Anda mungkin juga menyukai
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDari EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesPenilaian: 4 dari 5 bintang4/5 (2)
- PharmacologyDokumen7 halamanPharmacologyANNIE SHINE MAGSACAYBelum ada peringkat
- Metoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDokumen9 halamanMetoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDominique RamosBelum ada peringkat
- Metoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDokumen9 halamanMetoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDominique RamosBelum ada peringkat
- DI Query - 3Dokumen5 halamanDI Query - 3uneesolutionsBelum ada peringkat
- Pyrazinamide Summary of Product CharacteristicsDokumen6 halamanPyrazinamide Summary of Product Characteristicservano1969Belum ada peringkat
- AbemaciclibDokumen2 halamanAbemaciclibIna SimacheBelum ada peringkat
- V. Phenothiazines (ALIPHATIC)Dokumen3 halamanV. Phenothiazines (ALIPHATIC)Christine Pialan SalimbagatBelum ada peringkat
- Metoclopramide DiclofenacDokumen7 halamanMetoclopramide DiclofenacRasco, Allen jayBelum ada peringkat
- Drug StuDyDokumen11 halamanDrug StuDyMel SevillaBelum ada peringkat
- PP ObatDokumen7 halamanPP ObatSaifan AbdurrohmanBelum ada peringkat
- Metformin Hydrochloride PDFDokumen4 halamanMetformin Hydrochloride PDFHannaBelum ada peringkat
- Tishk International University: ApixabanDokumen4 halamanTishk International University: ApixabanDyar MzafarBelum ada peringkat
- Resolor 1mg Film-Coated Tablets (SPC) - DrugsDokumen8 halamanResolor 1mg Film-Coated Tablets (SPC) - DrugsDhiren PranamiBelum ada peringkat
- Description:: Assignment On MifepristoneDokumen5 halamanDescription:: Assignment On Mifepristonevenkata samyukthaBelum ada peringkat
- Jurnal Reading InternaDokumen10 halamanJurnal Reading InternaKrishnaBelum ada peringkat
- Aus Pi TargocidDokumen5 halamanAus Pi TargocidAsto Ata InteristiBelum ada peringkat
- Controloc 40: Prescribing InformationDokumen10 halamanControloc 40: Prescribing InformationNavieen RajBelum ada peringkat
- Final Anti TB in SP - SituationDokumen50 halamanFinal Anti TB in SP - SituationAbdul JalilBelum ada peringkat
- Management of Tuberculosis in Special Situations: Prof. Dr. Zafar Hussain IqbalDokumen27 halamanManagement of Tuberculosis in Special Situations: Prof. Dr. Zafar Hussain IqbalFahadKamalBelum ada peringkat
- Myrin P ForteDokumen3 halamanMyrin P ForteJohn Zedric Villanueva ArciagaBelum ada peringkat
- AzithromycinDokumen4 halamanAzithromycinBrittany ClontzBelum ada peringkat
- Banocide and Banocide ForteDokumen10 halamanBanocide and Banocide ForteJosephBelum ada peringkat
- Rovamycin 3868 DR 1256036243912Dokumen6 halamanRovamycin 3868 DR 1256036243912Ahmed El AlfyBelum ada peringkat
- Keto LogDokumen7 halamanKeto LogKim Justin InfantadoBelum ada peringkat
- CyclosporineDokumen25 halamanCyclosporineraki9999Belum ada peringkat
- Adult: IV Nosocomial Pneumonia Empiric Therapy For Febrile Neutropenic Patients 4.5Dokumen3 halamanAdult: IV Nosocomial Pneumonia Empiric Therapy For Febrile Neutropenic Patients 4.5Chris Denver BancaleBelum ada peringkat
- Summary of Product CharacteristicsDokumen9 halamanSummary of Product Characteristicsddandan_2Belum ada peringkat
- Metoclopramide HCL Metoclopramide Inj 10mg-2ml IreDokumen7 halamanMetoclopramide HCL Metoclopramide Inj 10mg-2ml IresiripBelum ada peringkat
- Colchicine DosageDokumen6 halamanColchicine DosageHam SotheaBelum ada peringkat
- Treatment of Tuberculosis .2Dokumen59 halamanTreatment of Tuberculosis .2Alexander Santiago Parel0% (1)
- Plazomicin - Drug Information - UpToDateDokumen13 halamanPlazomicin - Drug Information - UpToDateMarius PapuricaBelum ada peringkat
- Name of The Medicinal ProductDokumen16 halamanName of The Medicinal Productddandan_2Belum ada peringkat
- Management of Severe Ulcerative Colitis: DR - Siddharth SinghDokumen21 halamanManagement of Severe Ulcerative Colitis: DR - Siddharth SinghLohith VakacherlaBelum ada peringkat
