Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Case StudyDokumen3 halamanCase StudyAnqi Liu50% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Pnle ReviewerDokumen293 halamanPnle ReviewerAsniah Hadjiadatu Abdullah94% (18)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Health EDUC Teaching Demo RubricsDokumen4 halamanHealth EDUC Teaching Demo RubricsAsniah Hadjiadatu Abdullah100% (1)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- A Study On Mistakes and Errors in Consecutive Interpretation From Vietnamese To English. Dang Huu Chinh. Qhf.1Dokumen38 halamanA Study On Mistakes and Errors in Consecutive Interpretation From Vietnamese To English. Dang Huu Chinh. Qhf.1Kavic100% (2)
- HR Recruiter Interview Question & AnswerDokumen6 halamanHR Recruiter Interview Question & AnswerGurukrushna PatnaikBelum ada peringkat
- Application Forms (Fillable)Dokumen2 halamanApplication Forms (Fillable)Asniah Hadjiadatu AbdullahBelum ada peringkat
- Daniel Saladas ResumeDokumen2 halamanDaniel Saladas ResumeAsniah Hadjiadatu AbdullahBelum ada peringkat
- CV 2023010319584829Dokumen1 halamanCV 2023010319584829Asniah Hadjiadatu AbdullahBelum ada peringkat
- FNCP PoorsanitationmarwahDokumen3 halamanFNCP PoorsanitationmarwahAsniah Hadjiadatu AbdullahBelum ada peringkat
- To Fill-Up Id-Atm FormDokumen7 halamanTo Fill-Up Id-Atm FormAsniah Hadjiadatu AbdullahBelum ada peringkat
- Credential Verification Form Non-Clinical (Without Signature Page)Dokumen1 halamanCredential Verification Form Non-Clinical (Without Signature Page)Asniah Hadjiadatu AbdullahBelum ada peringkat
- Poor Environmetal Sanitation As Health Threat CuesDokumen11 halamanPoor Environmetal Sanitation As Health Threat CuesAsniah Hadjiadatu AbdullahBelum ada peringkat
- Nursing Notes Maternal and Child Nursing CareDokumen70 halamanNursing Notes Maternal and Child Nursing CareAsniah Hadjiadatu AbdullahBelum ada peringkat
- Family Case Study PresentationDokumen1 halamanFamily Case Study PresentationAsniah Hadjiadatu AbdullahBelum ada peringkat
- Family Case Study On Pulmonary TuberculosisDokumen4 halamanFamily Case Study On Pulmonary TuberculosisAsniah Hadjiadatu AbdullahBelum ada peringkat
- Poor Compliance With Treatment As Health Threat CuesDokumen11 halamanPoor Compliance With Treatment As Health Threat CuesAsniah Hadjiadatu AbdullahBelum ada peringkat
- Health Teaching Plan FinaleDokumen4 halamanHealth Teaching Plan FinaleAsniah Hadjiadatu AbdullahBelum ada peringkat
- Family Case StudyDokumen33 halamanFamily Case StudyAsniah Hadjiadatu AbdullahBelum ada peringkat
- History: Ebolavirus. After This Discovery, Scientists Concluded That The Virus Came From Two DifferentDokumen4 halamanHistory: Ebolavirus. After This Discovery, Scientists Concluded That The Virus Came From Two DifferentAsniah Hadjiadatu AbdullahBelum ada peringkat
- Water RescueDokumen7 halamanWater RescueAsniah Hadjiadatu AbdullahBelum ada peringkat
- Mock ResumeDokumen3 halamanMock ResumeAsniah Hadjiadatu AbdullahBelum ada peringkat
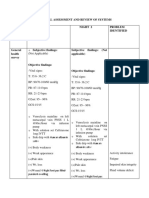
- Physical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedDokumen9 halamanPhysical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedAsniah Hadjiadatu AbdullahBelum ada peringkat
- Or/Dr/Nicu/Pacu Requirements: Open Wound TypesDokumen6 halamanOr/Dr/Nicu/Pacu Requirements: Open Wound TypesAsniah Hadjiadatu AbdullahBelum ada peringkat
- Psychiatric-Mental Health NursingDokumen6 halamanPsychiatric-Mental Health NursingAsniah Hadjiadatu AbdullahBelum ada peringkat
- Concept Map AtekharlssDokumen3 halamanConcept Map AtekharlssAsniah Hadjiadatu AbdullahBelum ada peringkat
- Final Nursing CareplanDokumen7 halamanFinal Nursing CareplanAsniah Hadjiadatu AbdullahBelum ada peringkat
