Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hi Tracy: Total Due Here's Your Bill For JanuaryDokumen6 halamanHi Tracy: Total Due Here's Your Bill For JanuaryalexBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- MMS-TRG-OP-02F3 Narrative ReportDokumen14 halamanMMS-TRG-OP-02F3 Narrative ReportCh Ma100% (1)
- Management of Renal DiseasesDokumen57 halamanManagement of Renal DiseasesAyana KeikoBelum ada peringkat
- When Not To Stop A Clinical Trial.23490736Dokumen4 halamanWhen Not To Stop A Clinical Trial.23490736Gloria KartikaBelum ada peringkat
- Survival Analysis, Part 3: Cox Regression: Statistics and Research DesignDokumen2 halamanSurvival Analysis, Part 3: Cox Regression: Statistics and Research DesignGloria KartikaBelum ada peringkat
- Prevalensi Ventricular HypertrophyDokumen8 halamanPrevalensi Ventricular HypertrophyGloria KartikaBelum ada peringkat
- 24 Newsletter Hypertension and ArrhythmiaDokumen2 halaman24 Newsletter Hypertension and ArrhythmiaGloria KartikaBelum ada peringkat
- Contoh Surat SponsorDokumen1 halamanContoh Surat SponsorGloria KartikaBelum ada peringkat
- QTinterval Changes During The Management of DHFDokumen7 halamanQTinterval Changes During The Management of DHFGloria KartikaBelum ada peringkat
- MC GowanDokumen13 halamanMC GowanGloria KartikaBelum ada peringkat
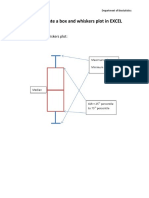
- How To Create A Box and Whiskers Plot in EXCELDokumen9 halamanHow To Create A Box and Whiskers Plot in EXCELGloria KartikaBelum ada peringkat
- Insertion of An Intra-Aortic Balloon Catheter: PurposeDokumen4 halamanInsertion of An Intra-Aortic Balloon Catheter: PurposeGloria KartikaBelum ada peringkat
- 6.21.10 Rose-Jones Board ReviewDokumen50 halaman6.21.10 Rose-Jones Board ReviewGloria KartikaBelum ada peringkat
- WHO LadderDokumen2 halamanWHO LaddertelorkodokBelum ada peringkat
- CLN 66 01 107 PDFDokumen5 halamanCLN 66 01 107 PDFGloria KartikaBelum ada peringkat
- WHO Blindness Action An 2014-2019Dokumen28 halamanWHO Blindness Action An 2014-2019Gloria KartikaBelum ada peringkat
- Vision2020 ReportDokumen97 halamanVision2020 ReportAdelaida Castro NavarreteBelum ada peringkat
- Degeneratif Copy 2Dokumen7 halamanDegeneratif Copy 2Gloria KartikaBelum ada peringkat
- Clinical Management 07Dokumen22 halamanClinical Management 07Fauzi SatriaBelum ada peringkat
- WHO Clinical Management 0f Avian InfluenzaDokumen83 halamanWHO Clinical Management 0f Avian InfluenzaGloria KartikaBelum ada peringkat
- Infeksi Marginalis NadaDokumen48 halamanInfeksi Marginalis NadaGloria KartikaBelum ada peringkat
- Staining and Tooth DiscolorationDokumen14 halamanStaining and Tooth DiscolorationGloria KartikaBelum ada peringkat
- CH 06Dokumen11 halamanCH 06kavitasibalBelum ada peringkat
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Dokumen17 halamanKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaBelum ada peringkat
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Dokumen17 halamanKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaBelum ada peringkat
- Hypertension: H.) or May Be Associated With Other Diseases - Dorland'sDokumen1 halamanHypertension: H.) or May Be Associated With Other Diseases - Dorland'sGloria KartikaBelum ada peringkat
- Lesson 3 Lymphatic System and Body DefensesDokumen10 halamanLesson 3 Lymphatic System and Body DefensesJulio De GuzmanBelum ada peringkat
- Volatility Clustering, Leverage Effects and Risk-Return Trade-Off in The Nigerian Stock MarketDokumen14 halamanVolatility Clustering, Leverage Effects and Risk-Return Trade-Off in The Nigerian Stock MarketrehanbtariqBelum ada peringkat
- Direct InstructionDokumen1 halamanDirect Instructionapi-189549713Belum ada peringkat
