Anda mungkin juga menyukai
- Psychopathology in Adolescents and Adults with Autism Spectrum DisordersDari EverandPsychopathology in Adolescents and Adults with Autism Spectrum DisordersRoberto KellerBelum ada peringkat
- SexualityDokumen150 halamanSexualityIyalisaiVijay100% (1)
- Intellectual DisabilityDokumen7 halamanIntellectual DisabilityspartanBelum ada peringkat
- Intellectual Disability (MR)Dokumen45 halamanIntellectual Disability (MR)Mobeen JuttBelum ada peringkat
- My Portfolio in Professional Education 4Dokumen25 halamanMy Portfolio in Professional Education 4Jessie PeraltaBelum ada peringkat
- Neurodevelopmental Disorders2023Dokumen62 halamanNeurodevelopmental Disorders2023Chriziel SanchezBelum ada peringkat
- Mental Retardation - Intellectual DisabilityDokumen13 halamanMental Retardation - Intellectual DisabilityMAHIMA DASBelum ada peringkat
- Neurodevelopmental DisordersDokumen2 halamanNeurodevelopmental DisordersDesiree Saldivar BuenoBelum ada peringkat
- Child Development DisorderDokumen75 halamanChild Development DisorderRujuta BaramateBelum ada peringkat
- Intellectual DisabilityDokumen5 halamanIntellectual DisabilityMorthiza EmbongBelum ada peringkat
- Mentally RetardatiomDokumen5 halamanMentally RetardatiomaruntheralBelum ada peringkat
- Chapter 8 Childhood DisordersDokumen6 halamanChapter 8 Childhood DisordersDessirie EnriquezBelum ada peringkat
- Mentally Challenged ChildDokumen13 halamanMentally Challenged ChildUday KumarBelum ada peringkat
- Mentally Challenged ChildDokumen42 halamanMentally Challenged ChildSivabarathy100% (2)
- James Morrison - Chapter 1 and 14Dokumen5 halamanJames Morrison - Chapter 1 and 14Amanda ParrellaBelum ada peringkat
- Introduction To Inclusive EducationDokumen137 halamanIntroduction To Inclusive EducationFeven SolomonBelum ada peringkat
- Unit 3Dokumen32 halamanUnit 32001 PGIMS RohtakBelum ada peringkat
- File 1663148139 0005620 AUTISMDokumen45 halamanFile 1663148139 0005620 AUTISM2022824838.pasangBelum ada peringkat
- Classification and Types of Mental RetardationDokumen2 halamanClassification and Types of Mental RetardationCh. Asad Nisar85% (13)
- ASDDokumen9 halamanASDEmaan AtifBelum ada peringkat
- Eduu 575 Signature Assignment 1Dokumen16 halamanEduu 575 Signature Assignment 1api-609548053Belum ada peringkat
- 1.1 Definitions of Basic Terms (Impairment, Disability and Handicap)Dokumen33 halaman1.1 Definitions of Basic Terms (Impairment, Disability and Handicap)basha100% (1)
- INTELLECTUAL DISABILITY NotesDokumen21 halamanINTELLECTUAL DISABILITY NotesdanieljohnarboledaBelum ada peringkat
- InclusivnessDokumen183 halamanInclusivnessmollalgnBelum ada peringkat
- Intellectual Disability and Communication DisordersDokumen100 halamanIntellectual Disability and Communication DisordersLaverne Mitch Grachelle Sanchez100% (1)
- Bi enDokumen4 halamanBi enBienida PiolloBelum ada peringkat
- Autism Is Characterized by Delays or Abnormal Functioning Before The Age of ThreeDokumen7 halamanAutism Is Characterized by Delays or Abnormal Functioning Before The Age of ThreeCaracel Cabrera SobionoBelum ada peringkat
- Psychological Assessment ReportDokumen66 halamanPsychological Assessment ReportYeshua Marion Dequito DavidBelum ada peringkat
- What Is Mental RetardationDokumen3 halamanWhat Is Mental Retardationpratibha mishraBelum ada peringkat
- Clinical Characteristics of Intellectual Disabilities - Mental Disorders and Disabilities Among Low-Income Children - NCBI BookshelfDokumen6 halamanClinical Characteristics of Intellectual Disabilities - Mental Disorders and Disabilities Among Low-Income Children - NCBI BookshelfArhatya MarsasinaBelum ada peringkat
