Anda mungkin juga menyukai
- Vendor ListDokumen55 halamanVendor ListbigpoelBelum ada peringkat
- Primary 4 / Grade 4: Full Name: School: Index NumberDokumen39 halamanPrimary 4 / Grade 4: Full Name: School: Index NumberLydia ApsariBelum ada peringkat
- 4.2BHow To Measure Guide ApparelsDokumen37 halaman4.2BHow To Measure Guide ApparelsAlokKumarBelum ada peringkat
- Interactive Science 1A: Part A Sectional Exercise 1.1 Concept Checking p.1Dokumen139 halamanInteractive Science 1A: Part A Sectional Exercise 1.1 Concept Checking p.1anson302302Belum ada peringkat
- Cold Weather Survival Guide: "Be Prepared" For Winter Safety - Don't Get Left Out in The C.O.L.DDokumen7 halamanCold Weather Survival Guide: "Be Prepared" For Winter Safety - Don't Get Left Out in The C.O.L.DDavid BaymillerBelum ada peringkat
- Geography Grade 8 June Exam 2019Dokumen7 halamanGeography Grade 8 June Exam 2019Israela Kimba0% (1)
- BM Thermal and Moisture ProtectionDokumen62 halamanBM Thermal and Moisture ProtectionAlvin Bariuan GuiyabBelum ada peringkat
- Splbe - Master Plumber (Psme-Sa, Uap, Pice) Quiz: MP Splbe Compiled By: O.T. AnoDokumen3 halamanSplbe - Master Plumber (Psme-Sa, Uap, Pice) Quiz: MP Splbe Compiled By: O.T. AnoReymond IgayaBelum ada peringkat
- FYP - Thermal Comfort Investigation of Multi Storey BuildingDokumen267 halamanFYP - Thermal Comfort Investigation of Multi Storey BuildingMuhd ZuhairiBelum ada peringkat
- Secondary 2Dokumen17 halamanSecondary 2kusniar deny permana100% (1)
- Unit 8: Sitcom: Which Dress Do You Like Better? Scene 1Dokumen2 halamanUnit 8: Sitcom: Which Dress Do You Like Better? Scene 1Angel Jesus Alvarez SierraBelum ada peringkat
- MICRO PARA Lab Environmental SamplingDokumen7 halamanMICRO PARA Lab Environmental SamplingShene Claire VigillaBelum ada peringkat
- Worksheet Class Ix - ScienceDokumen38 halamanWorksheet Class Ix - Sciencemegha21decBelum ada peringkat
- 6398773-Class 7 - PMT - Science - Set 1 - Vikrant - QPDokumen4 halaman6398773-Class 7 - PMT - Science - Set 1 - Vikrant - QPSriram JakkamsettyBelum ada peringkat
- NCERT Solutions For Class 7 Science Chapter 4 HeatDokumen1 halamanNCERT Solutions For Class 7 Science Chapter 4 HeatMadhav KaushikBelum ada peringkat
- Olympiad - TMP MsDokumen5 halamanOlympiad - TMP Msaaliya shamnadBelum ada peringkat
- Class Vii Science 2017 2Dokumen3 halamanClass Vii Science 2017 2Tanya GoyalBelum ada peringkat
- Class VII Science Annual Exam 2017 18Dokumen2 halamanClass VII Science Annual Exam 2017 18Akshara KarthikBelum ada peringkat
- FPE 2201 Set IIDokumen2 halamanFPE 2201 Set IIpsaid4Belum ada peringkat
- Interactive Science 1A: Part A Sectional Exercise 1.1 Concept Checking p.1Dokumen139 halamanInteractive Science 1A: Part A Sectional Exercise 1.1 Concept Checking p.1anson302302Belum ada peringkat
- B. Sc. Hons Agriculture 1st Semester December 2017Dokumen36 halamanB. Sc. Hons Agriculture 1st Semester December 2017RYZEN BBelum ada peringkat
- Conserve Electrical Energy - Quizizz POST TESTDokumen2 halamanConserve Electrical Energy - Quizizz POST TESTpilaryvonne6Belum ada peringkat
- Activity 2 MeteorologyDokumen3 halamanActivity 2 MeteorologyElaisa BassigBelum ada peringkat
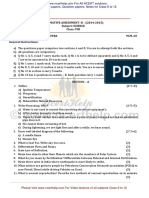
