Anda mungkin juga menyukai
- Trading Floors WSDokumen86 halamanTrading Floors WSAlok Singh100% (3)
- International Journal of Pharmaceutical Science Invention (IJPSI)Dokumen3 halamanInternational Journal of Pharmaceutical Science Invention (IJPSI)inventionjournalsBelum ada peringkat
- Case Report EndometriosisDokumen4 halamanCase Report EndometriosischristinejoanBelum ada peringkat
- Massive Splenomegaly in Pregnancy: Case ReportDokumen7 halamanMassive Splenomegaly in Pregnancy: Case ReportRiniBelum ada peringkat
- 9.radha Et Al.Dokumen3 halaman9.radha Et Al.International Journal of Clinical and Biomedical Research (IJCBR)Belum ada peringkat
- Case Report Ghazanfar Page 130-132Dokumen3 halamanCase Report Ghazanfar Page 130-132sohailurologistBelum ada peringkat
- Ectopic Abdominal Pregnancies: About 2 CasesDokumen10 halamanEctopic Abdominal Pregnancies: About 2 CasesIJAR JOURNALBelum ada peringkat
- Medicine: Intrauterine Device Found in An Ovarian TumorDokumen5 halamanMedicine: Intrauterine Device Found in An Ovarian TumorRezky amalia basirBelum ada peringkat
- Girija BS, Sudha TR: AbstractDokumen4 halamanGirija BS, Sudha TR: AbstractALfuBelum ada peringkat
- Endometrial Adenocarcinoma and Polycystic Ovary Syndrome: Risk Factors, Management, and PrognosisDokumen4 halamanEndometrial Adenocarcinoma and Polycystic Ovary Syndrome: Risk Factors, Management, and PrognosisDikie MustofadijayaBelum ada peringkat
- Case Report: Postpartum Uterine Wound Dehiscence Leading To Secondary PPH: Unusual SequelaeDokumen4 halamanCase Report: Postpartum Uterine Wound Dehiscence Leading To Secondary PPH: Unusual SequelaemelisaberlianBelum ada peringkat
- OHSSDokumen4 halamanOHSSNur AnindyaBelum ada peringkat
- A Case of Giant Uterine Fibroid in A Toung WomanDokumen5 halamanA Case of Giant Uterine Fibroid in A Toung WomanTETINOUBelum ada peringkat
- Barel 2019Dokumen3 halamanBarel 2019Mariana González DíazBelum ada peringkat
- Meigs' Syndrome and Pseudo-Meigs' Syndrome: Report of Four Cases and Literature ReviewsDokumen6 halamanMeigs' Syndrome and Pseudo-Meigs' Syndrome: Report of Four Cases and Literature ReviewsAlfa FebriandaBelum ada peringkat
- A Case Study On Ruptured Tubal Pregnancy: July 2018Dokumen4 halamanA Case Study On Ruptured Tubal Pregnancy: July 2018Shilpu RtwBelum ada peringkat
- Case Report: Retained Intrauterine Device (IUD) : Triple Case Report and Review of The LiteratureDokumen9 halamanCase Report: Retained Intrauterine Device (IUD) : Triple Case Report and Review of The LiteratureYosie Yulanda PutraBelum ada peringkat
- Article 1615981002 PDFDokumen3 halamanArticle 1615981002 PDFMaria Lyn Ocariza ArandiaBelum ada peringkat
- 37 Ovariancyst PDFDokumen5 halaman37 Ovariancyst PDFRizka ApBelum ada peringkat
- Bazo Errante 2016 REVISED Ijtra1601084Dokumen4 halamanBazo Errante 2016 REVISED Ijtra1601084luisalfredo_montesBelum ada peringkat
- Uterine Fibroid EmbolizationDokumen8 halamanUterine Fibroid EmbolizationAlexandre Campos Moraes AmatoBelum ada peringkat
- A Case Study On Successful Ayurvedic Management of Heamorrhagic Ovarian CystDokumen4 halamanA Case Study On Successful Ayurvedic Management of Heamorrhagic Ovarian CystEditor IJTSRDBelum ada peringkat
