Anda mungkin juga menyukai
- FDG PET CT in Testicular CancerDokumen4 halamanFDG PET CT in Testicular CancerlkitkatgirlBelum ada peringkat
- Askin's TumorDokumen5 halamanAskin's Tumoranon_828221297Belum ada peringkat
- Nasopharyngeal Carcinoma in Children and AdolescentsDokumen5 halamanNasopharyngeal Carcinoma in Children and AdolescentsSyifa MunawarahBelum ada peringkat
- Local Control in Metastatic Neuroblastoma in Children Over 1 Year of AgeDokumen8 halamanLocal Control in Metastatic Neuroblastoma in Children Over 1 Year of AgePutri ManurungBelum ada peringkat
- Bindea Et Al. - 2011 - The Prognostic Impact of Anti-Cancer Immune Response A Novel Classification of Cancer Patients PDFDokumen6 halamanBindea Et Al. - 2011 - The Prognostic Impact of Anti-Cancer Immune Response A Novel Classification of Cancer Patients PDFflashjetBelum ada peringkat
- cancer de hipofaringeDokumen8 halamancancer de hipofaringeBrandaBelum ada peringkat
- Radioterapia en CacUDokumen6 halamanRadioterapia en CacUVicente RamosBelum ada peringkat
- Tumores Malignos de Anexos CutáneosDokumen7 halamanTumores Malignos de Anexos CutáneostisadermaBelum ada peringkat
- Piis0167814019331123 230304 134522Dokumen7 halamanPiis0167814019331123 230304 134522Samuel Kelvin RuslimBelum ada peringkat
- The Impact of PETCT On Paediatric OncologyDokumen17 halamanThe Impact of PETCT On Paediatric OncologylkitkatgirlBelum ada peringkat
- Autologous: Journal HomepageDokumen9 halamanAutologous: Journal HomepageSiddharth DhanarajBelum ada peringkat
- Agaoglu2005 2Dokumen6 halamanAgaoglu2005 2Ngo Quang MinhBelum ada peringkat
- Vandenbent 2021Dokumen11 halamanVandenbent 2021bugBelum ada peringkat
- F-FDG PET CT As A Prognostic Factor in Hepatocellular CarcinomaDokumen7 halamanF-FDG PET CT As A Prognostic Factor in Hepatocellular CarcinomaUvi Cancino RamosBelum ada peringkat
- Pretreatment Leukocytes Predict Outcomes in HPV+ Oropharyngeal CancerDokumen11 halamanPretreatment Leukocytes Predict Outcomes in HPV+ Oropharyngeal CancerJoana KellenBelum ada peringkat
- Completion Thyroidectomy: Predicting Bilateral Disease: Originalresearcharticle Open AccessDokumen7 halamanCompletion Thyroidectomy: Predicting Bilateral Disease: Originalresearcharticle Open AccessRadita Dwihaning PutriBelum ada peringkat
- How To Approach Phyllodes Tumors of The Breast?Dokumen5 halamanHow To Approach Phyllodes Tumors of The Breast?lPiNGUSlBelum ada peringkat
- s11060 004 3546 5Dokumen5 halamans11060 004 3546 5Neetu ChadhaBelum ada peringkat
- Kjco 14 2 83Dokumen6 halamanKjco 14 2 83Antonio GligorievskiBelum ada peringkat
- Biomedicines 11 00128Dokumen13 halamanBiomedicines 11 00128dmandatari7327Belum ada peringkat
- 11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayDokumen8 halaman11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayBridia BogarBelum ada peringkat
- AsianJNeurosurg10150-2524489 070044 PDFDokumen4 halamanAsianJNeurosurg10150-2524489 070044 PDFSucipto HartonoBelum ada peringkat
- Jurnal Radiologi 2Dokumen21 halamanJurnal Radiologi 2Adelya Dwi AsyifaBelum ada peringkat
- Original ArticleDokumen6 halamanOriginal ArticleGaluin KulaimBelum ada peringkat
- Switch To EGFR TKI After Upfront Platinum Doublet Inductio - 2022 - Cancer TreatDokumen6 halamanSwitch To EGFR TKI After Upfront Platinum Doublet Inductio - 2022 - Cancer Treatyuris hikmanBelum ada peringkat
