Anda mungkin juga menyukai
- Report - Roche Pharmaceuticals LTD (Human Resource Planning & Development) 222Dokumen23 halamanReport - Roche Pharmaceuticals LTD (Human Resource Planning & Development) 222jawwadraja100% (1)
- Precast Concrete ConstructionDokumen37 halamanPrecast Concrete ConstructionRuta Parekh100% (1)
- La Relación Entre La Postura Del Pie y La Cinemática de Las Extremidades Inferiores Durante LaDokumen10 halamanLa Relación Entre La Postura Del Pie y La Cinemática de Las Extremidades Inferiores Durante LaDayana SánchezBelum ada peringkat
- Normative Values For The Foot PostureDokumen9 halamanNormative Values For The Foot PostureMom of twoBelum ada peringkat
- Foot Orthoses For Adults With Flexible Pes Planus: A Systematic ReviewDokumen18 halamanFoot Orthoses For Adults With Flexible Pes Planus: A Systematic ReviewDonna KrawczykBelum ada peringkat
- Journal of Foot and Ankle Research: Normative Values For The Foot Posture IndexDokumen9 halamanJournal of Foot and Ankle Research: Normative Values For The Foot Posture IndexAnup PednekarBelum ada peringkat
- The Effectiveness of Shoe Insoles For The Prevention and Treatment of Low BackDokumen19 halamanThe Effectiveness of Shoe Insoles For The Prevention and Treatment of Low BackhasBelum ada peringkat
- 31 PDFDokumen4 halaman31 PDFMonalisa MeidaniaBelum ada peringkat
- Differences in Landing and Balance Deficits at The Ankle Joint On Stable and Unstable Surfaces in Inflexible and Flexible Handball PlayersDokumen8 halamanDifferences in Landing and Balance Deficits at The Ankle Joint On Stable and Unstable Surfaces in Inflexible and Flexible Handball PlayersAJHSSR JournalBelum ada peringkat
- Occupational Risk Factors For Osteoarthritis of The Knee: A Meta-AnalysisDokumen11 halamanOccupational Risk Factors For Osteoarthritis of The Knee: A Meta-Analysisfidatahir93Belum ada peringkat
- Journal 10Dokumen29 halamanJournal 10Janet LooBelum ada peringkat
- Quiroprática e Osteopatia 2Dokumen19 halamanQuiroprática e Osteopatia 2Pedro FonsecaBelum ada peringkat
- Hes Sari 2012Dokumen6 halamanHes Sari 2012bbvnrsh279Belum ada peringkat
- The Case For Researching Biomechanics and Human Movement Using A Stochastic Model in A Peer Reviewed Journal To Generate Qualitative EvidenceDokumen3 halamanThe Case For Researching Biomechanics and Human Movement Using A Stochastic Model in A Peer Reviewed Journal To Generate Qualitative Evidencedennis shavelsonBelum ada peringkat
- A Systematic Review and Meta-Analysis of Lower Limb Neuromuscular Alteration Associates With Knee Osteoarthritis During Level WalkingDokumen12 halamanA Systematic Review and Meta-Analysis of Lower Limb Neuromuscular Alteration Associates With Knee Osteoarthritis During Level WalkingItai IzhakBelum ada peringkat
- (2023) Effects of Running On The Development of Knee OsteoarthritisDokumen6 halaman(2023) Effects of Running On The Development of Knee Osteoarthritiscalixto1995Belum ada peringkat
- Plantar FasciitisDokumen23 halamanPlantar FasciitisMoses PaulBelum ada peringkat
- Lee 2018Dokumen7 halamanLee 2018Kings AndrewBelum ada peringkat
- Pone 0074364Dokumen7 halamanPone 0074364Alejandro Patricio Castillo FajardoBelum ada peringkat