- 1 s2.0 S0020729205000652 MainDokumen2 halaman1 s2.0 S0020729205000652 MainEndang Sri WidiyantiBelum ada peringkat
- 586-Article Text-1680-1-10-20221019Dokumen7 halaman586-Article Text-1680-1-10-20221019Rahma Dwi JayantiBelum ada peringkat
- Chronic Ovarian Ectopic Pregnancy - An Unusual Occurrence: A Case ReportDokumen5 halamanChronic Ovarian Ectopic Pregnancy - An Unusual Occurrence: A Case Reportindex PubBelum ada peringkat
- Laparoscopic Management of Cervical-Isthmic Pregnancy: A Proposal MethodDokumen4 halamanLaparoscopic Management of Cervical-Isthmic Pregnancy: A Proposal MethodDinorah MarcelaBelum ada peringkat
- Bilateral Tubo-Ovarian Abscess After Cesarean Delivery: A Case Report and Literature ReviewDokumen4 halamanBilateral Tubo-Ovarian Abscess After Cesarean Delivery: A Case Report and Literature ReviewIntan PermataBelum ada peringkat
- Ectopic PregnancyDokumen7 halamanEctopic PregnancyDeepshikha MahapatraBelum ada peringkat
- Spontaneous Perforated Pyometra With An Intrauterine Device in Menopause: A Case ReportDokumen2 halamanSpontaneous Perforated Pyometra With An Intrauterine Device in Menopause: A Case ReportTomy SaputraBelum ada peringkat
- Lactating Adenoma A Case ReportDokumen3 halamanLactating Adenoma A Case ReportInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Case Report: Tubocutaneous FistulaDokumen2 halamanCase Report: Tubocutaneous FistulapebinscribdBelum ada peringkat
- Primary Umbilical Endometriosis. Case Report and Discussion On Management OptionsDokumen7 halamanPrimary Umbilical Endometriosis. Case Report and Discussion On Management Optionsari naBelum ada peringkat
- Hematometra in Uterus Didelphys With Right Hemivagina and Right Renal AgenesisDokumen3 halamanHematometra in Uterus Didelphys With Right Hemivagina and Right Renal AgenesisDexter BluesBelum ada peringkat
- Ectopic Pregnancy in Uncommon Implantation Sites: The Egyptian Journal of Radiology and Nuclear MedicineDokumen10 halamanEctopic Pregnancy in Uncommon Implantation Sites: The Egyptian Journal of Radiology and Nuclear MedicinerezachandraBelum ada peringkat
- Journal of Medical Case ReportsDokumen4 halamanJournal of Medical Case ReportsAna Di JayaBelum ada peringkat
- 1 s2.0 S1028455911001823 MainDokumen6 halaman1 s2.0 S1028455911001823 MainFatimah AssagafBelum ada peringkat
- Unavoidable Myomectomy During Cesarean Section: A Case ReportDokumen3 halamanUnavoidable Myomectomy During Cesarean Section: A Case ReportGuia Nina DuranBelum ada peringkat
- University Journal of Surgery and Surgical Specialities: Dhivya Lakshmi S JDokumen4 halamanUniversity Journal of Surgery and Surgical Specialities: Dhivya Lakshmi S JYonathanWaisendiBelum ada peringkat
- Gynec ExamDokumen45 halamanGynec ExamPutri Anggia BungaBelum ada peringkat
- Ovarian Pregnancy: Two Case Reports.: Jayeeta Roy, Anindita Sinha BabuDokumen5 halamanOvarian Pregnancy: Two Case Reports.: Jayeeta Roy, Anindita Sinha BabuAndriyani MuslimBelum ada peringkat
- Chronic Non-Puerperal Uterine Inversion Mimicking Complete Uterine ProlapsedDokumen6 halamanChronic Non-Puerperal Uterine Inversion Mimicking Complete Uterine ProlapsedCentral Asian StudiesBelum ada peringkat
- Aphallia Associate Fistula RectouretraDokumen3 halamanAphallia Associate Fistula Rectouretraeni nadzhifahBelum ada peringkat
