Anda mungkin juga menyukai
- The Gut Microbiota Tumorigenesis and Liver Diseases 2017 EngineeringDokumen5 halamanThe Gut Microbiota Tumorigenesis and Liver Diseases 2017 EngineeringMariaBelum ada peringkat
- Gut Microbiota and Allergic Disease New FindingsDokumen6 halamanGut Microbiota and Allergic Disease New FindingsEva Mayte GuadarramaBelum ada peringkat
- Enter o ColitisDokumen18 halamanEnter o ColitisAinil MardiahBelum ada peringkat
- The Microbiome in Early Life: Implications For Health OutcomesDokumen10 halamanThe Microbiome in Early Life: Implications For Health Outcomesngonzalezduran5920Belum ada peringkat
- Intricate Connections Between The Microbiota and EndometriosisDokumen23 halamanIntricate Connections Between The Microbiota and EndometriosiskannalijayaBelum ada peringkat
- Ijms 24 13507Dokumen15 halamanIjms 24 13507Kikin RizkynnisaBelum ada peringkat
- Human Microbiome Journal: Emmanouil Angelakis, Didier RaoultDokumen5 halamanHuman Microbiome Journal: Emmanouil Angelakis, Didier RaoultAndy SetiawanBelum ada peringkat
- Cancer and the Gut Microbiota LinkDokumen10 halamanCancer and the Gut Microbiota LinkEmilio AlaquàsBelum ada peringkat
- 1-S2.0-S0009898115000170-Main Microbiomul Si Sanatatea Adultului PDFDokumen6 halaman1-S2.0-S0009898115000170-Main Microbiomul Si Sanatatea Adultului PDFLUTICHIEVICI NATALIABelum ada peringkat
- Diseases 09 00060Dokumen25 halamanDiseases 09 00060Igor BaltaBelum ada peringkat
- Probiotics and Prebiotics - Role in Prevention of Nosocomial Sepsis in Preterm InfantsDokumen9 halamanProbiotics and Prebiotics - Role in Prevention of Nosocomial Sepsis in Preterm InfantsHyacinth RotaBelum ada peringkat
- Ibd GDDokumen15 halamanIbd GDAndi SusiloBelum ada peringkat
- Bio ProjectDokumen27 halamanBio ProjectAman ghoshBelum ada peringkat
- Exercise Diet and Stress As Modulators of Gut Microbiota - 2020 - NeurobiologyDokumen16 halamanExercise Diet and Stress As Modulators of Gut Microbiota - 2020 - NeurobiologySabrina YenBelum ada peringkat
- Appropriate Use of Antibiotics in The NICUDokumen6 halamanAppropriate Use of Antibiotics in The NICUmoniaBelum ada peringkat
- 2018 Article 1326Dokumen8 halaman2018 Article 1326Mohammad Ziaul KarimBelum ada peringkat
- Early Life Experience and Gut Microbiome: The Brain-Gut - Microbiota Signaling SystemDokumen17 halamanEarly Life Experience and Gut Microbiome: The Brain-Gut - Microbiota Signaling SystemLaura MarttilaBelum ada peringkat
- 1 s2.0 S1323893022000120 MainDokumen9 halaman1 s2.0 S1323893022000120 MainValeria BoomBelum ada peringkat
- Artigo 08 - Fimmu-12-683022Dokumen22 halamanArtigo 08 - Fimmu-12-683022Pedro AfonsoBelum ada peringkat
- The Roles of Inflammation, Nutrient Availability and The Commensal Microbiota in Enteric Pathogen Infection.Dokumen17 halamanThe Roles of Inflammation, Nutrient Availability and The Commensal Microbiota in Enteric Pathogen Infection.MariaAndreaLaraSalasBelum ada peringkat
- Microbiota-Brain-Gut AxisDokumen9 halamanMicrobiota-Brain-Gut AxisSara OchoaBelum ada peringkat
- Microbiota Effects On Cancer: From Risks To Therapies: Oncotarget, 2018, Vol. 9, (No. 25), PP: 17915-17927Dokumen13 halamanMicrobiota Effects On Cancer: From Risks To Therapies: Oncotarget, 2018, Vol. 9, (No. 25), PP: 17915-17927mutia gondrongBelum ada peringkat
- PGHN 25 194Dokumen17 halamanPGHN 25 194irene.ramadhaniBelum ada peringkat
- Communication Between The Gut Microbiota and PeripDokumen20 halamanCommunication Between The Gut Microbiota and PeripTuna TunBelum ada peringkat
- Ajpgi 00399 2020Dokumen9 halamanAjpgi 00399 2020ahmed KhattabBelum ada peringkat
- Human Microbiome Acquisition and Bioinformatic Challenges in Metagenomic StudiesDokumen12 halamanHuman Microbiome Acquisition and Bioinformatic Challenges in Metagenomic StudiesAminaHodžićBelum ada peringkat
- Reviews: Immunity, Microbiota and Kidney DiseaseDokumen12 halamanReviews: Immunity, Microbiota and Kidney DiseaseEss liBelum ada peringkat
- The Human Microbiota in Health and Disease: EngineeringDokumen12 halamanThe Human Microbiota in Health and Disease: Engineeringخديجة بيو100% (1)
- Does The Buck Stop With The Bugs?: An Overview of Microbial Dysbiosis in Rheumatoid ArthritisDokumen13 halamanDoes The Buck Stop With The Bugs?: An Overview of Microbial Dysbiosis in Rheumatoid ArthritiswiwekaBelum ada peringkat