- Dok Til 1Dokumen15 halamanDok Til 1Nurul Ulya RahimBelum ada peringkat
- Rcsann 2016 0300Dokumen4 halamanRcsann 2016 0300Siti Ayu kamsiahBelum ada peringkat
- Prognostic Value of Metabolic Tumor Burden On F-FDG PET in Nonsurgical Patients With Non-Small Cell Lung CancerDokumen12 halamanPrognostic Value of Metabolic Tumor Burden On F-FDG PET in Nonsurgical Patients With Non-Small Cell Lung CancerAmina GoharyBelum ada peringkat
- Diffuse Malignant Peritoneal Mesothelioma PDFDokumen9 halamanDiffuse Malignant Peritoneal Mesothelioma PDFAndreeaPopescuBelum ada peringkat
- 2019 Article 5894 PDFDokumen8 halaman2019 Article 5894 PDFGalgalo GarbichaBelum ada peringkat
- jnm046045 1920.Dokumen3 halamanjnm046045 1920.Rahul KashyapBelum ada peringkat
- As Trocito MaDokumen10 halamanAs Trocito Majeimy_carolina4163Belum ada peringkat
- Myositis Abstract v5-TMDokumen5 halamanMyositis Abstract v5-TMcaptainessliliBelum ada peringkat
- Identification of Patients at Risk of Metastasis UDokumen13 halamanIdentification of Patients at Risk of Metastasis UYilianeth Mena DazaBelum ada peringkat
- CBM Final PDFDokumen7 halamanCBM Final PDFSamah Abd ElhamidBelum ada peringkat
- Nejmoa 1112088Dokumen11 halamanNejmoa 1112088Med MedBelum ada peringkat
- Chu J, 2018Dokumen8 halamanChu J, 2018Andrea QuillupanguiBelum ada peringkat
- Cancers 12 00611Dokumen17 halamanCancers 12 00611IRINA BRANBelum ada peringkat
- 10 1002@pbc 27697Dokumen8 halaman10 1002@pbc 27697Ravi JhaBelum ada peringkat
- 1 s2.0 S0021755722000055 MainDokumen6 halaman1 s2.0 S0021755722000055 MainUsee TvBelum ada peringkat
- Cancers 14 03161Dokumen10 halamanCancers 14 03161Majd AssaadBelum ada peringkat
- Surgical Treatment of Trichilemmal CarcinomaDokumen4 halamanSurgical Treatment of Trichilemmal CarcinomaNESRINE MARZAKBelum ada peringkat
- Metastatic Hepatocellular Carcinoma Diagnosed by Fine Needle Aspiration: A Clinical and Cytologic StudyDokumen6 halamanMetastatic Hepatocellular Carcinoma Diagnosed by Fine Needle Aspiration: A Clinical and Cytologic StudyMara PitrezBelum ada peringkat
- Management of CraniopharyngiomaDokumen36 halamanManagement of CraniopharyngiomaNguyên KhoaBelum ada peringkat
- Glomus TumourDokumen5 halamanGlomus TumourDiamond DustBelum ada peringkat
- Nueroblastoma en AlemaniaDokumen17 halamanNueroblastoma en Alemaniavalentina rojasBelum ada peringkat
- Characterization of Adrenal Metastatic Cancer Using FDG PET CTDokumen8 halamanCharacterization of Adrenal Metastatic Cancer Using FDG PET CTEngky ChristianBelum ada peringkat
- Articles: BackgroundDokumen11 halamanArticles: BackgroundOncología CdsBelum ada peringkat
- Non-Suppressed Thyrotropin and Elevated Thyroglobulin Are Independent Predictors of Recurrence in Differentiated Thyroid CarcinomaDokumen8 halamanNon-Suppressed Thyrotropin and Elevated Thyroglobulin Are Independent Predictors of Recurrence in Differentiated Thyroid CarcinomaPressureserveBelum ada peringkat
- Trends in Patient Outcome Over The Past Two DecadesDokumen12 halamanTrends in Patient Outcome Over The Past Two Decadesfransiskus rendyBelum ada peringkat
- Ann Oncol 2010 Stupp v190 3Dokumen4 halamanAnn Oncol 2010 Stupp v190 3Aryantii AntyBelum ada peringkat
