Anda mungkin juga menyukai
- Health Pro Infinity BrochureDokumen5 halamanHealth Pro Infinity BrochureRK0% (1)
- Two Cover Bid SubmissionDokumen40 halamanTwo Cover Bid SubmissionRKBelum ada peringkat
- Axis GroupMedicare E-Brochure (Top-Up)Dokumen4 halamanAxis GroupMedicare E-Brochure (Top-Up)RKBelum ada peringkat
- Insurance Regulatory & Development Authority Act: Module - 5Dokumen12 halamanInsurance Regulatory & Development Authority Act: Module - 5RKBelum ada peringkat
- ETB Super Top Up GMC Mailer - Customer FacingDokumen2 halamanETB Super Top Up GMC Mailer - Customer FacingRKBelum ada peringkat
- Physiomodalities Catlog NewDokumen2 halamanPhysiomodalities Catlog NewRKBelum ada peringkat
- LIC Integrity PactDokumen2 halamanLIC Integrity PactRKBelum ada peringkat
- IRDA Brochure PDFDokumen24 halamanIRDA Brochure PDFRKBelum ada peringkat
- Bankers Indemnity Claim FormDokumen3 halamanBankers Indemnity Claim FormRKBelum ada peringkat
- Jewellers Block Claim FormDokumen3 halamanJewellers Block Claim FormRKBelum ada peringkat
- Kotak Health Premier Claim Form Part BDokumen32 halamanKotak Health Premier Claim Form Part BRKBelum ada peringkat
- SBI Life - EWealth Insurance - Web - 11102018Dokumen17 halamanSBI Life - EWealth Insurance - Web - 11102018RKBelum ada peringkat
- Top Up Re-Application and Transfer of Amount FormDokumen2 halamanTop Up Re-Application and Transfer of Amount FormRKBelum ada peringkat
- Family Medicare Policy-ProspectusDokumen11 halamanFamily Medicare Policy-ProspectusRKBelum ada peringkat
- Kotak Health Super Top Up Proposal Form ClassicDokumen4 halamanKotak Health Super Top Up Proposal Form ClassicRKBelum ada peringkat
- Policy Holder's Manual - Private Car Package: Bajaj Allianz General Insurance Company LTDDokumen33 halamanPolicy Holder's Manual - Private Car Package: Bajaj Allianz General Insurance Company LTDRKBelum ada peringkat
- Kotak Car Secure Brochure 16052018Dokumen4 halamanKotak Car Secure Brochure 16052018RKBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- ADM3346A Midterm Fall 2010 SolutionDokumen10 halamanADM3346A Midterm Fall 2010 SolutionJohn BecksBelum ada peringkat
- Food Safety and StandardsDokumen8 halamanFood Safety and StandardsArifSheriffBelum ada peringkat
- The World Wide WebDokumen22 halamanThe World Wide WebSa JeesBelum ada peringkat
- Corrugated Horn AntennasDokumen4 halamanCorrugated Horn AntennasmiusayBelum ada peringkat
- Oil and Gas Reloaded: Offshore ArgentinaDokumen9 halamanOil and Gas Reloaded: Offshore ArgentinaMuhammad Fahmi AnbBelum ada peringkat
- P102 Lesson 4Dokumen24 halamanP102 Lesson 4Tracy Blair Napa-egBelum ada peringkat
- School MemoDokumen1 halamanSchool MemoBellaBelum ada peringkat
- Singh 1959 Adam Smith's Theory of Economic DevelopmentDokumen27 halamanSingh 1959 Adam Smith's Theory of Economic DevelopmentBruce WayneBelum ada peringkat
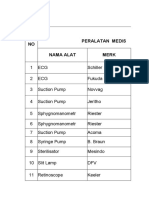
- Daftar Kalibrasi Peralatan MedisDokumen34 halamanDaftar Kalibrasi Peralatan Medisdiklat rssnBelum ada peringkat
- Process and Inter-Process Systems For All Industries.: Cleaning Validation: An Overall PerspectiveDokumen7 halamanProcess and Inter-Process Systems For All Industries.: Cleaning Validation: An Overall PerspectiveDesarrollo de Colecciones IVIC-BMRBelum ada peringkat
- Vol II - PIM (Feasibility Report) For Resort at ChorwadDokumen42 halamanVol II - PIM (Feasibility Report) For Resort at Chorwadmyvin jovi denzilBelum ada peringkat
- COA DBM JOINT CIRCULAR NO 2 s2022 DATED NOVEMBER 10 2022Dokumen2 halamanCOA DBM JOINT CIRCULAR NO 2 s2022 DATED NOVEMBER 10 2022John Christian ReyesBelum ada peringkat
- A Study On Impact of Acne Vulgaris On Quality of LifeDokumen7 halamanA Study On Impact of Acne Vulgaris On Quality of LifeIJAR JOURNALBelum ada peringkat
- Electronics World 1962 11Dokumen114 halamanElectronics World 1962 11meisterwantBelum ada peringkat
- Dungeon Magazine 195 PDFDokumen5 halamanDungeon Magazine 195 PDFGuillaumeRicherBelum ada peringkat
- Design of Posterior Lumbar Interbody Fusion Cages With Various Infill Pattern For 3D Printing ApplicationDokumen7 halamanDesign of Posterior Lumbar Interbody Fusion Cages With Various Infill Pattern For 3D Printing ApplicationdhazliBelum ada peringkat
- HYD CCU: TICKET - ConfirmedDokumen2 halamanHYD CCU: TICKET - ConfirmedRahul ValapadasuBelum ada peringkat
- Tugas-MPSI-P1-P14 - Kelompok 2 - 19.4A.04Dokumen29 halamanTugas-MPSI-P1-P14 - Kelompok 2 - 19.4A.04gilang putraBelum ada peringkat
- Winter 2016 QP3 Spreadsheet QuestionDokumen2 halamanWinter 2016 QP3 Spreadsheet Questioneegeekeek eieoieeBelum ada peringkat
- Blurring Borders Collusion Between Anti-Immigrant Groups and Immigration Enforcement AgentsDokumen9 halamanBlurring Borders Collusion Between Anti-Immigrant Groups and Immigration Enforcement AgentsJill HolslinBelum ada peringkat
- Invoice-1Dokumen2 halamanInvoice-1atipriya choudharyBelum ada peringkat
- Trail Beaver Valley Edition of May 29, 2012 PennywiseDokumen56 halamanTrail Beaver Valley Edition of May 29, 2012 PennywisePennywise PublishingBelum ada peringkat
- Thermo King CG 2000Dokumen155 halamanThermo King CG 2000Connie TaibaBelum ada peringkat
- Moot Problem FinalDokumen2 halamanMoot Problem FinalHimanshi SaraiyaBelum ada peringkat
- Invoice SummaryDokumen2 halamanInvoice SummarymuBelum ada peringkat
- Me Con Compressed Air SystemsDokumen8 halamanMe Con Compressed Air SystemsesvwestBelum ada peringkat
- Technical Writing PDFDokumen129 halamanTechnical Writing PDFKundan Kumar100% (1)
- Mid Semester Question Paper Programming in CDokumen8 halamanMid Semester Question Paper Programming in CbakaBelum ada peringkat
- Pricelist Jan 2023Dokumen7 halamanPricelist Jan 2023Rahmat FadilBelum ada peringkat
- 785 TrucksDokumen7 halaman785 TrucksJavier Pagan TorresBelum ada peringkat