- Gulle H. 2023. Prediciting Outcome Plantar Heel Pain. Systematic Review Prognostic FactorsDokumen13 halamanGulle H. 2023. Prediciting Outcome Plantar Heel Pain. Systematic Review Prognostic FactorsJavier MartinBelum ada peringkat
- AbstractDokumen99 halamanAbstracthakishankzBelum ada peringkat
- (15435474 - Journal of Physical Activity and Health) Framework For Physical Activity As A Complex and Multidimensional BehaviorDokumen8 halaman(15435474 - Journal of Physical Activity and Health) Framework For Physical Activity As A Complex and Multidimensional BehaviorarcadetorBelum ada peringkat
- Do Knee Abnormalities Visualised On MRI Explain Knee Pain in Knee OsteoarthritisDokumen9 halamanDo Knee Abnormalities Visualised On MRI Explain Knee Pain in Knee OsteoarthritisRosaneLacerdaBelum ada peringkat
- The Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisDokumen20 halamanThe Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisBruno FellipeBelum ada peringkat
- Framework IntradialisisDokumen8 halamanFramework IntradialisisNovara Qus'nul LuvfiantiBelum ada peringkat
- Conservative Management Following Patellar Dislocation: A Level I Systematic ReviewDokumen10 halamanConservative Management Following Patellar Dislocation: A Level I Systematic ReviewbitaBelum ada peringkat
- Jurnal 1 Ulkus Diabeticus PDFDokumen10 halamanJurnal 1 Ulkus Diabeticus PDFananta restyBelum ada peringkat
- Clinical Outcomes of Rehabilitation For Patients Following Lateral Patellar Dislocation: A Systematic ReviewDokumen13 halamanClinical Outcomes of Rehabilitation For Patients Following Lateral Patellar Dislocation: A Systematic ReviewHarshoi KrishannaBelum ada peringkat
- Arthritis Care Research - 2022 - Lima - How Do Non Surgical Interventions Improve Pain and Physical Function in PeopleDokumen36 halamanArthritis Care Research - 2022 - Lima - How Do Non Surgical Interventions Improve Pain and Physical Function in PeoplerdkelsallBelum ada peringkat
- Sumber Fisis FisioterapiDokumen9 halamanSumber Fisis FisioterapiAndi detty UtamiBelum ada peringkat
- Sexual Activity Before CompetitionDokumen8 halamanSexual Activity Before CompetitionCésar Ayala GuzmánBelum ada peringkat
- Movement Analysis FrameworkDokumen8 halamanMovement Analysis FrameworkSM199021Belum ada peringkat
- Abductor Strenght in Relation With Sports InjuriesDokumen7 halamanAbductor Strenght in Relation With Sports InjuriespetrBelum ada peringkat
- 5854 12393 1 SMDokumen6 halaman5854 12393 1 SMalaa adienBelum ada peringkat
- Peterson 2018Dokumen11 halamanPeterson 2018IndahMardhBelum ada peringkat
- JoelhoDokumen7 halamanJoelhoÉrica SilvaBelum ada peringkat
- Foot and Ankle Questions On The Orthopaedic In-Training Examination: Analysis of Content, Reference, and PerformanceDokumen10 halamanFoot and Ankle Questions On The Orthopaedic In-Training Examination: Analysis of Content, Reference, and PerformanceZia Ur RehmanBelum ada peringkat
- Publication 31Dokumen7 halamanPublication 31Tantia Dewi HariantoBelum ada peringkat
- 10.1007@s10067 020 04988 7Dokumen11 halaman10.1007@s10067 020 04988 7NyLa LibertyBelum ada peringkat
- AF X Fratura Vertebral OsteoporóticaDokumen3 halamanAF X Fratura Vertebral OsteoporóticajaziembowiczBelum ada peringkat