- Head and Neck Surgery: Pressure Ulcer Prevention Strategies in Prolonged SurgeryDokumen2 halamanHead and Neck Surgery: Pressure Ulcer Prevention Strategies in Prolonged SurgeryBenny KurniawanBelum ada peringkat
- ESMO Testicular CancerDokumen8 halamanESMO Testicular CancerBernadetta ViaBelum ada peringkat
- Correlation of MRI, Clinical and Pathologic Tumor Sizes in Cervical CancerDokumen1 halamanCorrelation of MRI, Clinical and Pathologic Tumor Sizes in Cervical CancerRomildo da SilvaBelum ada peringkat
- Carsinoma NasopharyngealDokumen9 halamanCarsinoma NasopharyngealRahma R SBelum ada peringkat
- Emergency Department Based Monoclonal Antibody TheDokumen2 halamanEmergency Department Based Monoclonal Antibody The88fqjgsdk5Belum ada peringkat
- Cancer in Rural MaharashtraDokumen2 halamanCancer in Rural MaharashtravporechaBelum ada peringkat
- Ewing's Sarcoma Review ArticleDokumen9 halamanEwing's Sarcoma Review ArticleSayan DasBelum ada peringkat
- The Use and Efficacy of Chemotherapy and Radiotherapy in Children and Adults With Pilocytic AstrocytomaDokumen9 halamanThe Use and Efficacy of Chemotherapy and Radiotherapy in Children and Adults With Pilocytic AstrocytomaAlejandro Zurita SaáBelum ada peringkat
- Water Colored Splashes PowerPoint TemplateDokumen36 halamanWater Colored Splashes PowerPoint TemplateAna Carmela DomingoBelum ada peringkat
- Kertas Resep YudiDokumen1 halamanKertas Resep YuditopBelum ada peringkat
- Eye TraumaDokumen19 halamanEye TraumatopBelum ada peringkat
- Pediatric Non-Hodgkin Lymphoma Treatment & Management: Approach ConsiderationsDokumen15 halamanPediatric Non-Hodgkin Lymphoma Treatment & Management: Approach ConsiderationstopBelum ada peringkat
- The Open Ophthalmology JournalDokumen5 halamanThe Open Ophthalmology JournalFenny Duma SariBelum ada peringkat
- Pediatric Non-Hodgkin Lymphoma Medication GuideDokumen8 halamanPediatric Non-Hodgkin Lymphoma Medication GuidetopBelum ada peringkat
- Eye ManualDokumen56 halamanEye Manualbashir019Belum ada peringkat
- Abstrack Delibrate PracticeDokumen2 halamanAbstrack Delibrate PracticetopBelum ada peringkat
- Slit LampbiomicrosDokumen18 halamanSlit LampbiomicrostopBelum ada peringkat
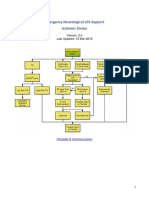
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Dokumen22 halamanEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraBelum ada peringkat
- Pediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiesDokumen5 halamanPediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiestopBelum ada peringkat
- Pediatric Non-Hodgkin Lymphoma - Background, Etiology, EpidemiologyDokumen11 halamanPediatric Non-Hodgkin Lymphoma - Background, Etiology, EpidemiologytopBelum ada peringkat
- Pediatric Non-Hodgkin Lymphoma Clinical Presentation - History, Physical ExaminationDokumen3 halamanPediatric Non-Hodgkin Lymphoma Clinical Presentation - History, Physical ExaminationtopBelum ada peringkat
- Pediatric Non-Hodgkin Lymphoma Differential DiagnosesDokumen2 halamanPediatric Non-Hodgkin Lymphoma Differential DiagnosestopBelum ada peringkat
- Jurnal Asli CSS - Khalida Khairunnisa - DR - ErniDokumen7 halamanJurnal Asli CSS - Khalida Khairunnisa - DR - ErnitopBelum ada peringkat
- Role of Limited Whole-BodyDokumen9 halamanRole of Limited Whole-BodytopBelum ada peringkat