- Fixcom 4® (Tab) : Natrapharm Natrapharm Anti-TB AgentsDokumen13 halamanFixcom 4® (Tab) : Natrapharm Natrapharm Anti-TB AgentsApril_Jane_Nat_8299Belum ada peringkat
- Drug Study CompilationDokumen9 halamanDrug Study CompilationRene John FranciscoBelum ada peringkat
- Drug CardsDokumen3 halamanDrug CardsDave HillBelum ada peringkat
- Lamivudine: in Vitro Studies Indicate That Zidovudine-Resistant Virus Isolates Can Become ZidovudineDokumen7 halamanLamivudine: in Vitro Studies Indicate That Zidovudine-Resistant Virus Isolates Can Become ZidovudineKirtikrushna Suresh Prasad OjhaBelum ada peringkat
- Treatment: Chapter 67: TuberculosisDokumen3 halamanTreatment: Chapter 67: TuberculosisNina MarlinaBelum ada peringkat
- PRIMAQUINE PHOSPHATE-primaquine Phos Phate Tablet Bays Hore Pharmaceuticals, LLCDokumen8 halamanPRIMAQUINE PHOSPHATE-primaquine Phos Phate Tablet Bays Hore Pharmaceuticals, LLCKulfi BarfiBelum ada peringkat
- TDM: Cyclosporin: Course: Advanced Clinical Pharmacy Corse No 711-T Course Incharge: Saima Saleem (Assistant Professor)Dokumen11 halamanTDM: Cyclosporin: Course: Advanced Clinical Pharmacy Corse No 711-T Course Incharge: Saima Saleem (Assistant Professor)Samra KhanBelum ada peringkat
- Drug StudyDokumen15 halamanDrug StudyLene Derlene Gerona100% (2)
- Drug Study On Mesalamine MercaptopurineDokumen15 halamanDrug Study On Mesalamine Mercaptopurineسوما الشمريBelum ada peringkat
- Cancer Cell-Specific AgentsDokumen5 halamanCancer Cell-Specific AgentsRomwella May AlgoBelum ada peringkat
- Primaquine: Phosphate Tablets, UspDokumen6 halamanPrimaquine: Phosphate Tablets, UspEphenk PunkBelum ada peringkat
- Drug Study Ko ToDokumen4 halamanDrug Study Ko ToGian Carlo FernandezBelum ada peringkat
- Therapeutic:: Brand Name: PLASIL ClassificationsDokumen5 halamanTherapeutic:: Brand Name: PLASIL ClassificationsAbby MontealegreBelum ada peringkat
- METFORMINDokumen4 halamanMETFORMINkhesler BacallaBelum ada peringkat
- Core Safety ProfileDokumen6 halamanCore Safety ProfilexepayahBelum ada peringkat
- Antidiarrhoeal DrugsDokumen15 halamanAntidiarrhoeal DrugsJyoti SidhuBelum ada peringkat
- DS Fenofibrate Osteo ARLEDDokumen9 halamanDS Fenofibrate Osteo ARLEDvivi's eyebrowsBelum ada peringkat
- LINEZOLID MonographDokumen3 halamanLINEZOLID Monographfayrouz fathiBelum ada peringkat
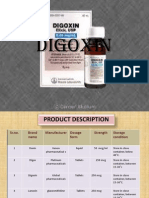
- DigoxinDokumen20 halamanDigoxinAbdulRehmanChaudaryBelum ada peringkat
- TB Drugs (RIPE)Dokumen7 halamanTB Drugs (RIPE)JoharaBelum ada peringkat
- Pharmacological Properties of Pyrazinamide, (Streptomycin)Dokumen14 halamanPharmacological Properties of Pyrazinamide, (Streptomycin)Roland Ma'arif PangestuBelum ada peringkat
- Drug StudyDokumen8 halamanDrug StudyLea FestejoBelum ada peringkat
- Name Mucosta Tablets 100 Description PDFDokumen7 halamanName Mucosta Tablets 100 Description PDFnanda RaharjaBelum ada peringkat
- Kanamycin (Mode of Administration)Dokumen3 halamanKanamycin (Mode of Administration)Waseem MaroofiBelum ada peringkat
- Mot Ilium TabDokumen11 halamanMot Ilium TabChandra FatmaBelum ada peringkat
- Pcol2 CrossDokumen1 halamanPcol2 CrossRaya Ibarra LumogdangBelum ada peringkat
- States of Matter NotesDokumen8 halamanStates of Matter NotesRaya Ibarra LumogdangBelum ada peringkat
- Hard Copy Sublingual FinalDokumen7 halamanHard Copy Sublingual FinalRaya Ibarra LumogdangBelum ada peringkat
- Organizational Chart of Quality Control LaboratoryDokumen1 halamanOrganizational Chart of Quality Control LaboratoryRaya Ibarra Lumogdang100% (1)
- Tablet PuzzleDokumen3 halamanTablet PuzzleRaya Ibarra LumogdangBelum ada peringkat
- ToxiiiiiiDokumen6 halamanToxiiiiiiRaya Ibarra LumogdangBelum ada peringkat
- Toxi Prelim To Finals 1Dokumen7 halamanToxi Prelim To Finals 1Raya Ibarra LumogdangBelum ada peringkat
- PLAN1Dokumen3 halamanPLAN1Raya Ibarra LumogdangBelum ada peringkat