- SUMMATIVE ASSESSMENT-II - (2014-2015) Subject: SCIENCE Class: VIII Time 2: 30 Hrs. + 30 Mins For OTBA M.M. 60 General InstructionsDokumen3 halamanSUMMATIVE ASSESSMENT-II - (2014-2015) Subject: SCIENCE Class: VIII Time 2: 30 Hrs. + 30 Mins For OTBA M.M. 60 General InstructionsMd ImranBelum ada peringkat
- Questions & Answers: Indian Olympiad Qualifier in Junior Science 2020-21 (IOQJS) Part-IIDokumen13 halamanQuestions & Answers: Indian Olympiad Qualifier in Junior Science 2020-21 (IOQJS) Part-IIYash PatelBelum ada peringkat
- EVSdocDokumen4 halamanEVSdocvikassasBelum ada peringkat
- Secondary 1Dokumen17 halamanSecondary 1Architecte UrbanisteBelum ada peringkat
- Worksheet 1 - Air, Water, Weather 2Dokumen4 halamanWorksheet 1 - Air, Water, Weather 2Jain PushpBelum ada peringkat
- Uk To Break Heat Record British English StudentDokumen10 halamanUk To Break Heat Record British English StudentNatali PetruhBelum ada peringkat
- Mps Public School: Annual Examination 2022Dokumen2 halamanMps Public School: Annual Examination 2022PRIYA KUMARIBelum ada peringkat
- Delhi Public School Jodhpur: Subject - Science Class - VIII Time: 2 Hours M.M.: 80Dokumen4 halamanDelhi Public School Jodhpur: Subject - Science Class - VIII Time: 2 Hours M.M.: 80Niranjan KumawatBelum ada peringkat
- Free NSO Sample Paper: ScienceDokumen9 halamanFree NSO Sample Paper: Sciencekishoreprithika100% (1)
- Instructions For Students: UHL2412/SEM22018/2019DEL/CMLHS/UMPDokumen5 halamanInstructions For Students: UHL2412/SEM22018/2019DEL/CMLHS/UMPwan nur mursyidahBelum ada peringkat
- Indian National Junior Science Olympiad Solved Paper 2013Dokumen22 halamanIndian National Junior Science Olympiad Solved Paper 2013vedjainBelum ada peringkat
- Erasmus Örnek Duyuru 2Dokumen4 halamanErasmus Örnek Duyuru 2aBelum ada peringkat
- Carbon Footprint WorksheetDokumen2 halamanCarbon Footprint WorksheetPawan PatilBelum ada peringkat
- GS May 28, 2023 PDFDokumen16 halamanGS May 28, 2023 PDFBishal LaskarBelum ada peringkat
- Science ExamDokumen7 halamanScience Examshanvishah1712Belum ada peringkat
- The Break Out (Scientific Method)Dokumen10 halamanThe Break Out (Scientific Method)gabriella sanonBelum ada peringkat
- Survey Template 05Dokumen31 halamanSurvey Template 05Mabodo SofaBelum ada peringkat
- 2122 F1 is 1st Term Exam - 複本Dokumen9 halaman2122 F1 is 1st Term Exam - 複本chengelizeBelum ada peringkat
- Quarter Assessment in Mathematics 7: Mother Guaini School, IncDokumen3 halamanQuarter Assessment in Mathematics 7: Mother Guaini School, IncJanGianVillarealBelum ada peringkat
- Science: Science Marking Scheme Paper 2 Section A AnswersDokumen7 halamanScience: Science Marking Scheme Paper 2 Section A AnswersSuaanBelum ada peringkat
- Science PaperDokumen4 halamanScience PaperVIMLA BBelum ada peringkat
- Integrated Science Assessment 1Dokumen22 halamanIntegrated Science Assessment 1MARICEL MIRANDABelum ada peringkat
- Vision Prelims Test 3Dokumen58 halamanVision Prelims Test 3anurag mauryaBelum ada peringkat
- 2019 Nov Exam 1Dokumen6 halaman2019 Nov Exam 1Petro Susan BarnardBelum ada peringkat
- Amity International School, Noida Science Worksheet Class Vii Chapter - HeatDokumen2 halamanAmity International School, Noida Science Worksheet Class Vii Chapter - HeatDakshBelum ada peringkat