- CSS Jurnal DR IdratDokumen8 halamanCSS Jurnal DR IdrattopBelum ada peringkat
- Radiologic Clinics of North America Volume 46 Issue 2 2008 (Doi 10.1016/j.rcl.2008.03.009) Abramson, Sara J. Price, Anita P. - Imaging of Pediatric LymphomasDokumen26 halamanRadiologic Clinics of North America Volume 46 Issue 2 2008 (Doi 10.1016/j.rcl.2008.03.009) Abramson, Sara J. Price, Anita P. - Imaging of Pediatric LymphomastopBelum ada peringkat
- Presentation 1Dokumen8 halamanPresentation 1topBelum ada peringkat
- Total ModalDokumen1 halamanTotal ModaltopBelum ada peringkat
- Nasal saline irrigation efficacy pediatric rhinosinusitisDokumen19 halamanNasal saline irrigation efficacy pediatric rhinosinusitistopBelum ada peringkat
- Poster Publik & Poster IlmiahDokumen10 halamanPoster Publik & Poster Ilmiahtop100% (1)
- Antihistamines For Treating RhinosinusitisDokumen6 halamanAntihistamines For Treating RhinosinusitistopBelum ada peringkat
- DESIGN? VECTOR VS BITMAPDokumen27 halamanDESIGN? VECTOR VS BITMAPtopBelum ada peringkat
- Guideline AoeDokumen25 halamanGuideline AoetopBelum ada peringkat
- Role of Isotonic Saline Nasal Irrigation in Seasonal Allergic RhinitisDokumen5 halamanRole of Isotonic Saline Nasal Irrigation in Seasonal Allergic RhinitistopBelum ada peringkat
- Felting Fabulous Flowers Templates PDFDokumen3 halamanFelting Fabulous Flowers Templates PDFtop67% (3)
- Antibiotics in Chronic RhinosinusitisDokumen5 halamanAntibiotics in Chronic RhinosinusitistopBelum ada peringkat
- Anatomy and Physiology Nasal ObstructionDokumen13 halamanAnatomy and Physiology Nasal ObstructiontopBelum ada peringkat
- Maths Clinic Gr12 ENG SmartPrep v1.0 1 PDFDokumen69 halamanMaths Clinic Gr12 ENG SmartPrep v1.0 1 PDFNakeisha Jesse Napallatan50% (6)
- JVT D125 LDokumen12 halamanJVT D125 LGrupo SolucionesBelum ada peringkat
- MPXV7007Dokumen11 halamanMPXV7007Phi MacBelum ada peringkat
- Ict Skills IIDokumen28 halamanIct Skills IIShraddha DubeyBelum ada peringkat
- Excel Formulas and Functions 2021-The Intermediate Level Step byDokumen122 halamanExcel Formulas and Functions 2021-The Intermediate Level Step bymaolegu100% (3)
- SAG - VGD NC 3Dokumen8 halamanSAG - VGD NC 3Jek KejBelum ada peringkat
- Hummer Space Adventure Service ManualDokumen73 halamanHummer Space Adventure Service ManualTony KututoBelum ada peringkat
- Apple Technology To Support Learning For Students With Sensory and Learning DisabilitiesDokumen25 halamanApple Technology To Support Learning For Students With Sensory and Learning Disabilitiesssa_joeBelum ada peringkat
- Doc-Fe Ie DT 021054 En-0 1Dokumen7 halamanDoc-Fe Ie DT 021054 En-0 1muhammad jalal khanBelum ada peringkat
- 2021 MSF2021 PM MG Precon3dDokumen4 halaman2021 MSF2021 PM MG Precon3dPavao MarovicBelum ada peringkat
- Supermicro TwinServer 2027PR-HC1R - 8coreDokumen1 halamanSupermicro TwinServer 2027PR-HC1R - 8coreAndreas CimengBelum ada peringkat
- 19Dokumen55 halaman19Daniel MosesBelum ada peringkat
- Assignment 3Dokumen2 halamanAssignment 3Poonam VaswaniBelum ada peringkat
- Diffpairs Cadence App Note 165Dokumen19 halamanDiffpairs Cadence App Note 165Mallappa PatilBelum ada peringkat
- Adxl345 App Note An-1023Dokumen28 halamanAdxl345 App Note An-1023b0bb0bb0bBelum ada peringkat