- Intellectualdisabilityand Languagedisorder: Natasha Marrus,, Lacey HallDokumen16 halamanIntellectualdisabilityand Languagedisorder: Natasha Marrus,, Lacey HallCristinaBelum ada peringkat
- "People-First" Language Message of RespectDokumen10 halaman"People-First" Language Message of RespectPaul VincentBelum ada peringkat
- Child PsychopathologyDokumen11 halamanChild PsychopathologySavleen KaurBelum ada peringkat
- TGBP Session 3 Intellectual Disability CNSP PDFDokumen100 halamanTGBP Session 3 Intellectual Disability CNSP PDFjlpabalan.tasiBelum ada peringkat
- Intellectual Disability With QuizDokumen52 halamanIntellectual Disability With QuizCarla Andrea QuilloBelum ada peringkat
- Lecture 4 - Neurodevelopmental DisordersDokumen12 halamanLecture 4 - Neurodevelopmental DisordersMinahil Rana Shamshad KhanBelum ada peringkat
- Handicapped Children, Acts and Welfare Measure, Phase IIIDokumen45 halamanHandicapped Children, Acts and Welfare Measure, Phase IIIDr. Meghana NarendranBelum ada peringkat
- DummyDokumen40 halamanDummycocksuckerBelum ada peringkat
- Chapter 10Dokumen21 halamanChapter 10algieBelum ada peringkat
- Intelligence (Psychology)Dokumen15 halamanIntelligence (Psychology)iqra kanwalBelum ada peringkat
- Social (Pragmatic) Communication Disorder and AutismDokumen35 halamanSocial (Pragmatic) Communication Disorder and AutismHooria AmerBelum ada peringkat
- Mental Retardation Research Paper TopicsDokumen10 halamanMental Retardation Research Paper Topicsjsllxhbnd100% (1)
- What Categories of Special Children Are Entitled To Special Education Under IDEA?Dokumen15 halamanWhat Categories of Special Children Are Entitled To Special Education Under IDEA?Edrian EleccionBelum ada peringkat
- Mental Health Information For Children: Child PsychiatryDokumen9 halamanMental Health Information For Children: Child Psychiatryedawood2100% (2)
- Disability DefinitionsDokumen25 halamanDisability DefinitionsviaBelum ada peringkat
- Abnormal Psychology Mental Retardation Autism Childhood DisordersDokumen15 halamanAbnormal Psychology Mental Retardation Autism Childhood DisordersAraBelum ada peringkat
- Fsie Compilation of Reports MidtermDokumen8 halamanFsie Compilation of Reports MidtermjmmelanioBelum ada peringkat
- 08) - Assignment of PsychologhDokumen14 halaman08) - Assignment of PsychologhmarchkotBelum ada peringkat
- Autism Spectrum DisorderDokumen17 halamanAutism Spectrum DisorderOlivia Reodique100% (1)
- Children With DisabilityDokumen89 halamanChildren With DisabilityMariakatrinuuhBelum ada peringkat
- Mental RetardationDokumen90 halamanMental Retardationfatima ombalBelum ada peringkat
- Mental Retardation: By: Louwella G. Padasas Bsed-English IiDokumen19 halamanMental Retardation: By: Louwella G. Padasas Bsed-English IiJustine Sican QueBelum ada peringkat
- Dr. I Gusti Ayu Endah Ardjana, SP - KJ (K)Dokumen17 halamanDr. I Gusti Ayu Endah Ardjana, SP - KJ (K)jaish8904Belum ada peringkat
- DocumentDokumen2 halamanDocumentJose BilogBelum ada peringkat
- Intellectual Disabilities ShowDokumen19 halamanIntellectual Disabilities ShowAmy BrownBelum ada peringkat
- Neurodevelopmental DisordersDokumen33 halamanNeurodevelopmental DisordersBrett de GuzmanBelum ada peringkat
- Autism: Autism Diagnosis DSM IV MatchDokumen6 halamanAutism: Autism Diagnosis DSM IV MatchReyhan VivaldyBelum ada peringkat
- IndexDokumen12 halamanIndexletinonsideBelum ada peringkat
- DSM IVDokumen109 halamanDSM IVMaja StjepicBelum ada peringkat
- 7.mental Retardation ModuleDokumen7 halaman7.mental Retardation ModuleJunadrian GenitoBelum ada peringkat
