Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Cardio 2019 SponsorshipDokumen7 halamanCardio 2019 SponsorshipAnonymous MUKKNew94DBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Polyarteritis Nodosa TambahanDokumen3 halamanPolyarteritis Nodosa TambahanAnonymous MUKKNew94DBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Jurnal Polyarteritis NodosaDokumen7 halamanJurnal Polyarteritis NodosaAnonymous MUKKNew94DBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Tugas ResponsiDokumen2 halamanTugas ResponsiAnonymous MUKKNew94DBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Ton Miles Calculation 1Dokumen17 halamanTon Miles Calculation 1Alexander Armando Clemente Andrade100% (1)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Vermicomposting Learning ModulesDokumen6 halamanVermicomposting Learning ModulesPamara Prema Khannae100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- QFW Series SteamDokumen8 halamanQFW Series Steamnikon_fa50% (2)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- 11 - Chapter 3Dokumen27 halaman11 - Chapter 3sam000678Belum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- 2019 Auto Truck Key Blank Reference PDFDokumen188 halaman2019 Auto Truck Key Blank Reference PDFAlbert RodaBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Review Test 1: Circle The Correct Answers. / 5Dokumen4 halamanReview Test 1: Circle The Correct Answers. / 5XeniaBelum ada peringkat
- Workshop Manual: 3LD 450 3LD 510 3LD 450/S 3LD 510/S 4LD 640 4LD 705 4LD 820Dokumen33 halamanWorkshop Manual: 3LD 450 3LD 510 3LD 450/S 3LD 510/S 4LD 640 4LD 705 4LD 820Ilie Viorel75% (4)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Crop Science SyllabusDokumen42 halamanCrop Science Syllabusbetty makushaBelum ada peringkat
- Code of Conduct For Public OfficialDokumen17 halamanCode of Conduct For Public OfficialHaBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Oxygenation - NCPDokumen5 halamanOxygenation - NCPCazze SunioBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- ShotcreteDokumen7 halamanShotcreteafuhcivBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Permeability PropertiesDokumen12 halamanPermeability Propertieskiwi27_87Belum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Dadm Assesment #2: Akshat BansalDokumen24 halamanDadm Assesment #2: Akshat BansalAkshatBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Psyche Finals: Trans 2: Psychotic Disorder: SchizophreniaDokumen4 halamanPsyche Finals: Trans 2: Psychotic Disorder: SchizophreniajisooBelum ada peringkat
- Imaging Anatomy Brain and Spine Osborn 1 Ed 2020 PDFDokumen3.130 halamanImaging Anatomy Brain and Spine Osborn 1 Ed 2020 PDFthe gaangster100% (1)
- Majan Audit Report Final2Dokumen46 halamanMajan Audit Report Final2Sreekanth RallapalliBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- RA-035659 - CIVIL ENGINEER - Cebu - 5-2022Dokumen157 halamanRA-035659 - CIVIL ENGINEER - Cebu - 5-2022Ash AlbainBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Lifecycle of A Frog For Primary StudentsDokumen10 halamanLifecycle of A Frog For Primary StudentsMónika KissBelum ada peringkat
- Weather Prediction Using Machine Learning TechniquessDokumen53 halamanWeather Prediction Using Machine Learning Techniquessbakiz89Belum ada peringkat
- Preparation, Characterization, and Evaluation of Some Ashless Detergent-Dispersant Additives For Lubricating Engine OilDokumen10 halamanPreparation, Characterization, and Evaluation of Some Ashless Detergent-Dispersant Additives For Lubricating Engine OilNelson Enrique Bessone MadridBelum ada peringkat
- Project - Dreambox Remote Video StreamingDokumen5 halamanProject - Dreambox Remote Video StreamingIonut CristianBelum ada peringkat
- Vishakha BroadbandDokumen6 halamanVishakha Broadbandvishakha sonawaneBelum ada peringkat
- Exchange 2010 UnderstandDokumen493 halamanExchange 2010 UnderstandSeKoFieBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Film Interpretation and Reference RadiographsDokumen7 halamanFilm Interpretation and Reference RadiographsEnrique Tavira67% (3)
- Splices LAS 3rd Quarter Week 1Dokumen6 halamanSplices LAS 3rd Quarter Week 1Winnielyn Quarteros BarreraBelum ada peringkat
- Limited Alembic: Employee Related DataDokumen4 halamanLimited Alembic: Employee Related DataTp EarningsBelum ada peringkat
- Open Book Online: Syllabus & Pattern Class - XiDokumen1 halamanOpen Book Online: Syllabus & Pattern Class - XiaadityaBelum ada peringkat
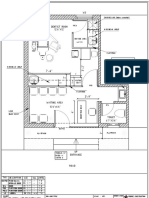
- Dental Clinic - Floor Plan R3-2Dokumen1 halamanDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- Competent Testing Requirements As Per Factory ActDokumen3 halamanCompetent Testing Requirements As Per Factory Actamit_lunia100% (1)
- MICRF230Dokumen20 halamanMICRF230Amador Garcia IIIBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)