Anda mungkin juga menyukai
- Let's Talk AboutDokumen7 halamanLet's Talk AboutTaco BellBelum ada peringkat
- Julian TinaDokumen4 halamanJulian TinaTaco BellBelum ada peringkat
- I Was Never YoursDokumen7 halamanI Was Never YoursTaco Bell56% (43)
- RevDokumen3 halamanRevTaco BellBelum ada peringkat
- Assessment Nursing Diagnosis Expected Outcome Nursing Implementation Rationale EvaluationDokumen2 halamanAssessment Nursing Diagnosis Expected Outcome Nursing Implementation Rationale EvaluationTaco BellBelum ada peringkat
- Nursing 101Dokumen5 halamanNursing 101Taco BellBelum ada peringkat
- NCM102 (Reviewer)Dokumen15 halamanNCM102 (Reviewer)Taco BellBelum ada peringkat
- GYNECOLOGICALDokumen255 halamanGYNECOLOGICALTaco BellBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Making Up For Lost TimeDokumen8 halamanMaking Up For Lost TimemochimochiBelum ada peringkat
- Activity No. 7.1 BloodDokumen2 halamanActivity No. 7.1 BloodDree SermanBelum ada peringkat
- Tumor of Small IntestineDokumen27 halamanTumor of Small IntestinePRUTHVI RAJ P SBelum ada peringkat
- Circulatory Disturbances PathophysiologyDokumen38 halamanCirculatory Disturbances Pathophysiologyامينو عبدوBelum ada peringkat
- Science 9, LM 2020Dokumen427 halamanScience 9, LM 2020Mira VeranoBelum ada peringkat
- GRAFT VS HOST AND TRANSPLANT INFECTIONDokumen44 halamanGRAFT VS HOST AND TRANSPLANT INFECTIONHasna Mirda AmazanBelum ada peringkat
- Bryan (Encap)Dokumen2 halamanBryan (Encap)bryan ramosBelum ada peringkat
- What living things are made of cells, tissues, organs and systemsDokumen10 halamanWhat living things are made of cells, tissues, organs and systemsRamyRamia ElzantBelum ada peringkat
- Digestive System Label MeDokumen13 halamanDigestive System Label MeMuhammad AdibBelum ada peringkat
- Prelim HPCTDokumen37 halamanPrelim HPCTMariaangela AliscuanoBelum ada peringkat
- Lesson 10 Brain Parts, Processes and FunctionsDokumen19 halamanLesson 10 Brain Parts, Processes and FunctionsAlfredo ModestoBelum ada peringkat
- Antibody Structure and Function PDFDokumen8 halamanAntibody Structure and Function PDFJay JaswaniBelum ada peringkat
- Cellulite Types by Location: Superficial Spaces of the Head and NeckDokumen30 halamanCellulite Types by Location: Superficial Spaces of the Head and NeckLUBelum ada peringkat
- Digestion and AbsorptionDokumen82 halamanDigestion and AbsorptionCoc FanBelum ada peringkat
- 5BBK Lec5 - Other Blood Groups MQA 2019-09-26 08-14-44Dokumen37 halaman5BBK Lec5 - Other Blood Groups MQA 2019-09-26 08-14-44gothai sivapragasamBelum ada peringkat
- Anatomy LE5 Samplex 2017BDokumen6 halamanAnatomy LE5 Samplex 2017BHanako Sasaki AranillaBelum ada peringkat
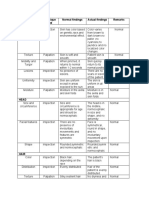
- Area Assessed Technique Used Normal Findings Actual Findings Remarks SkinDokumen6 halamanArea Assessed Technique Used Normal Findings Actual Findings Remarks SkinLadybelle GototosBelum ada peringkat
- Antiphospholipid Syndrome: Causes, Diagnosis and Treatment of Pregnancy ComplicationsDokumen26 halamanAntiphospholipid Syndrome: Causes, Diagnosis and Treatment of Pregnancy ComplicationsDyn AdrianiBelum ada peringkat
- All in One Golden CPSP QuestionsDokumen570 halamanAll in One Golden CPSP QuestionsQuranSunnat100% (2)
- Facial Soft-Tissue Spaces and Retaining Ligaments of The Midcheek - Defining The Premaxillary SpaceDokumen8 halamanFacial Soft-Tissue Spaces and Retaining Ligaments of The Midcheek - Defining The Premaxillary SpaceDaniel CoelhoBelum ada peringkat
- A Sonographic Sign of Moderate ToDokumen5 halamanA Sonographic Sign of Moderate ToDivisi FER MalangBelum ada peringkat
- Exercise Chapter 12Dokumen10 halamanExercise Chapter 12Nurul HusnaBelum ada peringkat
- General Veterinary Macroscopic Anatomy: MYOLOGYDokumen38 halamanGeneral Veterinary Macroscopic Anatomy: MYOLOGYneanna100% (1)
- Immunology Mid-ExamDokumen11 halamanImmunology Mid-ExamNgMinhHaiBelum ada peringkat
- 1) Lecture1Dokumen69 halaman1) Lecture1gurunathnkulkarniBelum ada peringkat
- Neuroanatomy Notes for Neuropsychology ClassDokumen35 halamanNeuroanatomy Notes for Neuropsychology ClassBetsabé VZBelum ada peringkat
- Biology Paper 2 Marking Scheme Asumbi Girls Final Prediction 2022-1Dokumen3 halamanBiology Paper 2 Marking Scheme Asumbi Girls Final Prediction 2022-1balozi training InstituteBelum ada peringkat
- Laryngeal Anatomy and Airway ManagementDokumen15 halamanLaryngeal Anatomy and Airway ManagementMeahgan Renee FeudoBelum ada peringkat
- Digestive System Anatomy and Physiology - NurseslabsDokumen33 halamanDigestive System Anatomy and Physiology - NurseslabsMari FeBelum ada peringkat
- Anatomy and Physiology of the Male and Female Reproductive SystemsDokumen55 halamanAnatomy and Physiology of the Male and Female Reproductive SystemsJeffrey Roy Adlawan LopezBelum ada peringkat