Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Mcob OcDokumen19 halamanMcob OcashisBelum ada peringkat
- Conductivity On Animal SpermDokumen8 halamanConductivity On Animal SpermAndrew AdamsBelum ada peringkat
- Chapter 4Dokumen21 halamanChapter 4Ahmad KhooryBelum ada peringkat
- Discovery Issues Resolution Naga NotesDokumen7 halamanDiscovery Issues Resolution Naga NotesNagaPrasannaKumarKakarlamudi100% (1)
- UntitledDokumen30 halamanUntitledGauravBelum ada peringkat
- Angular With Web ApiDokumen32 halamanAngular With Web ApiAnonymous hTmjRsiCp100% (1)
- Catalogo Molas PratoDokumen176 halamanCatalogo Molas Pratocassio_tecdrawBelum ada peringkat
- Double Helix Revisited PDFDokumen3 halamanDouble Helix Revisited PDFPaulo Teng An SumodjoBelum ada peringkat
- Fun Activities: Dhruv Global School, Pune Holiday Home Assignment NurseryDokumen14 halamanFun Activities: Dhruv Global School, Pune Holiday Home Assignment NurseryChintan JainBelum ada peringkat
- Construction Management Plan TemplateDokumen15 halamanConstruction Management Plan TemplatePrasad Ghorpade100% (2)
- Reflection and Refraction of LightDokumen34 halamanReflection and Refraction of Lightseunnuga93Belum ada peringkat
- Finding The Process Edge: ITIL at Celanese: Ulrike SchultzeDokumen18 halamanFinding The Process Edge: ITIL at Celanese: Ulrike SchultzeCristiane Drebes PedronBelum ada peringkat
- Earthquake EssayDokumen1 halamanEarthquake EssayAnsir Yaqoob100% (1)
- MCVM: Monte Carlo Modeling of Photon Migration in Voxelized MediaDokumen12 halamanMCVM: Monte Carlo Modeling of Photon Migration in Voxelized MediaĐô Lê PhiBelum ada peringkat
- Xaviers Institute of Social Service: Assignment On Quantitative TechniquesDokumen20 halamanXaviers Institute of Social Service: Assignment On Quantitative Techniquesravi kumarBelum ada peringkat
- Dos and DontsDokumen1 halamanDos and DontsLeah GlickBelum ada peringkat
- Reflection EssayDokumen3 halamanReflection Essayapi-451553720Belum ada peringkat
- Siddique, Tashfeen Coverletter 20170320Dokumen1 halamanSiddique, Tashfeen Coverletter 20170320Anonymous liUNtnyBelum ada peringkat
- Job PortalDokumen10 halamanJob PortalNiro ThakurBelum ada peringkat
- 11 Technical Analysis & Dow TheoryDokumen9 halaman11 Technical Analysis & Dow TheoryGulzar AhmedBelum ada peringkat
- PsiRun SheetsDokumen3 halamanPsiRun SheetsalemauBelum ada peringkat
- Mini Test PBD - SpeakingDokumen4 halamanMini Test PBD - Speakinghe shaBelum ada peringkat
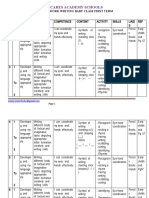
- Scheme of Work Writing Baby First TermDokumen12 halamanScheme of Work Writing Baby First TermEmmy Senior Lucky100% (1)
- OP-COM Fault Codes PrintDokumen2 halamanOP-COM Fault Codes Printtiponatis0% (1)
- DfgtyhDokumen4 halamanDfgtyhAditya MakkarBelum ada peringkat
- Articles of Confederation LessonDokumen2 halamanArticles of Confederation Lessonapi-233755289Belum ada peringkat
- Solution of Linear Systems of Equations in Matlab, Freemat, Octave and Scilab by WWW - Freemat.infoDokumen4 halamanSolution of Linear Systems of Equations in Matlab, Freemat, Octave and Scilab by WWW - Freemat.inforodwellheadBelum ada peringkat
- The Advanced Formula For Total Success - Google Search PDFDokumen2 halamanThe Advanced Formula For Total Success - Google Search PDFsesabcdBelum ada peringkat
- HR Associate - Job Description VFinalDokumen2 halamanHR Associate - Job Description VFinalPamela CardozoBelum ada peringkat
- Case Study Sustainable ConstructionDokumen5 halamanCase Study Sustainable ConstructionpraisethenordBelum ada peringkat