- Carbon Disulfide: Sulfocyanate Test Lead Acetate TestDokumen1 halamanCarbon Disulfide: Sulfocyanate Test Lead Acetate TestRaya Ibarra LumogdangBelum ada peringkat
- A.M. P.M. Number Of: Name & Signature of Pharmacists-in-ChargeDokumen4 halamanA.M. P.M. Number Of: Name & Signature of Pharmacists-in-ChargeRaya Ibarra LumogdangBelum ada peringkat
- Lab Report Act 6Dokumen6 halamanLab Report Act 6Raya Ibarra LumogdangBelum ada peringkat
- Experiment 6 9 (Docu)Dokumen1 halamanExperiment 6 9 (Docu)Raya Ibarra LumogdangBelum ada peringkat
- Spiral Wound GasketsDokumen7 halamanSpiral Wound GasketssadatBelum ada peringkat
- Chapter 1 - Introduction To Well Planning & Design PDFDokumen47 halamanChapter 1 - Introduction To Well Planning & Design PDFAkrem Hkimi100% (5)
- Shades Eq Gloss Large Shade ChartDokumen2 halamanShades Eq Gloss Large Shade ChartmeganBelum ada peringkat
- Ajax Disinfectant CleanserDokumen11 halamanAjax Disinfectant CleanserMateusPauloBelum ada peringkat
- Kami Export - Hanna Huff - Amoeba Sisters - DNA Vs RNA 1Dokumen1 halamanKami Export - Hanna Huff - Amoeba Sisters - DNA Vs RNA 1hannakhuffBelum ada peringkat
- Borehole ProblemsDokumen10 halamanBorehole ProblemsMuh Andika Pratama WarisBelum ada peringkat
- Potato Battery ExperimentDokumen4 halamanPotato Battery Experimentvincent cuaBelum ada peringkat
- tmp12B1 TMPDokumen29 halamantmp12B1 TMPFrontiersBelum ada peringkat
- 2018 10 08 ICSG Factbook Copper 2018Dokumen66 halaman2018 10 08 ICSG Factbook Copper 2018treBelum ada peringkat
- 3075-Article Text-9088-1-10-20201218Dokumen11 halaman3075-Article Text-9088-1-10-20201218Rasdawati RasulBelum ada peringkat
- MetalCoat 470 480 Brochure enDokumen9 halamanMetalCoat 470 480 Brochure endanceBelum ada peringkat
- Jurnal International AmilumDokumen17 halamanJurnal International AmilumGhiyatsKalukuBelum ada peringkat
- Database of Embodied Energy and Water Values For MaterialsDokumen3 halamanDatabase of Embodied Energy and Water Values For MaterialsMax Yanac TelleriaBelum ada peringkat
- Biodentine IFUDokumen2 halamanBiodentine IFUbabbalaBelum ada peringkat
- Anatomi Dan Fisiologi Tumbuhan: Ihsan Tria Pramanda, M.SDokumen19 halamanAnatomi Dan Fisiologi Tumbuhan: Ihsan Tria Pramanda, M.SReva RahmafitriBelum ada peringkat
- Medidor Caudal Kobold Flotador UrkDokumen4 halamanMedidor Caudal Kobold Flotador UrkBase SistemasBelum ada peringkat
- Effect of Flake Ice On Concrete CoolingDokumen1 halamanEffect of Flake Ice On Concrete CoolingGianni TogniBelum ada peringkat
- Thesis EnvironmentDokumen66 halamanThesis EnvironmentSorathBelum ada peringkat
- MorphologyDokumen5 halamanMorphologyJimi LeeBelum ada peringkat
- Solid-State Kinetic ModelsDokumen14 halamanSolid-State Kinetic Modelsleizar_death64Belum ada peringkat
- To Achieve 100% 3D Printing Reliability: Our Easy Cheat SheetDokumen7 halamanTo Achieve 100% 3D Printing Reliability: Our Easy Cheat Sheetfeere feeer0% (1)
- Galvaspan G450Dokumen2 halamanGalvaspan G450khurshedlakhoBelum ada peringkat
- Sofw Thickening AgentsDokumen8 halamanSofw Thickening AgentsPulbere NeagraBelum ada peringkat
- Chemical Basis of LifeDokumen5 halamanChemical Basis of LifeCaithlyn KirthleyBelum ada peringkat
- WasherDokumen80 halamanWasherbugdapugBelum ada peringkat
- 2023 Microalgae Application To Bone Repairing Process - A ReviewDokumen19 halaman2023 Microalgae Application To Bone Repairing Process - A ReviewvirgiparedesBelum ada peringkat
- Cummins SB 4022060-Oil Analysis Techniques For High Horsepower Diesel Engines-UpdateDokumen34 halamanCummins SB 4022060-Oil Analysis Techniques For High Horsepower Diesel Engines-Updategilar herliana putraBelum ada peringkat
- Polyglykol Declaration On Correlations Between PH - Eur. or USP-NF and Clariant Methods (Version 01 - 2018)Dokumen5 halamanPolyglykol Declaration On Correlations Between PH - Eur. or USP-NF and Clariant Methods (Version 01 - 2018)verpacking pimBelum ada peringkat
- Deepwater DrillingDokumen54 halamanDeepwater DrillingQuag MireBelum ada peringkat