Anda mungkin juga menyukai
- Appendix LDokumen1 halamanAppendix Lapi-383773980Belum ada peringkat
- Portfolio RubricDokumen1 halamanPortfolio Rubricapi-444163791Belum ada peringkat
- IsbarDokumen3 halamanIsbarapi-384653068Belum ada peringkat
- Community AssessmentDokumen19 halamanCommunity Assessmentapi-384653068Belum ada peringkat
- Bed Number Ten ReflectionDokumen7 halamanBed Number Ten Reflectionapi-384653068Belum ada peringkat
- Salary Issues FinalDokumen10 halamanSalary Issues Finalapi-384653068Belum ada peringkat
- Teaching ProjectDokumen2 halamanTeaching Projectapi-384653068Belum ada peringkat
- Cover LetterDokumen1 halamanCover Letterapi-384653068Belum ada peringkat
- Research Article CritiqueDokumen12 halamanResearch Article Critiqueashley kingBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- AS Geography: Case StudiesDokumen26 halamanAS Geography: Case StudiesBrittany FarrantBelum ada peringkat
- 1020 Final EvaluationDokumen9 halaman1020 Final Evaluationapi-456466614Belum ada peringkat
- Adolescent Symptom InventoryDokumen6 halamanAdolescent Symptom InventoryКонстантин КрахмалевBelum ada peringkat
- Monkeypox FAQDokumen2 halamanMonkeypox FAQMaritza NunezBelum ada peringkat
- Cranial NervesDokumen4 halamanCranial NervesAnonymous t5TDwdBelum ada peringkat
- COMMON HAIR DISORDERS: DIAGNOSTIC TOOLS AND NON-SCARRING CAUSESDokumen14 halamanCOMMON HAIR DISORDERS: DIAGNOSTIC TOOLS AND NON-SCARRING CAUSESkateverdadBelum ada peringkat
- Helping Mothers BreastfeedDokumen23 halamanHelping Mothers Breastfeed.Belum ada peringkat
- Soap 3 Adult Alyssa MatulichDokumen6 halamanSoap 3 Adult Alyssa Matulichapi-456313554Belum ada peringkat
- SIMI - Volume Comunicazioni Orali e PosterDokumen212 halamanSIMI - Volume Comunicazioni Orali e Postermaria wahyuniBelum ada peringkat
- Gram Negative RodsDokumen19 halamanGram Negative RodsAnonymous pc5WTTgMBelum ada peringkat
- Cerebral EdemaDokumen6 halamanCerebral EdemaantonopoulosalBelum ada peringkat
- The Jet Volume 4 Number 4 WebDokumen24 halamanThe Jet Volume 4 Number 4 WebShalendra Prasad JohnnyBelum ada peringkat
- Ceftriaxone: Antibiotic ClassDokumen2 halamanCeftriaxone: Antibiotic ClassTanjung PrabandariBelum ada peringkat
- DXN Products South AfricaDokumen15 halamanDXN Products South AfricadxnhpbBelum ada peringkat
- Smelling: Module 3 - Looking Forward: Reading Text Section C, Your HealthDokumen1 halamanSmelling: Module 3 - Looking Forward: Reading Text Section C, Your HealthAmalia Reyes FuentesBelum ada peringkat
- 08 Chapter 2Dokumen73 halaman08 Chapter 2adi_samBelum ada peringkat
- Renal - Goljan SlidesDokumen29 halamanRenal - Goljan SlidesJoan ChoiBelum ada peringkat
- MeaslesDokumen11 halamanMeaslesMarivic DianoBelum ada peringkat
- Aace Guidelines, Diabetes, DMDokumen66 halamanAace Guidelines, Diabetes, DMChanukya GriddaluruBelum ada peringkat
- AKIN DİL Prepositions-AdverbsDokumen15 halamanAKIN DİL Prepositions-AdverbsSerpil AyBelum ada peringkat
- Development and Validation of The Immune Status Questionnaire (ISQ)Dokumen18 halamanDevelopment and Validation of The Immune Status Questionnaire (ISQ)SPE CommitteeBelum ada peringkat
- Dgca HandbookDokumen45 halamanDgca Handbookhswami20037730Belum ada peringkat
- HerbsDokumen476 halamanHerbsVishnu Ronaldus Narayan100% (1)
- CLINDA DRUG STUDYDokumen6 halamanCLINDA DRUG STUDYMa. Rita Concepcion TungulBelum ada peringkat
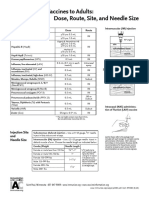
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDokumen1 halamanAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashBelum ada peringkat
- Robert Louis StevensonDokumen3 halamanRobert Louis StevensonjunaidBelum ada peringkat
- Dr. HY Peds Shelf Parts 1 & 2Dokumen22 halamanDr. HY Peds Shelf Parts 1 & 2Emanuella GomezBelum ada peringkat
- BiochemistryDokumen82 halamanBiochemistryAmritzz Paul83% (6)
- Thomas Bowers v. Carolyn Colvin, 4th Cir. (2015)Dokumen10 halamanThomas Bowers v. Carolyn Colvin, 4th Cir. (2015)Scribd Government DocsBelum ada peringkat
- Principle of ElectroDx by Dr. Angkana Nudsasarn, Chiang Mai UniversityDokumen113 halamanPrinciple of ElectroDx by Dr. Angkana Nudsasarn, Chiang Mai UniversitySurat Tanprawate100% (3)