- Catchlogs - 2023-01-10 at 05-30-40 - 5.12.0.100 (1165) - .JavaDokumen27 halamanCatchlogs - 2023-01-10 at 05-30-40 - 5.12.0.100 (1165) - .Javaarie candraBelum ada peringkat
- Delta Ltl2000sDokumen45 halamanDelta Ltl2000sDritta Anies CahayaBelum ada peringkat
- Electrical Permit Application FormDokumen3 halamanElectrical Permit Application FormChristian RuizBelum ada peringkat
- FALCON: Smart Portable Solution: Condition Monitoring Has Never Been So Easy!!Dokumen21 halamanFALCON: Smart Portable Solution: Condition Monitoring Has Never Been So Easy!!Pedro RosaBelum ada peringkat
- EmanuelDokumen4 halamanEmanuelbawihpuiapaBelum ada peringkat
- XRC BasicDokumen136 halamanXRC BasicJunior FernandesBelum ada peringkat
- FLEXIBOWL V2.0 - Electrical Panel (EN)Dokumen7 halamanFLEXIBOWL V2.0 - Electrical Panel (EN)Adolfo ReverteBelum ada peringkat
- Certificate SampleDokumen2 halamanCertificate SampleAljenneth MicallerBelum ada peringkat
- Conductivity TesterDokumen4 halamanConductivity TesterFelix PintoBelum ada peringkat
- HP10 BLLDokumen13 halamanHP10 BLLkelvin mkweshaBelum ada peringkat
- Qlogic SAN CLI GuideDokumen408 halamanQlogic SAN CLI Guide김대성Belum ada peringkat
- Advance Optima Analyzer 50 24 01EN FinalDokumen12 halamanAdvance Optima Analyzer 50 24 01EN FinalJoeyBelum ada peringkat
- The Brocard - Ramanujan Diophantine Equation N! + 1 M 2Dokumen2 halamanThe Brocard - Ramanujan Diophantine Equation N! + 1 M 2api-26401608Belum ada peringkat
- Fungsi Komposisi English YOLANDADokumen11 halamanFungsi Komposisi English YOLANDAyolanda anastasyaBelum ada peringkat
- Emerging IT trends in management systemsDokumen5 halamanEmerging IT trends in management systemsrohan kumarBelum ada peringkat
- Mastering Parrot Behavior: A Step-by-Step Guide to Building a Strong Relationship with Your Avian FriendDari EverandMastering Parrot Behavior: A Step-by-Step Guide to Building a Strong Relationship with Your Avian FriendPenilaian: 4.5 dari 5 bintang4.5/5 (69)
- Horse Training 101: Key Techniques for Every Horse OwnerDari EverandHorse Training 101: Key Techniques for Every Horse OwnerPenilaian: 4.5 dari 5 bintang4.5/5 (27)
- Show Dog: The Charmed Life and Trying Times of a Near-Perfect PurebredDari EverandShow Dog: The Charmed Life and Trying Times of a Near-Perfect PurebredPenilaian: 3.5 dari 5 bintang3.5/5 (13)
- Inside of a Dog: What Dogs See, Smell, and KnowDari EverandInside of a Dog: What Dogs See, Smell, and KnowPenilaian: 4 dari 5 bintang4/5 (390)
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueDari EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescuePenilaian: 5 dari 5 bintang5/5 (2)
- The Dog Listener: Learn How to Communicate with Your Dog for Willing CooperationDari EverandThe Dog Listener: Learn How to Communicate with Your Dog for Willing CooperationPenilaian: 4 dari 5 bintang4/5 (37)
- Dog Training Journeys: A Guide to Training and Bonding with Your Mix-Breed DogDari EverandDog Training Journeys: A Guide to Training and Bonding with Your Mix-Breed DogPenilaian: 4.5 dari 5 bintang4.5/5 (77)
- Cats Can Learn Too: A Simple Guide to Training Your Furry FriendDari EverandCats Can Learn Too: A Simple Guide to Training Your Furry FriendPenilaian: 4.5 dari 5 bintang4.5/5 (55)
