Anda mungkin juga menyukai
- BotulismDokumen6 halamanBotulismMarsiano QendroBelum ada peringkat
- 114149-Article Text-158814-1-10-20190423Dokumen6 halaman114149-Article Text-158814-1-10-20190423biah.volpiiBelum ada peringkat
- Clostridium BotulinumDokumen11 halamanClostridium BotulinumStefy BarranoBelum ada peringkat
- Https:watermark Silverchair Com:41-8-1167Dokumen7 halamanHttps:watermark Silverchair Com:41-8-1167Doni SaragihBelum ada peringkat
- BotulismDokumen29 halamanBotulismRohan TejaBelum ada peringkat
- Emcc - 3Dokumen30 halamanEmcc - 3SomeshBelum ada peringkat
- Botulism PIR 2016Dokumen12 halamanBotulism PIR 2016Nick SzokoBelum ada peringkat
- Botulism - WHODokumen6 halamanBotulism - WHOLembah SunyiBelum ada peringkat
- BAM Chapter 17 - Clostridium Botulinum - FDADokumen27 halamanBAM Chapter 17 - Clostridium Botulinum - FDAclinicosBelum ada peringkat
- BAM Chapter 17. Clostridium BotulinumDokumen26 halamanBAM Chapter 17. Clostridium BotulinumremyBelum ada peringkat
- Risk Assessment Project: Botulism: by Micah KinneyDokumen26 halamanRisk Assessment Project: Botulism: by Micah Kinneyapi-547398649Belum ada peringkat
- Control of Communicable Disease ManualDokumen30 halamanControl of Communicable Disease ManualEl-yes Yonirazer El-Banjary0% (1)
- Veterinary Microbiology: Short CommunicationDokumen5 halamanVeterinary Microbiology: Short CommunicationbmalvareBelum ada peringkat
- BotulismDokumen16 halamanBotulismElena ro alBelum ada peringkat
- Canned Foods and Botulism: January 2014Dokumen4 halamanCanned Foods and Botulism: January 2014febry anggelaBelum ada peringkat
- Botulismo Infantil Comunicacion de Un Caso ClinicoDokumen7 halamanBotulismo Infantil Comunicacion de Un Caso ClinicoBrayan CastilloBelum ada peringkat
- Wa0003.Dokumen18 halamanWa0003.Adrija DasBelum ada peringkat
- Clostridium Botulinum: and BotulismDokumen14 halamanClostridium Botulinum: and BotulismTara smana AmliBelum ada peringkat
- Botulism, My ReviewDokumen19 halamanBotulism, My ReviewAdrija DasBelum ada peringkat
- Botulism EpiDokumen26 halamanBotulism EpiMaria PavlovaBelum ada peringkat
- Botulism, My Review - 213224-11-0023Dokumen18 halamanBotulism, My Review - 213224-11-0023Adrija DasBelum ada peringkat
- Clostridium Botulinum PDFDokumen3 halamanClostridium Botulinum PDFsyazaqilahBelum ada peringkat
- Caso Clínico 4 - Bacilos Gram Positivos - Clostridium BotulinumDokumen6 halamanCaso Clínico 4 - Bacilos Gram Positivos - Clostridium BotulinumGris GuevBelum ada peringkat
- BotulismDokumen5 halamanBotulismsubhash nayakBelum ada peringkat
- BotulismDokumen50 halamanBotulismRenati Venkata SrinathBelum ada peringkat
- BotulismDokumen26 halamanBotulismDiviya ArikrishnanBelum ada peringkat
- Botulism As A Bioterrorism AgentDokumen24 halamanBotulism As A Bioterrorism AgentFabián FernándezBelum ada peringkat
- Rare paralytic illness caused by botulinum toxin from C. botulinum bacteriaDokumen10 halamanRare paralytic illness caused by botulinum toxin from C. botulinum bacteriapranit_saikiaBelum ada peringkat
- Anaerobic Bacteria 9B Jo BabieraDokumen9 halamanAnaerobic Bacteria 9B Jo BabieraJoan BabieraBelum ada peringkat
- Appendix 1: Microbial IntoxicationsDokumen7 halamanAppendix 1: Microbial IntoxicationsZiur IshmaelBelum ada peringkat
- BAM: Clostridium Botulinum: Bacteriological Analytical ManualDokumen28 halamanBAM: Clostridium Botulinum: Bacteriological Analytical ManualCésar Augusto Pérez AguilarBelum ada peringkat