- Ukoro Frank Ecology EXAMINATIONDokumen4 halamanUkoro Frank Ecology EXAMINATIONFrank UkoroBelum ada peringkat
- Title: Is It Hot or Cold? LEARNING COMPETENCY: Apply Knowledge of Temperature in Solving EverydayDokumen89 halamanTitle: Is It Hot or Cold? LEARNING COMPETENCY: Apply Knowledge of Temperature in Solving Everydayshiva avelBelum ada peringkat
- Science Solved-Sample-Paper-Class-7-SA1-Set-1Dokumen5 halamanScience Solved-Sample-Paper-Class-7-SA1-Set-1SushilBelum ada peringkat
- Vision IASDokumen19 halamanVision IASAmbuj sharmaBelum ada peringkat
- Ch-8 SolutionDokumen9 halamanCh-8 SolutionIdrissMahdi OkiyeBelum ada peringkat
- Questions On This Quiz Are Based On Information From .: Earth Science: SeasonsDokumen2 halamanQuestions On This Quiz Are Based On Information From .: Earth Science: SeasonschristalBelum ada peringkat
- CE Exam Midterm SET A1Dokumen4 halamanCE Exam Midterm SET A1Hanny Creselle Banac GravinoBelum ada peringkat
- Test 1 - September 16, 2010: Use The Graph Shown To Answer Questions 4 and 5Dokumen5 halamanTest 1 - September 16, 2010: Use The Graph Shown To Answer Questions 4 and 5Jessica IsemanBelum ada peringkat
- Test 1 - September 16, 2010: Use The Graph Shown To Answer Questions 4 and 5Dokumen6 halamanTest 1 - September 16, 2010: Use The Graph Shown To Answer Questions 4 and 5Jessica IsemanBelum ada peringkat
- P3 SCIENCE TEST 4 (CHP 8 and 9)Dokumen4 halamanP3 SCIENCE TEST 4 (CHP 8 and 9)Wilson SunantoBelum ada peringkat
- MEC653 ODL Test 2-Mac 2022Dokumen14 halamanMEC653 ODL Test 2-Mac 2022Muhammad Zuhairy jabarBelum ada peringkat
- SOC ReviewDokumen2 halamanSOC ReviewDino Manuel PrestadoBelum ada peringkat
- Test Bank Chapter 1Dokumen4 halamanTest Bank Chapter 1teafBelum ada peringkat
- PASSAGES EditedDokumen56 halamanPASSAGES EditedNIZA GALLEGOSBelum ada peringkat
- Temperature and Heat 1691413509Dokumen2 halamanTemperature and Heat 1691413509THREE BROTHERS LIFESTYLEBelum ada peringkat
- Science Final Unseen QuestionDokumen3 halamanScience Final Unseen QuestionEX CORE GAMERBelum ada peringkat
- Weather Studies: The Commonwealth and International Library: Rural and Environmental Studies DivisionDari EverandWeather Studies: The Commonwealth and International Library: Rural and Environmental Studies DivisionBelum ada peringkat
- Individual Assignment Q2Dokumen1 halamanIndividual Assignment Q2Muhd ZuhairiBelum ada peringkat
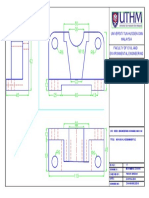
- Example 1 in Module 4.1Dokumen1 halamanExample 1 in Module 4.1Muhd ZuhairiBelum ada peringkat
- Full Report AssmentDokumen25 halamanFull Report AssmentMuhd ZuhairiBelum ada peringkat
- Civil Engineering Software (BFC 43201) SEMESTER 2 SESSION 2017/2018 Foc Assignment - Indivudual Section 5 Answer All QuestionsDokumen1 halamanCivil Engineering Software (BFC 43201) SEMESTER 2 SESSION 2017/2018 Foc Assignment - Indivudual Section 5 Answer All QuestionsMuhd ZuhairiBelum ada peringkat
- Chapter 2 - Classification of Cross-SectionDokumen20 halamanChapter 2 - Classification of Cross-SectionMuhd Zuhairi100% (2)
- Lancia MerchandisingDokumen19 halamanLancia MerchandisingManuela BernardiBelum ada peringkat
- Sophie Woodward 21-39Dokumen16 halamanSophie Woodward 21-39Florina FrancuBelum ada peringkat