- Will's Red Coat: The Story of One Old Dog Who Chose to Live AgainDari EverandWill's Red Coat: The Story of One Old Dog Who Chose to Live AgainPenilaian: 4.5 dari 5 bintang4.5/5 (18)
- Come Back, Como: Winning the Heart of a Reluctant DogDari EverandCome Back, Como: Winning the Heart of a Reluctant DogPenilaian: 3.5 dari 5 bintang3.5/5 (10)
- An Eagle Named Freedom: My True Story of a Remarkable FriendshipDari EverandAn Eagle Named Freedom: My True Story of a Remarkable FriendshipBelum ada peringkat
- Your Dog Is Your Mirror: The Emotional Capacity of Our Dogs and OurselvesDari EverandYour Dog Is Your Mirror: The Emotional Capacity of Our Dogs and OurselvesPenilaian: 4 dari 5 bintang4/5 (30)
- The Other End of the Leash: Why We Do What We Do Around DogsDari EverandThe Other End of the Leash: Why We Do What We Do Around DogsPenilaian: 5 dari 5 bintang5/5 (63)
- What Cats Want: An Illustrated Guide for Truly Understanding Your CatDari EverandWhat Cats Want: An Illustrated Guide for Truly Understanding Your CatPenilaian: 4.5 dari 5 bintang4.5/5 (13)
- Lessons from Tara: Life Advice from the World's Most Brilliant DogDari EverandLessons from Tara: Life Advice from the World's Most Brilliant DogPenilaian: 4.5 dari 5 bintang4.5/5 (42)
- The Dog Who Couldn't Stop Loving: How Dogs Have Captured Our Hearts for Thousands of YearsDari EverandThe Dog Who Couldn't Stop Loving: How Dogs Have Captured Our Hearts for Thousands of YearsBelum ada peringkat
- Bird Life: A Guide to the Study of Our Common BirdsDari EverandBird Life: A Guide to the Study of Our Common BirdsPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- Stable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnDari EverandStable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnPenilaian: 5 dari 5 bintang5/5 (4)
- The Illustrated Guide to Chickens: How to Choose Them, How to Keep ThemDari EverandThe Illustrated Guide to Chickens: How to Choose Them, How to Keep ThemPenilaian: 4.5 dari 5 bintang4.5/5 (5)
- Edward's Menagerie: Dogs: 50 canine crochet patternsDari EverandEdward's Menagerie: Dogs: 50 canine crochet patternsPenilaian: 3 dari 5 bintang3/5 (5)
- The Purest Bond: Understanding the Human-Canine ConnectionDari EverandThe Purest Bond: Understanding the Human-Canine ConnectionPenilaian: 4 dari 5 bintang4/5 (4)
- Fish School 101: A Step-by-Step Guide for Fish OwnersDari EverandFish School 101: A Step-by-Step Guide for Fish OwnersPenilaian: 5 dari 5 bintang5/5 (16)
- What It Takes to Save a Life: A Veterinarian’s Quest for Healing and HopeDari EverandWhat It Takes to Save a Life: A Veterinarian’s Quest for Healing and HopeBelum ada peringkat
- Meet Your Dog: The Game-Changing Guide to Understanding Your Dog's BehaviorDari EverandMeet Your Dog: The Game-Changing Guide to Understanding Your Dog's BehaviorPenilaian: 5 dari 5 bintang5/5 (34)
- Puppy Training 101: How to Train a Puppy, Training Your Own Psychiatric Service Dog, A Step-By-Step Program so your Pup Will Understand You!Dari EverandPuppy Training 101: How to Train a Puppy, Training Your Own Psychiatric Service Dog, A Step-By-Step Program so your Pup Will Understand You!Penilaian: 5 dari 5 bintang5/5 (85)
- The Wrong Dog: An Unlikely Tale of Unconditional LoveDari EverandThe Wrong Dog: An Unlikely Tale of Unconditional LovePenilaian: 4.5 dari 5 bintang4.5/5 (26)