- Assaignment On Clostridium BotulinumDokumen11 halamanAssaignment On Clostridium BotulinumRifath AhmedBelum ada peringkat
- Historical and Current Perspectives On Clostridium Botulinum DiversityDokumen13 halamanHistorical and Current Perspectives On Clostridium Botulinum DiversityKiara K.Belum ada peringkat
- Introduction to Botulism: Causes, Symptoms and TreatmentDokumen18 halamanIntroduction to Botulism: Causes, Symptoms and TreatmentPolinaBelum ada peringkat
- Clostridium - Botulinum.Dokumen26 halamanClostridium - Botulinum.tummalapalli venkateswara rao100% (1)
- Botulism Neurotoxin: Rare but Potentially Life ThreateningDokumen15 halamanBotulism Neurotoxin: Rare but Potentially Life ThreateningPietro BracagliaBelum ada peringkat
- How Spreads? & How To Avoid? (Hüseyinden Al) (NOTION)Dokumen3 halamanHow Spreads? & How To Avoid? (Hüseyinden Al) (NOTION)Hüseyin KocakuşakBelum ada peringkat
- Animals 13 02435 v2Dokumen9 halamanAnimals 13 02435 v2Iggjchthfx JcytxutxutxtjBelum ada peringkat
- Suerbaum ReviewDokumen13 halamanSuerbaum Reviewايمن التوميBelum ada peringkat
- Clostridium Botulinum Neurotoxin Types and SourcesDokumen17 halamanClostridium Botulinum Neurotoxin Types and SourcesJanvi PatelBelum ada peringkat
- Botulism: Causes, Symptoms and TreatmentDokumen16 halamanBotulism: Causes, Symptoms and TreatmentSabari Krishnan B BBelum ada peringkat
- Botulism Is A Serious Illness Caused by The Botulinum ToxinDokumen10 halamanBotulism Is A Serious Illness Caused by The Botulinum ToxinReyBelum ada peringkat
- Causes, Signs and Diagnosis of BotulismDokumen7 halamanCauses, Signs and Diagnosis of BotulismAnonymous DA8iQzBelum ada peringkat
- Birao Sas 13 Microbiology and ParasitologyDokumen9 halamanBirao Sas 13 Microbiology and ParasitologyFrancis Jacob Dejecacion GarcesBelum ada peringkat
- Botulism FinalDokumen4 halamanBotulism FinalUlul Ilmi ArhamBelum ada peringkat
- Foodborne Botulism - Scalfaro2018Dokumen6 halamanFoodborne Botulism - Scalfaro2018david ojBelum ada peringkat
- 4 Infección Neonatal C. DifficileDokumen5 halaman4 Infección Neonatal C. DifficileLuis Astudillo MedinaBelum ada peringkat
- Botulism: Prepared by 2nd Year Student of 13th Group Kozachenko AnastasiaDokumen12 halamanBotulism: Prepared by 2nd Year Student of 13th Group Kozachenko AnastasiaЮхно ЮрийBelum ada peringkat
- Food Borne DiseasesDokumen14 halamanFood Borne DiseasesRoseNavyaBelum ada peringkat
- Brucelosis en Pediatría2018 PDFDokumen5 halamanBrucelosis en Pediatría2018 PDFLuis RaymundoBelum ada peringkat
- Thesis 16 June 2023Dokumen133 halamanThesis 16 June 2023Pushpender SinghBelum ada peringkat
- P RO JE CT: Theme:AntibioticDokumen7 halamanP RO JE CT: Theme:AntibioticFijona KeloBelum ada peringkat
- Epidemiology and Prevention of BotulismDokumen43 halamanEpidemiology and Prevention of BotulismIgnasi Parron BernabeBelum ada peringkat
- Diseases 09 00060Dokumen25 halamanDiseases 09 00060Igor BaltaBelum ada peringkat
- Food Poisoning Caused by Gram Positive Spore Forming BacteriaDokumen3 halamanFood Poisoning Caused by Gram Positive Spore Forming Bacteriahadia yousafBelum ada peringkat
- Botulinum Toxin: B. Zane Horowitz, MD, FACMTDokumen15 halamanBotulinum Toxin: B. Zane Horowitz, MD, FACMTŞükriye AngaBelum ada peringkat
- Biological Warfare Agents: AnthraxDokumen4 halamanBiological Warfare Agents: AnthraxVevin MozaBelum ada peringkat
- International Journal of Pharmacy and Pharmaceutical SciencesDokumen6 halamanInternational Journal of Pharmacy and Pharmaceutical SciencesNurainiManda-MinozBelum ada peringkat
