Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- 8 Right Triangle Trig Finding Missing Side and Angle KEY 1yua7xpDokumen2 halaman8 Right Triangle Trig Finding Missing Side and Angle KEY 1yua7xpRovinn 1375% (4)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- 321 E Lesson 17 PDFDokumen20 halaman321 E Lesson 17 PDFRovinn 13Belum ada peringkat
- Activity 1 Newtons 1st and 2nd Law PDFDokumen5 halamanActivity 1 Newtons 1st and 2nd Law PDFRovinn 13Belum ada peringkat
- Manila Science High School: Principal ThruDokumen1 halamanManila Science High School: Principal ThruRovinn 13Belum ada peringkat
- Manila Science High School: "I Am Masci"Dokumen4 halamanManila Science High School: "I Am Masci"Rovinn 13Belum ada peringkat
- Members: Merielle Anne Montano Danica Nubla Pauline Delo Santos Nino Gabriel Roque Patrick Janiel Bindadan Ken CruzDokumen3 halamanMembers: Merielle Anne Montano Danica Nubla Pauline Delo Santos Nino Gabriel Roque Patrick Janiel Bindadan Ken CruzRovinn 13Belum ada peringkat
- Book Report: The Prince and The Pauper by Mark Twain: Submitted By: Rovin Niño P. Montaño Gr. 7 - Descartes Mrs. AlcaydeDokumen6 halamanBook Report: The Prince and The Pauper by Mark Twain: Submitted By: Rovin Niño P. Montaño Gr. 7 - Descartes Mrs. AlcaydeRovinn 13Belum ada peringkat
- Letter To GodDokumen3 halamanLetter To GodRovinn 13Belum ada peringkat
- Handling Hazardous Materials at Home: Safety MustsDokumen2 halamanHandling Hazardous Materials at Home: Safety MustsRovinn 13Belum ada peringkat
- CHAPTER 3 SantrockDokumen29 halamanCHAPTER 3 SantrockJohn Ray SadgitapBelum ada peringkat
- Antepartum HemorrhageDokumen6 halamanAntepartum HemorrhageNurul SyuhadaBelum ada peringkat
- 10 Abnormal Umbilical CordDokumen30 halaman10 Abnormal Umbilical CordImam SuryaBelum ada peringkat
- Midwifery April 2014 PSDokumen10 halamanMidwifery April 2014 PSTheSummitExpressBelum ada peringkat
- NCP Alterations in Normal LaborDokumen9 halamanNCP Alterations in Normal LaborCameron De GuzmanBelum ada peringkat
- Waterbirth - HandoutDokumen1 halamanWaterbirth - Handoutpooja singhBelum ada peringkat
- PhilHealth ClaimForm3Dokumen2 halamanPhilHealth ClaimForm3slyn_boneheadBelum ada peringkat
- FHTMonitoringDokumen21 halamanFHTMonitoringlaarnie100% (1)
- Preterm Labour: Management GuidelinesDokumen44 halamanPreterm Labour: Management Guidelinesvacha sardar100% (1)
- Hypertension in PregnancyDokumen45 halamanHypertension in PregnancyMary Anne Cabalza ApinardoBelum ada peringkat
- Lecture-28 Placenta PreviaDokumen43 halamanLecture-28 Placenta PreviaMadhu Sudhan Pandeya100% (1)
- MK Fetal Lie and Presentation (OBGY)Dokumen9 halamanMK Fetal Lie and Presentation (OBGY)Moses Jr KazevuBelum ada peringkat
- Reassessing The Labor Curve in Nulliparous WomenDokumen5 halamanReassessing The Labor Curve in Nulliparous WomenPercy Astocaza FloresBelum ada peringkat
- DR NotesDokumen3 halamanDR Notesnoreen ellie100% (2)
- Case Pres PartographDokumen15 halamanCase Pres PartographJazzyleene Mejia UbagBelum ada peringkat
- U World Practice QuestionsDokumen3 halamanU World Practice QuestionsSavanna ChambersBelum ada peringkat
- Cesarean Section Audit FormatDokumen6 halamanCesarean Section Audit FormatRahul JalauniaBelum ada peringkat
- Cesarean Section MedicationsDokumen18 halamanCesarean Section MedicationsRhalhf Magtoto LegacionBelum ada peringkat
- Diabetes Gestacional 2022 NejmDokumen12 halamanDiabetes Gestacional 2022 NejmGabrielaBelum ada peringkat
- Tabla Fenton Niñas PrematuraDokumen1 halamanTabla Fenton Niñas PrematuraDahiana BolañosBelum ada peringkat
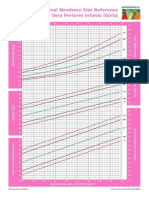
- Intergrowth21 Newborn Size Reference Charts (Girls)Dokumen2 halamanIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyBelum ada peringkat
- Oxytocin Drug StudyDokumen3 halamanOxytocin Drug Studysachi yuBelum ada peringkat
- Anthropometry in Perinatology and Beyond - of Changing Curves and Crossing CentilesDokumen77 halamanAnthropometry in Perinatology and Beyond - of Changing Curves and Crossing CentilesNEONATRIX AIIMSBelum ada peringkat
- Partogram and Its Relevance in Modern Obstetrics: Anjali Choudhary, Meenakshi TanwarDokumen5 halamanPartogram and Its Relevance in Modern Obstetrics: Anjali Choudhary, Meenakshi Tanwarأحمد صابرBelum ada peringkat
- Introduction To ObstetricsDokumen27 halamanIntroduction To ObstetricsDaniel NegeriBelum ada peringkat
- Multiple PregnancyDokumen20 halamanMultiple PregnancySelma FraBelum ada peringkat
- Determining Gravidity and Parity: I. GravidaDokumen6 halamanDetermining Gravidity and Parity: I. GravidaDanica CorpuzBelum ada peringkat
- JurnalDokumen7 halamanJurnalKarina GoysalBelum ada peringkat
- Public Program On Sensitisation of Midwifery Educator TrainingDokumen2 halamanPublic Program On Sensitisation of Midwifery Educator TrainingKUSH JOSHIBelum ada peringkat
- Treatment of Dystocia Dr. S.P.gaviTDokumen72 halamanTreatment of Dystocia Dr. S.P.gaviTsanjay gavit100% (11)