- Proposed Budget For The 17th Striping and Pinning Investiture CeremonyDokumen1 halamanProposed Budget For The 17th Striping and Pinning Investiture CeremonyAsniah Hadjiadatu AbdullahBelum ada peringkat
- Assessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationDokumen11 halamanAssessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationAsniah Hadjiadatu Abdullah100% (1)
- Assessments Nursing Diagnosis Planning Interventions Rationale EvaluationDokumen12 halamanAssessments Nursing Diagnosis Planning Interventions Rationale EvaluationAsniah Hadjiadatu AbdullahBelum ada peringkat
- Rule 107Dokumen8 halamanRule 107AlexBelum ada peringkat
- G12 PR1 AsDokumen34 halamanG12 PR1 Asjaina rose yambao-panerBelum ada peringkat
- Classroom Management PaperDokumen7 halamanClassroom Management PaperdessyutamiBelum ada peringkat
- De Villa vs. Court of AppealsDokumen1 halamanDe Villa vs. Court of AppealsValerie Aileen AnceroBelum ada peringkat
- What Is Art?Dokumen14 halamanWhat Is Art?Sarvenaaz QaffariBelum ada peringkat
- Hoaxes Involving Military IncidentsDokumen5 halamanHoaxes Involving Military IncidentsjtcarlBelum ada peringkat
- Reaction On The 83RD Post Graduate Course On Occupational Health and SafetyDokumen1 halamanReaction On The 83RD Post Graduate Course On Occupational Health and SafetyEdcelle SabanalBelum ada peringkat
- Human Resource Planning in Health CareDokumen3 halamanHuman Resource Planning in Health CarevishalbdsBelum ada peringkat
- Sections 3 7Dokumen20 halamanSections 3 7ninalgamaryroseBelum ada peringkat
- What Is Innovation A ReviewDokumen33 halamanWhat Is Innovation A ReviewAnonymous EnIdJOBelum ada peringkat
- Solution Manual For Management A Focus On Leaders Plus 2014 Mymanagementlab With Pearson Etext Package 2 e Annie MckeeDokumen24 halamanSolution Manual For Management A Focus On Leaders Plus 2014 Mymanagementlab With Pearson Etext Package 2 e Annie MckeeAnnGregoryDDSemcxo100% (90)
- Young Learners Starters Sample Papers 2018 Vol1Dokumen15 halamanYoung Learners Starters Sample Papers 2018 Vol1Natalia García GarcíaBelum ada peringkat
- Unilateral Lower Limb SwellingDokumen1 halamanUnilateral Lower Limb SwellingLilius TangBelum ada peringkat
- List of Festivals in India - WikipediaDokumen13 halamanList of Festivals in India - WikipediaRashmi RaviBelum ada peringkat
- Armor MagazineDokumen56 halamanArmor Magazine"Rufus"100% (2)
- Young Entrepreneurs of IndiaDokumen13 halamanYoung Entrepreneurs of Indiamohit_jain_90Belum ada peringkat
- Stat 201 - Project 1 - Spring 2019: Due Friday, February 8, 2019Dokumen9 halamanStat 201 - Project 1 - Spring 2019: Due Friday, February 8, 2019Bao GanBelum ada peringkat
- 5909 East Kaviland AvenueDokumen1 halaman5909 East Kaviland Avenueapi-309853346Belum ada peringkat
- Jacob Boehme Bibliography 6 August LatestDokumen20 halamanJacob Boehme Bibliography 6 August Latestuli20Belum ada peringkat
- Asher - Bacteria, Inc.Dokumen48 halamanAsher - Bacteria, Inc.Iyemhetep100% (1)
- (Dr. Mariam) NT40103 AssignmentDokumen11 halaman(Dr. Mariam) NT40103 AssignmentAhmad Syamil Muhamad ZinBelum ada peringkat
- Paleontology 1Dokumen6 halamanPaleontology 1Avinash UpadhyayBelum ada peringkat
- Sandra Lippert Law Definitions and CodificationDokumen14 halamanSandra Lippert Law Definitions and CodificationЛукас МаноянBelum ada peringkat
- ABC of Effective WritingDokumen4 halamanABC of Effective Writingprada85Belum ada peringkat
- Explicit and Implicit Grammar Teaching: Prepared By: Josephine Gesim & Jennifer MarcosDokumen17 halamanExplicit and Implicit Grammar Teaching: Prepared By: Josephine Gesim & Jennifer MarcosJosephine GesimBelum ada peringkat
- D78846GC20 sg2Dokumen356 halamanD78846GC20 sg2hilordBelum ada peringkat
- Waterfront Development Goals and ObjectivesDokumen2 halamanWaterfront Development Goals and ObjectivesShruthi Thakkar100% (1)