- Karnataka Land Revenue ActDokumen27 halamanKarnataka Land Revenue ActSachin GowdaBelum ada peringkat
- IEP ChecklistDokumen2 halamanIEP ChecklistHolly Jaye RiversBelum ada peringkat
- 17Dokumen35 halaman17Gwen PhamBelum ada peringkat
- Mental Retardation Mental RetardationDokumen2 halamanMental Retardation Mental RetardationMaia Joyce SagerBelum ada peringkat
- Vineland-Ii Review - VelenoDokumen14 halamanVineland-Ii Review - Velenoapi-163017967100% (1)
- Edgerton, R. (1984) Anthropology and Mental Retardation. Research Approaches and OpportunitiesDokumen24 halamanEdgerton, R. (1984) Anthropology and Mental Retardation. Research Approaches and OpportunitiesjuanitoendaraBelum ada peringkat
- Social IntelligenceDokumen18 halamanSocial IntelligenceRose DeppBelum ada peringkat
- SNIE 1012 PDF Rift VDokumen32 halamanSNIE 1012 PDF Rift VUkash sukarmanBelum ada peringkat
- PEDS and ASQ Developmental Screening TestsDokumen10 halamanPEDS and ASQ Developmental Screening TestsSuryani Malik100% (1)
- Case Study Mental RetardationDokumen8 halamanCase Study Mental RetardationElirene IrenBelum ada peringkat
- The Dyslexic Reader 2006 - Issue 41Dokumen32 halamanThe Dyslexic Reader 2006 - Issue 41Davis Dyslexia Association International100% (17)
- Educational Provisions For Learners With Disabilities in IndiaDokumen22 halamanEducational Provisions For Learners With Disabilities in IndiaKishori RaoBelum ada peringkat
- ProjectDokumen7 halamanProject- Serena -Belum ada peringkat
- Emerald Book ChapterDokumen21 halamanEmerald Book ChapterSinduBelum ada peringkat
- Physical Education Unit 4Dokumen15 halamanPhysical Education Unit 4Suhan HaldarBelum ada peringkat
- Disability NotesDokumen71 halamanDisability NotesAkshita BhatBelum ada peringkat
- Etiology of Down Syndrome PDFDokumen2 halamanEtiology of Down Syndrome PDFJoseBelum ada peringkat
- Moving ForwardDokumen293 halamanMoving ForwardHannah JosephBelum ada peringkat
- Human Behavior and VictimologyDokumen85 halamanHuman Behavior and VictimologyJD DBelum ada peringkat
- Foundation of Special and Inclusive EducationDokumen25 halamanFoundation of Special and Inclusive Educationmarjory empredoBelum ada peringkat
- Clc-Student Rights Case Analysis 1Dokumen26 halamanClc-Student Rights Case Analysis 1api-517265222Belum ada peringkat
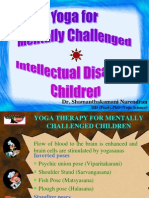
- Dr. Shamanthakamani Narendran: MD (Pead), PHD (Yoga Science)Dokumen31 halamanDr. Shamanthakamani Narendran: MD (Pead), PHD (Yoga Science)jhoo16Belum ada peringkat
- Factors Influencing Personality Development in The Disabled and Their Personality AssessmentDokumen9 halamanFactors Influencing Personality Development in The Disabled and Their Personality Assessmentadheena simon100% (1)
- Developmental Assessment, Warning Signs and Referral PathwaysDokumen33 halamanDevelopmental Assessment, Warning Signs and Referral PathwaysJonathan TayBelum ada peringkat
- Wahl, O. E. (2002) - Children's Views of Mental Illness A Review of the Literature. ν PDFDokumen26 halamanWahl, O. E. (2002) - Children's Views of Mental Illness A Review of the Literature. ν PDFchrissanthiBelum ada peringkat
- Children With Special NeedsDokumen13 halamanChildren With Special NeedsMei-Mei ÜBelum ada peringkat
- Child With Speech DelayDokumen12 halamanChild With Speech DelayJamal100% (1)
- Disability EtiquetteDokumen56 halamanDisability Etiquetteapi-3705160Belum ada peringkat
- PD No. 603Dokumen4 halamanPD No. 603maria luisa radaBelum ada peringkat
- Exploring Experiences of Advocacy by People With Learning DisabilitiesDokumen224 halamanExploring Experiences of Advocacy by People With Learning Disabilitiesremy788Belum ada peringkat