Anda mungkin juga menyukai
- HSS - Summer 2020 - Syllabus - ANTH 1667Dokumen7 halamanHSS - Summer 2020 - Syllabus - ANTH 1667Bruce JobseBelum ada peringkat
- A Year of Blessings: Regina Coeli ReportDokumen12 halamanA Year of Blessings: Regina Coeli ReportBruce JobseBelum ada peringkat
- HSS - Summer 2020 - Syllabus - ANTH 1667Dokumen7 halamanHSS - Summer 2020 - Syllabus - ANTH 1667Bruce JobseBelum ada peringkat
- RPO0100b 25Dokumen130 halamanRPO0100b 25Bruce JobseBelum ada peringkat
- Metal Gods: Dominic Covey Chris DavisDokumen66 halamanMetal Gods: Dominic Covey Chris DavisBruce JobseBelum ada peringkat
- Fuel Cell Handbook (2000)Dokumen352 halamanFuel Cell Handbook (2000)erhan ünal100% (4)
- Charles Rice: Cover: EditingDokumen11 halamanCharles Rice: Cover: EditingBruce JobseBelum ada peringkat
- Vexilliod Tabloid - 73Dokumen12 halamanVexilliod Tabloid - 73Bruce JobseBelum ada peringkat
- AOSpine Global Spine Journal Vol 7 (1S) 46S-52SDokumen7 halamanAOSpine Global Spine Journal Vol 7 (1S) 46S-52SBruce JobseBelum ada peringkat
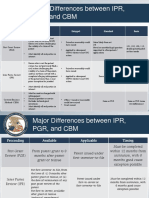
- Major Differences Between IPR, PGR, and CBM: Inter Partes Review (IPR) Petitioner Estoppel Standard BasisDokumen2 halamanMajor Differences Between IPR, PGR, and CBM: Inter Partes Review (IPR) Petitioner Estoppel Standard BasisBruce JobseBelum ada peringkat
- Remington II00 SystemDokumen78 halamanRemington II00 SystemBruce JobseBelum ada peringkat
- C5 Palsy After Cervical Spine Surgery - A Multicenter Retrospective Review of 59 CasesDokumen7 halamanC5 Palsy After Cervical Spine Surgery - A Multicenter Retrospective Review of 59 CasesBruce JobseBelum ada peringkat
- Prevalence and Outcomes in Patients Undergoing Reintubation After Anterior Cervical Spine Surgery - Results From AOSpine North America MultiCenter Study On 8887 PatientsDokumen7 halamanPrevalence and Outcomes in Patients Undergoing Reintubation After Anterior Cervical Spine Surgery - Results From AOSpine North America MultiCenter Study On 8887 PatientsBruce JobseBelum ada peringkat
- Phoenix Command Panzer WWII Medium TanksDokumen32 halamanPhoenix Command Panzer WWII Medium TanksBruce Jobse100% (1)
- Kan 2019 RDF Events and Nonevetns PDFDokumen14 halamanKan 2019 RDF Events and Nonevetns PDFBruce JobseBelum ada peringkat
- Freeway Warrior 01Dokumen291 halamanFreeway Warrior 01Bruce JobseBelum ada peringkat
- Anterior Cervical Infection - Presentation and Incidience of An Uncommon PostOperative ConditionDokumen5 halamanAnterior Cervical Infection - Presentation and Incidience of An Uncommon PostOperative ConditionBruce JobseBelum ada peringkat
- AOSpine Global Spine Journal Vol 7 (1S) 46S-52SDokumen7 halamanAOSpine Global Spine Journal Vol 7 (1S) 46S-52SBruce JobseBelum ada peringkat
- Firearms Oicw Multipurpose Weapon Us Patent 6250194Dokumen17 halamanFirearms Oicw Multipurpose Weapon Us Patent 6250194jim100abBelum ada peringkat
- Freeway Warrior 03 PDFDokumen323 halamanFreeway Warrior 03 PDFBruce JobseBelum ada peringkat
- Freeway Warrior 02 PDFDokumen301 halamanFreeway Warrior 02 PDFBruce Jobse100% (1)
- Army - tc90 1 - Training For Urban OperationsDokumen149 halamanArmy - tc90 1 - Training For Urban OperationsMeowmix100% (6)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Smart Irrigation System With Lora & Recording of Lora Broadcast Using RTL-SDR Dongle For Spectrum AnalyzationDokumen4 halamanSmart Irrigation System With Lora & Recording of Lora Broadcast Using RTL-SDR Dongle For Spectrum AnalyzationInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Reflecting Surfaces Discussion BibliographyDokumen58 halamanReflecting Surfaces Discussion BibliographyAnanthanarayananBelum ada peringkat
- Multiple Choice Questions Class Viii: GeometryDokumen29 halamanMultiple Choice Questions Class Viii: GeometrySoumitraBagBelum ada peringkat