- Dress Codes - Singapore American SchoolDokumen8 halamanDress Codes - Singapore American SchoolNguyen Phuong LinhBelum ada peringkat
- Wishlist Star Stable OnlineDokumen9 halamanWishlist Star Stable OnlineAbbie FireflyBelum ada peringkat
- Dramatic - Classic - Gamine: What Not To WearDokumen3 halamanDramatic - Classic - Gamine: What Not To Wearjuliensorel325Belum ada peringkat
- 2009-10 KIPP Academy Middle Family HandbookDokumen33 halaman2009-10 KIPP Academy Middle Family HandbookpsuthramBelum ada peringkat
- Day 7 Asking & Describing What Someone Is WearingDokumen21 halamanDay 7 Asking & Describing What Someone Is WearingIntan NelwanBelum ada peringkat
- Lamborghini Katalog 2012Dokumen280 halamanLamborghini Katalog 2012bn2552Belum ada peringkat
- Price List enDokumen6 halamanPrice List enSergiu LaurentiuBelum ada peringkat
- Difference Between Indian English and American EnglishDokumen7 halamanDifference Between Indian English and American EnglishAnonymous f16rdvBelum ada peringkat
- Wadfrance Wad MagDokumen28 halamanWadfrance Wad Maghello3321100% (1)
- Price List Apparel (Naik Harga) 1 Jan 2022 (Clandys Denpasar Dan Hompimpah)Dokumen6 halamanPrice List Apparel (Naik Harga) 1 Jan 2022 (Clandys Denpasar Dan Hompimpah)Herman Ghifary Part IIIBelum ada peringkat
- Test Your English VocabDokumen10 halamanTest Your English VocabLu SanBelum ada peringkat
- What Are You Like? What's He Like? What's She Like?Dokumen9 halamanWhat Are You Like? What's He Like? What's She Like?Adelaida Ruiz VelandiaBelum ada peringkat
- Employee Handbook - IGT Technologies PhilippinesDokumen28 halamanEmployee Handbook - IGT Technologies PhilippinesIra Angelo CorderoBelum ada peringkat
- FashionDokumen42 halamanFashionBùi TânBelum ada peringkat
- Winter Clothes Esl Picture Dictionary For Kids PDFDokumen1 halamanWinter Clothes Esl Picture Dictionary For Kids PDFVirginia JbBelum ada peringkat
- Runner - SandDokumen6 halamanRunner - SandAmirulBelum ada peringkat
- BeWare Clothing Is An Apparel Fashion and Clothing Shop For Women and MenDokumen4 halamanBeWare Clothing Is An Apparel Fashion and Clothing Shop For Women and MenChristian Mark AliñoBelum ada peringkat
- 10 0876 01 6RP AFP tcm143-701160Dokumen12 halaman10 0876 01 6RP AFP tcm143-701160SnowiestSleetBelum ada peringkat
- Dolce and Gabbana ManDokumen13 halamanDolce and Gabbana ManIacob Corneliu-VictorBelum ada peringkat
- Y12 - Hand - Book - 2019 2Dokumen22 halamanY12 - Hand - Book - 2019 2tiagoBelum ada peringkat
- Lesson Goals: To Recognize The Different Types of Garment To Use Adjectives in Comparative Form ProperlyDokumen3 halamanLesson Goals: To Recognize The Different Types of Garment To Use Adjectives in Comparative Form Properlym a y uBelum ada peringkat
- High Note 3 Teachers Book Removed PDF Prom English Language 5Dokumen1 halamanHigh Note 3 Teachers Book Removed PDF Prom English Language 5Дана ЛастовенкоBelum ada peringkat
- Topic-Men'S Preppy Style: Submitted byDokumen10 halamanTopic-Men'S Preppy Style: Submitted byDivyaBelum ada peringkat
- Buy Tokyo Talkies Women White Solid Sweatshirt - Sweatshirts For Women 10853992 MyntraDokumen1 halamanBuy Tokyo Talkies Women White Solid Sweatshirt - Sweatshirts For Women 10853992 MyntraAnnapurna HirematBelum ada peringkat