- Review Activity For The Final Test - 6 Level: 1. Match Phrasal Verbs and Match To The MeaningDokumen3 halamanReview Activity For The Final Test - 6 Level: 1. Match Phrasal Verbs and Match To The MeaningGabrielle CostaBelum ada peringkat
- Journal Entry DiscussionDokumen8 halamanJournal Entry DiscussionAyesha Eunice SalvaleonBelum ada peringkat
- Ava Gardner Biography StructureDokumen5 halamanAva Gardner Biography Structuredanishfiverr182Belum ada peringkat
- Siege by Roxane Orgill Chapter SamplerDokumen28 halamanSiege by Roxane Orgill Chapter SamplerCandlewick PressBelum ada peringkat
- Life Stories and Travel UnitDokumen3 halamanLife Stories and Travel UnitSamuel MatsinheBelum ada peringkat
- Aaps Pronouns-ExplainedDokumen2 halamanAaps Pronouns-Explainedapi-277377140Belum ada peringkat
- Chrome Settings For CameraDokumen6 halamanChrome Settings For CameraDeep BhanushaliBelum ada peringkat
- Unit-2 Fourier Series & Integral: 2130002 - Advanced Engineering MathematicsDokumen143 halamanUnit-2 Fourier Series & Integral: 2130002 - Advanced Engineering MathematicsDarji DhrutiBelum ada peringkat
- Ward A. Thompson v. City of Lawrence, Kansas Ron Olin, Chief of Police Jerry Wells, District Attorney Frank Diehl, David Davis, Kevin Harmon, Mike Hall, Ray Urbanek, Jim Miller, Bob Williams, Craig Shanks, John Lewis, Jack Cross, Catherine Kelley, Dan Ward, James Haller, Dave Hubbell and Matilda Woody, Frances S. Wisdom v. City of Lawrence, Kansas Ron Olin, Chief of Police David Davis, Mike Hall, Jim Miller, Bob Williams, Craig Shanks, John L. Lewis, Jack Cross, Kevin Harmon, Catherine Kelley, Dan Ward and James Haller, Jr., 58 F.3d 1511, 10th Cir. (1995)Dokumen8 halamanWard A. Thompson v. City of Lawrence, Kansas Ron Olin, Chief of Police Jerry Wells, District Attorney Frank Diehl, David Davis, Kevin Harmon, Mike Hall, Ray Urbanek, Jim Miller, Bob Williams, Craig Shanks, John Lewis, Jack Cross, Catherine Kelley, Dan Ward, James Haller, Dave Hubbell and Matilda Woody, Frances S. Wisdom v. City of Lawrence, Kansas Ron Olin, Chief of Police David Davis, Mike Hall, Jim Miller, Bob Williams, Craig Shanks, John L. Lewis, Jack Cross, Kevin Harmon, Catherine Kelley, Dan Ward and James Haller, Jr., 58 F.3d 1511, 10th Cir. (1995)Scribd Government DocsBelum ada peringkat
- TarotDokumen21 halamanTarotKrystal Jacquot100% (2)
- Impact of Agile On IT and BusinessDokumen6 halamanImpact of Agile On IT and BusinessPurva RaneBelum ada peringkat
- Cub Cadet 1650 PDFDokumen46 halamanCub Cadet 1650 PDFkbrckac33% (3)
- Doña PerfectaDokumen317 halamanDoña PerfectadracbullBelum ada peringkat
- Wave of WisdomDokumen104 halamanWave of WisdomRasika Kesava100% (1)
- Affect of CRM-SCM Integration in Retail IndustryDokumen8 halamanAffect of CRM-SCM Integration in Retail IndustryRajeev ChinnappaBelum ada peringkat
- Global Finance - Introduction ADokumen268 halamanGlobal Finance - Introduction AfirebirdshockwaveBelum ada peringkat
- Times Leader 04-10-2013Dokumen37 halamanTimes Leader 04-10-2013The Times LeaderBelum ada peringkat
- HDFDJH 5Dokumen7 halamanHDFDJH 5balamuruganBelum ada peringkat
- Full Download Test Bank For Macroeconomics 11th Edition Arnold PDF Full ChapterDokumen36 halamanFull Download Test Bank For Macroeconomics 11th Edition Arnold PDF Full Chaptervitalizefoothook.x05r100% (17)
- Boston Consulting Group Portfolio Analysis MatrixDokumen16 halamanBoston Consulting Group Portfolio Analysis MatrixNimish SharmaBelum ada peringkat
- Introduction To Mass Communication Solved MCQs (Set-3)Dokumen5 halamanIntroduction To Mass Communication Solved MCQs (Set-3)Abdul karim MagsiBelum ada peringkat
- History of LotteryDokumen29 halamanHistory of LotteryBala G100% (2)
- GRADE 8 English Lesson on Indian LiteratureDokumen3 halamanGRADE 8 English Lesson on Indian LiteratureErold TarvinaBelum ada peringkat
- Toyota TPMDokumen23 halamanToyota TPMchteo1976Belum ada peringkat