- Body Weight-Supported Gait Training For Restoration of Walking in People With An Incomplete Spinal Cord Injury: A Systematic ReviewDokumen7 halamanBody Weight-Supported Gait Training For Restoration of Walking in People With An Incomplete Spinal Cord Injury: A Systematic ReviewInterSocial LinkBelum ada peringkat
- Callaghan2021 Article ManagementOfPatellofemoralJoinDokumen13 halamanCallaghan2021 Article ManagementOfPatellofemoralJoinNejla Núñez GuevaraBelum ada peringkat
- 28 - Jpts 2015 919Dokumen7 halaman28 - Jpts 2015 919Ikaf FauziahBelum ada peringkat
- Oa KneeDokumen9 halamanOa KneerohanaBelum ada peringkat
- Factors Associated With Patellofemoral Pain Syndrome: A Systematic ReviewDokumen17 halamanFactors Associated With Patellofemoral Pain Syndrome: A Systematic Reviewנתנאל מושקוביץBelum ada peringkat
- RunningDokumen21 halamanRunningHossein NajjarzadeBelum ada peringkat
- 2017 Article 1388Dokumen10 halaman2017 Article 1388MonikaBelum ada peringkat
- Cambios en Dorsiflexión y Control Postural Dinámico Tras Movilizaciones en Individuos Con Inestabilidad Crónica Del TobilloDokumen15 halamanCambios en Dorsiflexión y Control Postural Dinámico Tras Movilizaciones en Individuos Con Inestabilidad Crónica Del Tobillocontact.movementsiteBelum ada peringkat
- 보행패턴2Dokumen24 halaman보행패턴2ahdbrhsjBelum ada peringkat
- Research Article: Gait Patterns in Hemiplegic Patients With Equinus Foot DeformityDokumen8 halamanResearch Article: Gait Patterns in Hemiplegic Patients With Equinus Foot DeformityCamila VargasBelum ada peringkat
- Pathogenic Factors Associated With Osgood-Schlatter Disease in Adolescent Male Soccer PlayersDokumen8 halamanPathogenic Factors Associated With Osgood-Schlatter Disease in Adolescent Male Soccer PlayersBreechesBelum ada peringkat
- Research PaperDokumen10 halamanResearch PaperTaryn BlackstockBelum ada peringkat
- Effects of Attentional Focus On Jump Performance After ACL Reconstruction.Dokumen7 halamanEffects of Attentional Focus On Jump Performance After ACL Reconstruction.Claudia OSBelum ada peringkat
- SiaiDokumen8 halamanSiaimassimo bertoniBelum ada peringkat
- Differences in Gait and Trunk Movement Between Patients After Ankle Fracture and Healthy SubjectsDokumen13 halamanDifferences in Gait and Trunk Movement Between Patients After Ankle Fracture and Healthy SubjectsTerryBelum ada peringkat
- Hospital Therapy Dog Walking For Adolesc Orthopedic LimitationsDokumen17 halamanHospital Therapy Dog Walking For Adolesc Orthopedic LimitationsOnte FelizBelum ada peringkat
- Activity Modification and Knee Strengthening For Osgood-Schlatter DiseaseDokumen9 halamanActivity Modification and Knee Strengthening For Osgood-Schlatter DiseaseSebastian FandiñoBelum ada peringkat
- Functional Electric StimulationDokumen11 halamanFunctional Electric StimulationGustavo CabanasBelum ada peringkat
- Custom Foot Orthoses Improve First-Step Pain in Individuals With Unilateral Plantar Fasciopathy: A Pragmatic Randomised Controlled TrialDokumen11 halamanCustom Foot Orthoses Improve First-Step Pain in Individuals With Unilateral Plantar Fasciopathy: A Pragmatic Randomised Controlled TrialRafael FontesBelum ada peringkat
- Body Weight Changes and Corresponding Changes in Pain and Function in Persons With Symptomatic Knee Osteoarthritis: A Cohort StudyDokumen8 halamanBody Weight Changes and Corresponding Changes in Pain and Function in Persons With Symptomatic Knee Osteoarthritis: A Cohort StudyMiguelBelum ada peringkat
