Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Ecg in Emergency Medicine and Acute Care-2005Dokumen420 halamanEcg in Emergency Medicine and Acute Care-2005Ioana Nicoleta Dinu91% (22)
- IN25 Sensory Overload Induction - PHPDokumen3 halamanIN25 Sensory Overload Induction - PHPlucianmateoBelum ada peringkat
- Lotus Home Care Induction Manual © 2012 Inspire Education April 2012Dokumen20 halamanLotus Home Care Induction Manual © 2012 Inspire Education April 2012Nhung NguyenBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Personal BoundariesDokumen4 halamanPersonal Boundariesscribdreaderplus75% (4)
- (The Norton Library) Karen Horney - Feminine Psychology (1973, W W Norton & Co.)Dokumen276 halaman(The Norton Library) Karen Horney - Feminine Psychology (1973, W W Norton & Co.)daniela86% (7)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- M-FUN Assessment ReviewDokumen4 halamanM-FUN Assessment ReviewKishan RamtohulBelum ada peringkat
- Acog Practice Bulletin Summary: Management of Symptomatic Uterine LeiomyomasDokumen3 halamanAcog Practice Bulletin Summary: Management of Symptomatic Uterine LeiomyomasMariana Hernandez100% (6)
- Peter Pan Syndrome Is A DeepDokumen3 halamanPeter Pan Syndrome Is A DeeptucklertBelum ada peringkat
- What Is Head and Neck CancerDokumen42 halamanWhat Is Head and Neck CancerrositaBelum ada peringkat
- NURSING CARE PLAN OcdDokumen25 halamanNURSING CARE PLAN Ocdkiran mahal81% (26)
- Barium MealDokumen3 halamanBarium MealVithiya Chandra SagaranBelum ada peringkat
- Test Bank For Counseling and Psychotherapy Theories in Context and Practice Skills Strategies and Techniques 3rd Edition John Sommers Flanagan Rita Sommers FlanaganDokumen17 halamanTest Bank For Counseling and Psychotherapy Theories in Context and Practice Skills Strategies and Techniques 3rd Edition John Sommers Flanagan Rita Sommers Flanagancuthbertfinncx2nBelum ada peringkat
- Standard Operating Procedure Handling, Storage and Disposal: Punyam Manufacturing INCDokumen4 halamanStandard Operating Procedure Handling, Storage and Disposal: Punyam Manufacturing INCJaijeev PaliBelum ada peringkat
- Biochemistry LaboratoryDokumen6 halamanBiochemistry LaboratoryMark Benedict MontalboBelum ada peringkat
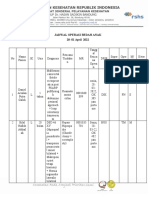
- JOP 28 Mar-01 Apr - WYDokumen6 halamanJOP 28 Mar-01 Apr - WYBell SwanBelum ada peringkat
- E PosterDokumen2 halamanE PosterBell SwanBelum ada peringkat
- Colonic StenosisDokumen3 halamanColonic StenosisBell SwanBelum ada peringkat
- CAT Jurnal ReadingDokumen9 halamanCAT Jurnal ReadingBell SwanBelum ada peringkat
- Medicine: Full-Endoscopic Discectomy Via The Interlaminar Approach For Disc Herniation at L4-L5 and L5-S1Dokumen7 halamanMedicine: Full-Endoscopic Discectomy Via The Interlaminar Approach For Disc Herniation at L4-L5 and L5-S1Bell SwanBelum ada peringkat
- Journal Reading: Dr. Firdaus RamliDokumen22 halamanJournal Reading: Dr. Firdaus RamliBell SwanBelum ada peringkat
- Slipped Capital Femoral Epiphysis: MSC Otho, MRCS Assistant Lecturer of Orthopaedic at Ain Shams UniversityDokumen30 halamanSlipped Capital Femoral Epiphysis: MSC Otho, MRCS Assistant Lecturer of Orthopaedic at Ain Shams UniversityBell Swan100% (1)
- Romiyo/ MALE/21 Yo: Thursday, 10 TH January 2014Dokumen13 halamanRomiyo/ MALE/21 Yo: Thursday, 10 TH January 2014Bell SwanBelum ada peringkat
- MainDokumen9 halamanMainBell SwanBelum ada peringkat
- Mekong Bedah Hirsprung DiseaseDokumen12 halamanMekong Bedah Hirsprung DiseaseBell SwanBelum ada peringkat
- BurnsDokumen7 halamanBurnsBell SwanBelum ada peringkat
- Bab10 InflammatoryDisordersofBonesandJoints PDFDokumen50 halamanBab10 InflammatoryDisordersofBonesandJoints PDFBell SwanBelum ada peringkat
- Daftar PustakaDokumen3 halamanDaftar PustakaEKABelum ada peringkat
- MEDIWAYSDokumen79 halamanMEDIWAYSRaj KumarBelum ada peringkat
- Carmin WentworthDokumen4 halamanCarmin Wentworthapi-356549360Belum ada peringkat
- RTFDokumen32 halamanRTFrobert lee100% (1)
- 100 Ways To Achieve SuccessDokumen5 halaman100 Ways To Achieve SuccessSampath KumarBelum ada peringkat
- ANDA Check ListDokumen13 halamanANDA Check Listmadhupharma9623Belum ada peringkat
- Evaluation of The Health Beneficial Properties of The Aromatic Ether Myristicin, A Volatile Oil Derived From Various Plants SourcesDokumen17 halamanEvaluation of The Health Beneficial Properties of The Aromatic Ether Myristicin, A Volatile Oil Derived From Various Plants SourcesIndra syahputraBelum ada peringkat
- Thyriodectomy BrochureDokumen2 halamanThyriodectomy BrochureHeedahBelum ada peringkat
- Bio-Medical Waste Management Rules: DR NaveenDokumen26 halamanBio-Medical Waste Management Rules: DR Naveenmani kandanBelum ada peringkat
- Hypoxic Ischemic Hypoxic Ischemic E HL H E HL H Encephalopathty EncephalopathtyDokumen34 halamanHypoxic Ischemic Hypoxic Ischemic E HL H E HL H Encephalopathty EncephalopathtyKatrinaTandoc100% (1)
- A2 Edexcel Psychology Module 4 Unit 3 Clinical PsychologyDokumen32 halamanA2 Edexcel Psychology Module 4 Unit 3 Clinical PsychologyAyse KerimBelum ada peringkat
- Santhigiri Siddha Therapeutic GuideDokumen36 halamanSanthigiri Siddha Therapeutic Guidedrkiranrk83% (6)
- P 174 Insulin TherapyDokumen3 halamanP 174 Insulin TherapyJeane ClerkBelum ada peringkat
- Design of Novel Oral Films As Drug Delivery SystemDokumen7 halamanDesign of Novel Oral Films As Drug Delivery SystemReza-ul JalilBelum ada peringkat
- ASD Interventions Theories, Age Range and SettingsDokumen4 halamanASD Interventions Theories, Age Range and SettingstracycwBelum ada peringkat
- Double Burden of Malnutrition 2017Dokumen31 halamanDouble Burden of Malnutrition 2017Gîrneţ AlinaBelum ada peringkat