- Project Notes PackagingDokumen4 halamanProject Notes PackagingAngrej Singh SohalBelum ada peringkat
- Philippines Disaster Response PlanDokumen7 halamanPhilippines Disaster Response PlanJoselle RuizBelum ada peringkat
- Rational design of Nile bargesDokumen8 halamanRational design of Nile bargesjhairBelum ada peringkat
- Find Bridges in a Graph Using DFSDokumen15 halamanFind Bridges in a Graph Using DFSVamshi YadavBelum ada peringkat
- 3D Model of Steam Engine Using Opengl: Indian Institute of Information Technology, AllahabadDokumen18 halaman3D Model of Steam Engine Using Opengl: Indian Institute of Information Technology, AllahabadRAJ JAISWALBelum ada peringkat
- Introduction To Intelligent BuildingsDokumen3 halamanIntroduction To Intelligent Buildingsmamta jainBelum ada peringkat
- Whole Brain Lesson Plan: 3 QuarterDokumen5 halamanWhole Brain Lesson Plan: 3 QuarterNieve Marie Cerezo100% (1)
- Budget Planner Floral Style-A5Dokumen17 halamanBudget Planner Floral Style-A5Santi WidyaninggarBelum ada peringkat
- Shell Rimula R7 AD 5W-30: Performance, Features & Benefits Main ApplicationsDokumen2 halamanShell Rimula R7 AD 5W-30: Performance, Features & Benefits Main ApplicationsAji WibowoBelum ada peringkat
- A.A AntagonismDokumen19 halamanA.A Antagonismjraj030_2k6Belum ada peringkat
- Symbiosis Law School ICE QuestionsDokumen2 halamanSymbiosis Law School ICE QuestionsRidhima PurwarBelum ada peringkat
- Test Initial Engleza A 8a Cu Matrice Si BaremDokumen4 halamanTest Initial Engleza A 8a Cu Matrice Si BaremTatiana BeileșenBelum ada peringkat
- 1888 Speth Ars Quatuor Coronatorum v1Dokumen280 halaman1888 Speth Ars Quatuor Coronatorum v1Paulo Sequeira Rebelo100% (2)
- Value Creation-How-Can-The-Semiconductor-Industry-Keep-Outperforming-FinalDokumen7 halamanValue Creation-How-Can-The-Semiconductor-Industry-Keep-Outperforming-FinalJoão Vitor RibeiroBelum ada peringkat
- Cambridge IGCSE: Pakistan Studies 0448/01Dokumen4 halamanCambridge IGCSE: Pakistan Studies 0448/01Mehmood AlimBelum ada peringkat
- Tthe Sacrament of Reconciliation1Dokumen47 halamanTthe Sacrament of Reconciliation1Rev. Fr. Jessie Somosierra, Jr.Belum ada peringkat
- User Manual: Imagenet Lite™ SoftwareDokumen93 halamanUser Manual: Imagenet Lite™ SoftwareDe Mohamed KaraBelum ada peringkat
- Alice Corporation Pty. Ltd. v. CLS Bank International and CLS Services Ltd.Dokumen4 halamanAlice Corporation Pty. Ltd. v. CLS Bank International and CLS Services Ltd.Rachel PauloseBelum ada peringkat
- Chemistry The Molecular Science 5th Edition Moore Solutions Manual 1Dokumen36 halamanChemistry The Molecular Science 5th Edition Moore Solutions Manual 1josephandersonxqwbynfjzk100% (27)
- Boundless - 5 Steps For High Impact Work ExperienceDokumen3 halamanBoundless - 5 Steps For High Impact Work ExperienceCameron WinnettBelum ada peringkat
- BiOWiSH Crop OverviewDokumen2 halamanBiOWiSH Crop OverviewBrian MassaBelum ada peringkat
- Army National Guard Military Funeral Honors Soldier S Training SOP 23 Nov 15Dokumen203 halamanArmy National Guard Military Funeral Honors Soldier S Training SOP 23 Nov 15LuisAndresBellavista100% (1)
- Amgen Inc. v. F. Hoffmann-LaRoche LTD Et Al - Document No. 423Dokumen19 halamanAmgen Inc. v. F. Hoffmann-LaRoche LTD Et Al - Document No. 423Justia.comBelum ada peringkat
- City of Manila vs. Hon CaridadDokumen2 halamanCity of Manila vs. Hon CaridadkelbingeBelum ada peringkat
- Innovations in Teaching-Learning ProcessDokumen21 halamanInnovations in Teaching-Learning ProcessNova Rhea GarciaBelum ada peringkat
- Quantitative Techniques For Business DecisionsDokumen8 halamanQuantitative Techniques For Business DecisionsArumairaja0% (1)
- Describing A CompanyDokumen3 halamanDescribing A CompanyAfnanBelum ada peringkat