- Mullerian Agenesis: An Unusual Presentation As Hematometra and Bilateral HematosalpinxDokumen2 halamanMullerian Agenesis: An Unusual Presentation As Hematometra and Bilateral Hematosalpinxwanwan_adongBelum ada peringkat
- OGIJ 06 00208hematometra PDFDokumen4 halamanOGIJ 06 00208hematometra PDFMarthin ArdoBelum ada peringkat
- Primary Splenic Pregnancy With Hemorrhagic Shock: Hongyan GaoDokumen4 halamanPrimary Splenic Pregnancy With Hemorrhagic Shock: Hongyan GaoClan MéxicoBelum ada peringkat
- Abrasio PlacentaDokumen3 halamanAbrasio Placentamuhammad azamBelum ada peringkat
- Endometriosis With Hemorrhagic AscitiesDokumen5 halamanEndometriosis With Hemorrhagic AscitiesGavin TexeirraBelum ada peringkat
- Suspected Illegal Abortion and Unsafe Abortion Leading To Uterine RuptureDokumen4 halamanSuspected Illegal Abortion and Unsafe Abortion Leading To Uterine Ruptureoke boskuBelum ada peringkat
- Placenta Increta Causing Um in The 26th Week of Pregnancy 2Dokumen3 halamanPlacenta Increta Causing Um in The 26th Week of Pregnancy 2Kester ApostolBelum ada peringkat
- Van Wyk Grumbach Syndrome The Importance of Thyroi 2024 International JournDokumen5 halamanVan Wyk Grumbach Syndrome The Importance of Thyroi 2024 International JournRonald QuezadaBelum ada peringkat
- Successful Management of Giant Hydrocolpos in A LiDokumen3 halamanSuccessful Management of Giant Hydrocolpos in A LiVictor FernandoBelum ada peringkat
- Diagnosis and Management of Intramural Ectopic PregnancyDokumen4 halamanDiagnosis and Management of Intramural Ectopic PregnancyDinorah MarcelaBelum ada peringkat
- Circ PlacentDokumen7 halamanCirc PlacentnicoavilaBelum ada peringkat
- Abnormal Uterine Bleeding in A 39 Year OldDokumen16 halamanAbnormal Uterine Bleeding in A 39 Year OldEliana GerzonBelum ada peringkat
- Ilovepdf MergedDokumen53 halamanIlovepdf MergedHardikBelum ada peringkat
- World Journal of Colorectal SurgeryDokumen7 halamanWorld Journal of Colorectal Surgeryyulita heraBelum ada peringkat
- Homoeopathic Management of Ovarian Cyst - A Case RDokumen7 halamanHomoeopathic Management of Ovarian Cyst - A Case RB. B.Belum ada peringkat
- LBM 6-Bheta Silfana Ulul AzmiDokumen41 halamanLBM 6-Bheta Silfana Ulul AzminafikayBelum ada peringkat
- How to Perform Ultrasonography in EndometriosisDari EverandHow to Perform Ultrasonography in EndometriosisStefano GuerrieroBelum ada peringkat
- Management of Occult GI Bleeding: A Clinical GuideDari EverandManagement of Occult GI Bleeding: A Clinical GuideMicheal TadrosBelum ada peringkat
- DR Leonar, DENGUE PIN PAPDI 2019Dokumen51 halamanDR Leonar, DENGUE PIN PAPDI 2019Yuni Purnama SariBelum ada peringkat
- Oftalmologi Indonesia. Vol.6 (2) : 92-103.: Daftar PustakaDokumen1 halamanOftalmologi Indonesia. Vol.6 (2) : 92-103.: Daftar PustakaYuni Purnama SariBelum ada peringkat
- JR 3Dokumen10 halamanJR 3Yuni Purnama SariBelum ada peringkat
- JR 6Dokumen8 halamanJR 6Yuni Purnama SariBelum ada peringkat
- 50 Interview Questions For Adryenn AshleyDokumen5 halaman50 Interview Questions For Adryenn AshleyAdryenn AshleyBelum ada peringkat
- Translator Resume SampleDokumen2 halamanTranslator Resume SampleIsabel JimenezBelum ada peringkat
