (1)
- Nursing Care Plan Impaired Gas ExchangeDokumen1 halamanNursing Care Plan Impaired Gas ExchangeKarylle PetilBelum ada peringkat
- Chest Physiotherapy or Techniques in Cardio Pulmonary Physiotherapy A Running CommentaryDokumen5 halamanChest Physiotherapy or Techniques in Cardio Pulmonary Physiotherapy A Running CommentaryGopi KrishnanBelum ada peringkat
- Joi170110supp3 ProdDokumen37 halamanJoi170110supp3 ProdsprfyllisBelum ada peringkat
- L17. Askep Kritis Dan Gadar Pasien Dengan Ggguan Sistem Pernafan NontraumatikDokumen75 halamanL17. Askep Kritis Dan Gadar Pasien Dengan Ggguan Sistem Pernafan NontraumatikSepto KristianaBelum ada peringkat
- Module 12 - Health Conditions RajDokumen6 halamanModule 12 - Health Conditions RajRajesh MakwanaBelum ada peringkat
- Flyer PICNIC ACADEMIA REGULAR COURSE NICU (LUNGS)Dokumen1 halamanFlyer PICNIC ACADEMIA REGULAR COURSE NICU (LUNGS)frbriyanty cendyBelum ada peringkat