Anda mungkin juga menyukai
- Magical Self AffirmationDokumen1 halamanMagical Self AffirmationElanghovan ArumugamBelum ada peringkat
- 3 GranthiDokumen1 halaman3 GranthiElanghovan Arumugam100% (1)
- Acu Point TreasureDokumen1 halamanAcu Point TreasureElanghovan ArumugamBelum ada peringkat
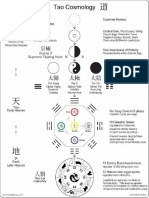
- Tao 1Dokumen1 halamanTao 1Elanghovan Arumugam50% (2)
- MK SastryDokumen1 halamanMK SastryElanghovan ArumugamBelum ada peringkat
- Introduction To Neijing Classical Acupuncture Part II: Clinical TheoryDokumen14 halamanIntroduction To Neijing Classical Acupuncture Part II: Clinical TheoryElanghovan ArumugamBelum ada peringkat
- Nutrients Chap 12Dokumen3 halamanNutrients Chap 12Elanghovan ArumugamBelum ada peringkat
- BD Chem PTableDokumen14 halamanBD Chem PTableElanghovan ArumugamBelum ada peringkat
- The Hippocratic View On Humors and Human Temperament: January 2015Dokumen6 halamanThe Hippocratic View On Humors and Human Temperament: January 2015Elanghovan ArumugamBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Acoustical Determinations On A Composite Materials (Extruded Polystyrene Type/ Cork)Dokumen6 halamanAcoustical Determinations On A Composite Materials (Extruded Polystyrene Type/ Cork)pinoyarkiBelum ada peringkat
- Shopping Centres, 10?FIRE?ENGINEERING ?CASE? STUDIES? IN? FINLAND?Dokumen52 halamanShopping Centres, 10?FIRE?ENGINEERING ?CASE? STUDIES? IN? FINLAND?Bambang Setyo UtomoBelum ada peringkat
- Weld Simulator PDFDokumen4 halamanWeld Simulator PDFAmilin HatiaraBelum ada peringkat
- Commercial Drafting and Detailing 4th Edition by Jefferis and Smith ISBN Solution ManualDokumen8 halamanCommercial Drafting and Detailing 4th Edition by Jefferis and Smith ISBN Solution Manualmatthew100% (22)
- Importance of Communication in SocietyDokumen16 halamanImportance of Communication in SocietyPh843 King's Kids StudentCenterBelum ada peringkat
- Strategi Pengembangan Dan Analisis Swot Pada Pt. Garuda Indonesia TBKDokumen12 halamanStrategi Pengembangan Dan Analisis Swot Pada Pt. Garuda Indonesia TBKtedzmedicalBelum ada peringkat
- ECEN 314: Matlab Project 1 Fourier Series Synthesizer: Due April 8th, 2013Dokumen3 halamanECEN 314: Matlab Project 1 Fourier Series Synthesizer: Due April 8th, 2013Dante HavershamBelum ada peringkat
- INVESTIGATION REPORT eFNCR 076 - BOP Test Plug Stuck in CHHDokumen4 halamanINVESTIGATION REPORT eFNCR 076 - BOP Test Plug Stuck in CHHOmer Abd Al NasserBelum ada peringkat
- Fundamentals of Momentum, Heat and Mass TransferDokumen87 halamanFundamentals of Momentum, Heat and Mass TransferSlim KanounBelum ada peringkat
- Educational PhilosophyDokumen2 halamanEducational Philosophyapi-393451535Belum ada peringkat
- The Determinants of MoralityDokumen10 halamanThe Determinants of MoralityKaimi Ardee BorjaBelum ada peringkat
- Notebook Three: Leadership Begins With An AttitudeDokumen19 halamanNotebook Three: Leadership Begins With An AttitudeJessie James YapaoBelum ada peringkat
- Obturation of Root Canal LectureDokumen8 halamanObturation of Root Canal LectureOsama AsadiBelum ada peringkat
- Learning Chara Dasa K N RaoDokumen34 halamanLearning Chara Dasa K N RaoVikram Kumar100% (3)
- Lab Manual Molecular BiologyDokumen19 halamanLab Manual Molecular BiologyLockerLingBelum ada peringkat
- Amateur Photographer - May 28, 2016Dokumen84 halamanAmateur Photographer - May 28, 2016Lee100% (1)
- The Final Revesion of My Paper in Wulfenia Journal PDFDokumen22 halamanThe Final Revesion of My Paper in Wulfenia Journal PDFAli Abdul-RahmanBelum ada peringkat
- Meanings Symbols and Local Wisdomin The Pinakang Dance Movements Costumesand Accessories of The Kimaragang in SabahDokumen6 halamanMeanings Symbols and Local Wisdomin The Pinakang Dance Movements Costumesand Accessories of The Kimaragang in SabahFredBTC007Belum ada peringkat
- SICK DT35 Setup InstructionsDokumen6 halamanSICK DT35 Setup InstructionsTalicni TomBelum ada peringkat
- Presentation Template IR For ManagementDokumen13 halamanPresentation Template IR For ManagementYosia SuhermanBelum ada peringkat
- Scholarship Application FormDokumen4 halamanScholarship Application FormAnonymous fY1HXgJRkzBelum ada peringkat
- Chios Reiki Attunement ManualDokumen12 halamanChios Reiki Attunement Manualkeithmac100% (1)
- Awodele - Observations On W.D. Gann, Vol. 1 PeriodicityDokumen82 halamanAwodele - Observations On W.D. Gann, Vol. 1 Periodicityforex50087% (23)
- How To Get Google Maps API Key For Android. Issues and Errors SolvedDokumen11 halamanHow To Get Google Maps API Key For Android. Issues and Errors SolvedFrancisco FeitosaBelum ada peringkat
- Froebelian Eglantyne Jebb, Save The ChildrenDokumen3 halamanFroebelian Eglantyne Jebb, Save The ChildrenLifeinthemix_FroebelBelum ada peringkat
- Form IR Civil Proyek PLTMG MERAUKE-20 MW (Contoh)Dokumen94 halamanForm IR Civil Proyek PLTMG MERAUKE-20 MW (Contoh)Ramdan Pramedis SetyaBelum ada peringkat
- Course Structure Course: Bio101 Essentials of Biology, Lab (4 CR) PrerequisiteDokumen2 halamanCourse Structure Course: Bio101 Essentials of Biology, Lab (4 CR) PrerequisiteAaron ChongBelum ada peringkat
- Manual For Adjustment Inventory For: School Students (AISS)Dokumen6 halamanManual For Adjustment Inventory For: School Students (AISS)Priyansh Patel67% (3)
- SAP Query IntroductionDokumen7 halamanSAP Query Introductionkashram2001Belum ada peringkat
- Q4W1 WW Home-Based Task PDFDokumen2 halamanQ4W1 WW Home-Based Task PDFTintin MorjiaBelum ada peringkat