- Life in The Middle Ages Unit Study - Grade 8Dokumen21 halamanLife in The Middle Ages Unit Study - Grade 8HCSLearningCommonsBelum ada peringkat
- DD McqsDokumen21 halamanDD McqsSyeda MunazzaBelum ada peringkat
- Karling Aguilera-Fort ResumeDokumen4 halamanKarling Aguilera-Fort Resumeapi-3198760590% (1)
- Marketing Ethics Amal 12-09-10Dokumen11 halamanMarketing Ethics Amal 12-09-10amalroy1986Belum ada peringkat
- IHL 1 BALLB ProjectDokumen16 halamanIHL 1 BALLB Projectabcde fghikjBelum ada peringkat
- How Common Indian People Take Investment Decisions Exploring Aspects of Behavioral Economics in IndiaDokumen3 halamanHow Common Indian People Take Investment Decisions Exploring Aspects of Behavioral Economics in IndiaInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- LESSON 1 Overview of Toeic Speaking WritingDokumen29 halamanLESSON 1 Overview of Toeic Speaking WritingPhạm Thị HuyềnBelum ada peringkat
- M 1.2 RMDokumen16 halamanM 1.2 RMk thejeshBelum ada peringkat
- Daily Lesson Log in Math 9Dokumen13 halamanDaily Lesson Log in Math 9Marjohn PalmesBelum ada peringkat
- Coronel Vs CA, GR No 103577Dokumen10 halamanCoronel Vs CA, GR No 103577AddAllBelum ada peringkat
- Cs6109 - Compiler Design: Lab AssignmentDokumen8 halamanCs6109 - Compiler Design: Lab AssignmentvezhaventhanBelum ada peringkat
- Warm Pretend Lead Line Cater Resist Provide Reflect Anticipate Advertise Range Sentence AccessDokumen24 halamanWarm Pretend Lead Line Cater Resist Provide Reflect Anticipate Advertise Range Sentence AccessJacinto Leite Aquino RêgoBelum ada peringkat
- Mission: Children'SDokumen36 halamanMission: Children'SWillian A. Palacio MurilloBelum ada peringkat
- 1940 - English Missal - Order of MassDokumen15 halaman1940 - English Missal - Order of MassDavid ConleyBelum ada peringkat
- Seng2011 - Assignment 5Dokumen11 halamanSeng2011 - Assignment 5yajnas1996Belum ada peringkat
- Convekta Training MethodsDokumen9 halamanConvekta Training MethodsTech PadawanBelum ada peringkat
- 5 - Data Room Procedure TemplatesDokumen8 halaman5 - Data Room Procedure TemplatesnajahBelum ada peringkat
- 434-Article Text-2946-1-10-20201113Dokumen9 halaman434-Article Text-2946-1-10-20201113Rian Armansyah ManggeBelum ada peringkat
- Strucni TekstDokumen6 halamanStrucni TekstDusanBelum ada peringkat
- Manila Trading & Supply Co. v. Manila Trading Labor Assn (1953)Dokumen2 halamanManila Trading & Supply Co. v. Manila Trading Labor Assn (1953)Zan BillonesBelum ada peringkat
- Child and Adolescent Psychiatry ST1Dokumen6 halamanChild and Adolescent Psychiatry ST1danielBelum ada peringkat
- 158 Carino vs. CADokumen2 halaman158 Carino vs. CAFrancesca Isabel Montenegro67% (3)
- Absolute Community of Property vs. Conjugal Partnership of GainsDokumen7 halamanAbsolute Community of Property vs. Conjugal Partnership of GainsJill LeaBelum ada peringkat
- Transparency IIDokumen25 halamanTransparency IIKatyanne ToppingBelum ada peringkat
- General Service ListDokumen77 halamanGeneral Service ListMustafa GüneşBelum ada peringkat
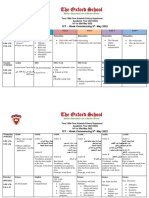
- Term 3 Mid-Term Assessment ScheduleDokumen9 halamanTerm 3 Mid-Term Assessment ScheduleRabia MoeedBelum ada peringkat
- History of English Culture and Literature MidDokumen4 halamanHistory of English Culture and Literature Midfirdasalsa59Belum ada peringkat