Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- VK-53 (ВК-53) Erecting Cut-Out Switch: Maintenance ManualDokumen76 halamanVK-53 (ВК-53) Erecting Cut-Out Switch: Maintenance ManualhaileBelum ada peringkat
- Russian MarketDokumen228 halamanRussian Marketjelena_bojovic1Belum ada peringkat
- The Role of Complementary and Alternative Therapies in Managing Rheumatoid ArthritisDokumen1 halamanThe Role of Complementary and Alternative Therapies in Managing Rheumatoid Arthritisjelena_bojovic1Belum ada peringkat
- Muscle Fatigue in The Horse: A ReviewDokumen3 halamanMuscle Fatigue in The Horse: A Reviewjelena_bojovic1Belum ada peringkat
- E Following Acupoints Were Used in This Study (Needle Acupuncture) : Baihui (GV), Neiguan (HT), and Taichong (Liv) (See Also Figures (A) - (D) )Dokumen1 halamanE Following Acupoints Were Used in This Study (Needle Acupuncture) : Baihui (GV), Neiguan (HT), and Taichong (Liv) (See Also Figures (A) - (D) )jelena_bojovic1Belum ada peringkat
- Effect of Toe Treatments On The Fatigue Resistance of Structural Steel WeldsDokumen12 halamanEffect of Toe Treatments On The Fatigue Resistance of Structural Steel WeldsVicente Palazzo De MarinoBelum ada peringkat
- C.4. Quiz Conservation of BiodiversityDokumen2 halamanC.4. Quiz Conservation of Biodiversitylaura pongutaBelum ada peringkat
- Statistical Mechanics PDFDokumen578 halamanStatistical Mechanics PDFraymon6666100% (6)
- CCNP 300 410 ENARSI NetworkTUT 26 5 2021Dokumen104 halamanCCNP 300 410 ENARSI NetworkTUT 26 5 2021Olga BradyBelum ada peringkat
- Ap2 Safe ManipulationDokumen5 halamanAp2 Safe ManipulationDarthVader975Belum ada peringkat
- Assignment Class X Similar Triangles: A D E B CDokumen2 halamanAssignment Class X Similar Triangles: A D E B CCRPF School100% (1)
- Cleavage in MammalsDokumen51 halamanCleavage in MammalsIrfan Azram100% (4)
- Unipoxy LiningDokumen3 halamanUnipoxy LiningDien Thoai Nguyen HuuBelum ada peringkat
- Labangon Elementary School Diagbostic Test in Epp/Tle 6 Directions: Multiple Choice. Choose The Correct The Letter of The Correct AnswerDokumen4 halamanLabangon Elementary School Diagbostic Test in Epp/Tle 6 Directions: Multiple Choice. Choose The Correct The Letter of The Correct AnswerJulianFlorenzFalconeBelum ada peringkat
- Feu Sharing Stress MNGTDokumen58 halamanFeu Sharing Stress MNGTsquidsexoBelum ada peringkat
- Alien Magic - William Hamilton IIIDokumen179 halamanAlien Magic - William Hamilton IIICarlos Rodriguez100% (7)
- Foods 09 01560 PDFDokumen10 halamanFoods 09 01560 PDFkim cheBelum ada peringkat
- Manual Placa Mae Ga 945gcmx-s2 6.6Dokumen72 halamanManual Placa Mae Ga 945gcmx-s2 6.6luisb3toBelum ada peringkat
- Dell Inspiron 16 5000 (5625) Laptop - Dell IndiaDokumen5 halamanDell Inspiron 16 5000 (5625) Laptop - Dell IndiamubbunBelum ada peringkat
- Heil 4000 FeaturesDokumen1 halamanHeil 4000 FeaturesBogdan NgrBelum ada peringkat
- ABB Photovoltaic DisconnectorsDokumen6 halamanABB Photovoltaic DisconnectorsBog PenBelum ada peringkat
- QW PDFDokumen45 halamanQW PDFkarthikeyan PBelum ada peringkat
- Schueco+FW+50+SG+ +FW+60+SGDokumen1 halamanSchueco+FW+50+SG+ +FW+60+SGDaniel Nedelcu100% (1)
- Air Quality Index Analysis & PredictionDokumen34 halamanAir Quality Index Analysis & PredictionGottumukkala Sravan KumarBelum ada peringkat
- Gummetal Zastosowania Kliniczne 0Dokumen8 halamanGummetal Zastosowania Kliniczne 0ΑΛΕΞΑΝΔΡΟΣ ΣΤΕΦΑΝΗΣBelum ada peringkat
- Astm A479Dokumen7 halamanAstm A479Martin RomeroBelum ada peringkat
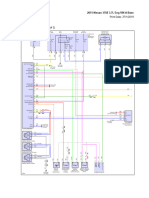
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDokumen69 halaman2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaBelum ada peringkat
- The CyclotronDokumen10 halamanThe CyclotronSupriya DuttaBelum ada peringkat
- Fundamental and Technical Analysis of Iron and Steel SIP PROJECTDokumen34 halamanFundamental and Technical Analysis of Iron and Steel SIP PROJECThaveuever910Belum ada peringkat
- Commissioning/Troubleshooting: Check List: C B A Yellow Grey Black TBPDokumen2 halamanCommissioning/Troubleshooting: Check List: C B A Yellow Grey Black TBPmohamedBelum ada peringkat
- X-Ray Radiation and Gamma RadiationDokumen13 halamanX-Ray Radiation and Gamma RadiationVence MeraBelum ada peringkat
- Effect of Calorie Restriction and Exercise On Type 2 DiabetesDokumen18 halamanEffect of Calorie Restriction and Exercise On Type 2 DiabetesDitya Monica 065Belum ada peringkat
- Lesson 4Dokumen10 halamanLesson 4Nagiri MuraliBelum ada peringkat
- Notes On Peck&Coyle Practical CriticismDokumen10 halamanNotes On Peck&Coyle Practical CriticismLily DameBelum ada peringkat