- 10-P Epidem 3 2015-EN3Dokumen7 halaman10-P Epidem 3 2015-EN3rodrigocpnovaisBelum ada peringkat
- Blok 3.1 Minggu 2Dokumen18 halamanBlok 3.1 Minggu 2Amir ShafiqBelum ada peringkat
- Receipt PDFDokumen1 halamanReceipt PDFAmir ShafiqBelum ada peringkat
- Osteoarthritis PathophysiologyDokumen2 halamanOsteoarthritis PathophysiologyJona Suarez70% (10)
- Imperforate HymenDokumen4 halamanImperforate HymenMohammad Zaki Budiman100% (2)
- Undescended TestisDokumen25 halamanUndescended TestisAmir ShafiqBelum ada peringkat
- Academic Sessions 2019-2020Dokumen3 halamanAcademic Sessions 2019-2020atiBelum ada peringkat
- Testicular TorsionDokumen24 halamanTesticular TorsionAmir ShafiqBelum ada peringkat
- Blok 3.1 Minggu 2Dokumen18 halamanBlok 3.1 Minggu 2Amir ShafiqBelum ada peringkat
- Definition of PhimosisDokumen11 halamanDefinition of PhimosisAzizah Hafaz0% (1)
- GlomerulonephritisDokumen20 halamanGlomerulonephritisAmir ShafiqBelum ada peringkat
- Testicular TorsionDokumen24 halamanTesticular TorsionAmir ShafiqBelum ada peringkat
- PATHOPHYSIOLOGY PyelonephritisDokumen1 halamanPATHOPHYSIOLOGY PyelonephritisJane Elizabeth Gonzales Macahia100% (1)
- The Beauty of Malaysia English EssayDokumen2 halamanThe Beauty of Malaysia English EssaySyaf AronzBelum ada peringkat
- Acute GlomerulonephritisDokumen57 halamanAcute GlomerulonephritisAmir ShafiqBelum ada peringkat
- CystitisDokumen2 halamanCystitisMazhar WarisBelum ada peringkat
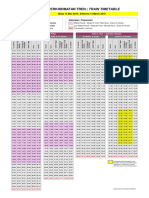
- New KT Schedule 14MAR2018 PDFDokumen1 halamanNew KT Schedule 14MAR2018 PDFWan SyafiqBelum ada peringkat
- CystitisDokumen2 halamanCystitisMazhar WarisBelum ada peringkat
- Imperforate HymenDokumen4 halamanImperforate HymenMohammad Zaki Budiman100% (2)
- Fome - Family Dynamics PDFDokumen21 halamanFome - Family Dynamics PDFfarhanomeBelum ada peringkat
- Testicular TorsionDokumen20 halamanTesticular TorsionGAURAV100% (3)
- Academic Sessions 2018-2019 PDFDokumen3 halamanAcademic Sessions 2018-2019 PDFJohaikal JamaluddinBelum ada peringkat
- Ce 313 Hydraulic Engineering Winter 2013 Instructor: Arturo Leon Ta: Yunji Choi Quiz 1 - Chapter 8 Viscous Flow in Pipes (Part 1) NameDokumen2 halamanCe 313 Hydraulic Engineering Winter 2013 Instructor: Arturo Leon Ta: Yunji Choi Quiz 1 - Chapter 8 Viscous Flow in Pipes (Part 1) NameAmir ShafiqBelum ada peringkat
- ECG Interpretation Guide - Key Components and AbnormalitiesDokumen1 halamanECG Interpretation Guide - Key Components and Abnormalitieshirsi20051879% (24)
- Academic Sessions 2019-2020Dokumen3 halamanAcademic Sessions 2019-2020atiBelum ada peringkat
- Pleno Minggu 6 Blok 3.2Dokumen18 halamanPleno Minggu 6 Blok 3.2Siqbal Karta AsmanaBelum ada peringkat
- Cardiology - ArrhythmiaDokumen18 halamanCardiology - Arrhythmiadrfabianomarins100% (1)
- ArrhythmiaDokumen2 halamanArrhythmiaChris Pritchard93% (30)
- BotulismDokumen6 halamanBotulismAmir ShafiqBelum ada peringkat
- FOME - Opening and Closing SkillsDokumen33 halamanFOME - Opening and Closing Skillsnadhira.daniswaraBelum ada peringkat
- Hirshsprung's DiseaseDokumen4 halamanHirshsprung's DiseaseAmir ShafiqBelum ada peringkat
- Microbiology, Usmle EndpointDokumen208 halamanMicrobiology, Usmle EndpointYazan M Abu-FaraBelum ada peringkat
- A Study of Consumers' Feedback On Street Foods of KolkataDokumen47 halamanA Study of Consumers' Feedback On Street Foods of KolkataSangita JoardarBelum ada peringkat