- Sports Hernia and Athletic Pubalgia: Diagnosis and TreatmentDari EverandSports Hernia and Athletic Pubalgia: Diagnosis and TreatmentDavid R. DiduchBelum ada peringkat
- Dakshin Dinajpur TP ListDokumen5 halamanDakshin Dinajpur TP ListDeb D Creative StudioBelum ada peringkat
- Sample Question Paper Computer GraphicsDokumen4 halamanSample Question Paper Computer Graphicsrohit sanjay shindeBelum ada peringkat
- BCO120Dokumen3 halamanBCO120erwin_simsensohnBelum ada peringkat
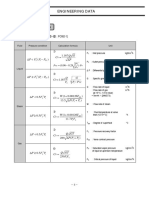
- Engineering Data: 2. CV CalculationDokumen1 halamanEngineering Data: 2. CV Calculationdj22500Belum ada peringkat
- Examples and Non-ExamplesDokumen5 halamanExamples and Non-ExamplesslidegaeBelum ada peringkat
- Werling Optimal Trajectory Generationfor Dynamic Street Scenariosina Frenet FrameDokumen8 halamanWerling Optimal Trajectory Generationfor Dynamic Street Scenariosina Frenet FramehugoBelum ada peringkat
- Pascal LawDokumen17 halamanPascal LawJasmandeep brarBelum ada peringkat
- Adient Managment CSRDokumen68 halamanAdient Managment CSRClaudia PEÑABelum ada peringkat
- Hw1 2 SolutionsDokumen7 halamanHw1 2 SolutionsFrancisco AlvesBelum ada peringkat
- SOS Children's Village: by Bekim RamkuDokumen21 halamanSOS Children's Village: by Bekim RamkuAbdulKerim AyubBelum ada peringkat
- HP RT3000 G2 Toronto UPS SpecsDokumen13 halamanHP RT3000 G2 Toronto UPS SpecsJokBalingitBelum ada peringkat
- PTS Controller: Over Fuel Dispensers and ATG Systems For Petrol StationsDokumen161 halamanPTS Controller: Over Fuel Dispensers and ATG Systems For Petrol StationsdawitBelum ada peringkat
- Belbin's Team ModelDokumen2 halamanBelbin's Team Modelsonu_saisBelum ada peringkat
- UntitledDokumen44 halamanUntitledFrancesco TauroBelum ada peringkat
- 67 - Es - Ut Republic Csalamade BooDokumen47 halaman67 - Es - Ut Republic Csalamade BooTyler LeeBelum ada peringkat
- Data Analaysis and InterpretationDokumen56 halamanData Analaysis and Interpretationporkodisvl100% (2)
- 1 Conformity Asch StudyDokumen31 halaman1 Conformity Asch StudyjasbruBelum ada peringkat
- Acm 003Dokumen5 halamanAcm 003Roan BBelum ada peringkat
- CNSB Bypass Separator Commissioning and Maintenance Guide: Conder® Tanks Covered by This GuideDokumen4 halamanCNSB Bypass Separator Commissioning and Maintenance Guide: Conder® Tanks Covered by This GuidesterlingBelum ada peringkat
- Swot Analysis of Revlon IncDokumen5 halamanSwot Analysis of Revlon IncSubhana AsimBelum ada peringkat
- Tutorial Chapter 2Dokumen5 halamanTutorial Chapter 2Naasir SheekeyeBelum ada peringkat
- Pardoseli PVCDokumen72 halamanPardoseli PVCnasuemilBelum ada peringkat
- Survey 2 Module 2Dokumen76 halamanSurvey 2 Module 2veereshBelum ada peringkat
- 4363 112 Heat TransferDokumen6 halaman4363 112 Heat Transferyogesh_b_kBelum ada peringkat
- Recommendation Letter MhandoDokumen2 halamanRecommendation Letter MhandoAnonymous Xb3zHio0% (1)
- Department of Education: Activity Completion ReportDokumen1 halamanDepartment of Education: Activity Completion ReportJanineJavier100% (1)
- Connecting Your Database and Auto Generate ID Using VB - Net 2008 and MySQL DatabaseDokumen1 halamanConnecting Your Database and Auto Generate ID Using VB - Net 2008 and MySQL DatabaseAgusWibowoBelum ada peringkat