- U WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDokumen75 halamanU WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDrbee10Belum ada peringkat
- Neurology 2012 MrcppassDokumen154 halamanNeurology 2012 MrcppassRaouf Ra'fat SolimanBelum ada peringkat
- Clostridial Diseases: Tetanus, Botulism, Gas Gangrene and MoreDokumen65 halamanClostridial Diseases: Tetanus, Botulism, Gas Gangrene and MoreGalih Maygananda PutraBelum ada peringkat
- Clostridia: Gas Gangrene, Tetanus, Botulism & Pseudo-Membranous ColitisDokumen11 halamanClostridia: Gas Gangrene, Tetanus, Botulism & Pseudo-Membranous Colitishussain AltaherBelum ada peringkat
- CLOSTRIDIUM TETANI Rashmi 777Dokumen25 halamanCLOSTRIDIUM TETANI Rashmi 777renuBelum ada peringkat
- Lec4 TransDokumen23 halamanLec4 TransErika PatarayBelum ada peringkat
- Quick Start Guide To Feeding Your Super Baby by Ruth Yaron PDFDokumen26 halamanQuick Start Guide To Feeding Your Super Baby by Ruth Yaron PDFsuhaidahBelum ada peringkat
- The G+ve Bacilli of Medical ImportanceDokumen65 halamanThe G+ve Bacilli of Medical ImportanceAbubakr AdilBelum ada peringkat
- Botulinum ToxinDokumen7 halamanBotulinum ToxinAliAyoub100% (2)
- Food Poisoning (Copy)Dokumen6 halamanFood Poisoning (Copy)animesh pandaBelum ada peringkat
- Digestive System Case StudiesDokumen4 halamanDigestive System Case StudiesAndrei CapiliBelum ada peringkat
- Saint Francis of Assisi College: Time: 40 Minutes A. Case Study 1Dokumen2 halamanSaint Francis of Assisi College: Time: 40 Minutes A. Case Study 1Kristine Lyn CamposBelum ada peringkat
- Manual On Fish CanningDokumen78 halamanManual On Fish CanningcaigizaytroiBelum ada peringkat
- Biological Hazards in Food ServiceDokumen24 halamanBiological Hazards in Food Serviceana mejicoBelum ada peringkat
- Whittle K., Howgate P. - Glossary of Fish TechnologyDokumen63 halamanWhittle K., Howgate P. - Glossary of Fish TechnologyResourcesBelum ada peringkat
- Foundations in Microbiology: TalaroDokumen65 halamanFoundations in Microbiology: Talaromertx013Belum ada peringkat
- Blue Book - Guidelines For The Control of Infectious DiseaseDokumen271 halamanBlue Book - Guidelines For The Control of Infectious DiseaseavarathunnyBelum ada peringkat
- Sas 9-14Dokumen8 halamanSas 9-14Bráian Tzéims άλμπαBelum ada peringkat
- Anaerobic InfectionsDokumen36 halamanAnaerobic InfectionsPatriceBelum ada peringkat
- Clostridium - Botulinum.Dokumen26 halamanClostridium - Botulinum.tummalapalli venkateswara rao100% (1)
- The Magic of Honey and It's Many UsesDokumen8 halamanThe Magic of Honey and It's Many UsesSShaBelum ada peringkat
- Antibiotic options for diphtheria and pertussisDokumen22 halamanAntibiotic options for diphtheria and pertussisAseel AliBelum ada peringkat
- Antibiotic, Pesticide, and Microbial Contaminants of Honey Human HealthDokumen10 halamanAntibiotic, Pesticide, and Microbial Contaminants of Honey Human HealthJuan Alejandro JiménezBelum ada peringkat
- Clostridium and Mycobacterium Nursing PresentationDokumen40 halamanClostridium and Mycobacterium Nursing PresentationSAYMABANUBelum ada peringkat
- Field Manual of Wildlife DiseasesDokumen438 halamanField Manual of Wildlife DiseasesMaíra67% (3)
- Clostridial Diseases in Cattle PDFDokumen4 halamanClostridial Diseases in Cattle PDFMuhammad JameelBelum ada peringkat
- April 22, 2015Dokumen14 halamanApril 22, 2015The Delphos HeraldBelum ada peringkat
- Foodborne Botulism, A Case ReportDokumen4 halamanFoodborne Botulism, A Case ReportAri SiswadiBelum ada peringkat