- Review Article: Probiotics and Gastrointestinal InfectionsDokumen11 halamanReview Article: Probiotics and Gastrointestinal InfectionsFarid FergianBelum ada peringkat
- Neuroscience and Biobehavioral Reviews: Bogdana Golofast, Karel Vales TDokumen20 halamanNeuroscience and Biobehavioral Reviews: Bogdana Golofast, Karel Vales Ttimea_gheneaBelum ada peringkat
- Gut Microbial Flora, Prebiotics and Probiotics in IBD - Their Current Usage and UtilityDokumen10 halamanGut Microbial Flora, Prebiotics and Probiotics in IBD - Their Current Usage and UtilityHyacinth RotaBelum ada peringkat
- Gut Microbiota in Children and Altered Profiles in Juvenile Idiopathic ArthritisDokumen12 halamanGut Microbiota in Children and Altered Profiles in Juvenile Idiopathic ArthritisAndrea Torrico SiacaraBelum ada peringkat
- Clinical Immunology: Review ArticleDokumen13 halamanClinical Immunology: Review Articledoc0814Belum ada peringkat
- Necrotizing Enterocolitis in Newborns: Update in Pathophysiology and Newly Emerging Therapeutic StrategiesDokumen9 halamanNecrotizing Enterocolitis in Newborns: Update in Pathophysiology and Newly Emerging Therapeutic Strategiesemilly vidyaBelum ada peringkat
- Intestinal Microbiota and Sclerosis Lateral AmyotrophicDokumen11 halamanIntestinal Microbiota and Sclerosis Lateral AmyotrophicaluminiossaolucasBelum ada peringkat
- Microbiomes in Physiology Insights Into 21stcentury GlobalDokumen8 halamanMicrobiomes in Physiology Insights Into 21stcentury GlobalLuis Ernesto CastilloBelum ada peringkat
- Clinical Evidence On The Potential Beneficial Effects ofDokumen12 halamanClinical Evidence On The Potential Beneficial Effects ofDyane VatriciaBelum ada peringkat
- the matter of the reproductive microbiome (5)Dokumen9 halamanthe matter of the reproductive microbiome (5)Marcos Vinicio Lopes de CastroBelum ada peringkat
- Fcimb 11 631972Dokumen15 halamanFcimb 11 631972Xime RdzBelum ada peringkat
- Microbes and Infection: Matthew K. Wong, Philip Barbulescu, Bryan Coburn, Elaine Reguera-Nu NezDokumen9 halamanMicrobes and Infection: Matthew K. Wong, Philip Barbulescu, Bryan Coburn, Elaine Reguera-Nu NezSpore FluxBelum ada peringkat
- Microbiota Intestinal e Inmunidad. Review.2020Dokumen15 halamanMicrobiota Intestinal e Inmunidad. Review.2020hacek357Belum ada peringkat
- Antibiotics 10 00719Dokumen39 halamanAntibiotics 10 00719ilhamBelum ada peringkat
- Ajpgi 00008 2022Dokumen18 halamanAjpgi 00008 2022Jéssica Thandara GosseBelum ada peringkat
- Necrotizing Enterocolitis: Old Problem With New Hope: Shu-Fen Wu, Michael Caplan, Hung-Chih LinDokumen6 halamanNecrotizing Enterocolitis: Old Problem With New Hope: Shu-Fen Wu, Michael Caplan, Hung-Chih LintsntbBelum ada peringkat
- Role of The Intestinal Microbiome in Health and Disease: From Correlation To CausationDokumen12 halamanRole of The Intestinal Microbiome in Health and Disease: From Correlation To CausationAlexa MaciucaBelum ada peringkat
- Nutrients 10 01723Dokumen27 halamanNutrients 10 01723nguyen thu trangBelum ada peringkat
- Microorganisms 09 01021Dokumen24 halamanMicroorganisms 09 01021Alice de MoraesBelum ada peringkat
- The Role of Microbiota in Respiratory Health and DiseasesDokumen13 halamanThe Role of Microbiota in Respiratory Health and DiseasesannewidiatmoBelum ada peringkat
- Gut MicrobiotDokumen8 halamanGut MicrobiotJayantiBelum ada peringkat
- Accepted Manuscript: Genomics, Proteomics & BioinformaticsDokumen34 halamanAccepted Manuscript: Genomics, Proteomics & BioinformaticsDiogoBelum ada peringkat
- The Vaginal Microbiota: Insights From High-Throughput SequencingDokumen15 halamanThe Vaginal Microbiota: Insights From High-Throughput SequencingHauBelum ada peringkat
- Extracellular Vesicles Mediated Interaction Within Intes - 2022 - Journal of AdvDokumen13 halamanExtracellular Vesicles Mediated Interaction Within Intes - 2022 - Journal of AdvVinayak29Belum ada peringkat
- Artigo NutriçãoDokumen4 halamanArtigo Nutriçãoannakah18Belum ada peringkat
- 10 1016@j Coviro 2019 05 013Dokumen6 halaman10 1016@j Coviro 2019 05 013BarakBelum ada peringkat
- Hypothesis: Inappropriate Colonization of The Premature Intestine Can Cause Neonatal Necrotizing EnterocolitisDokumen6 halamanHypothesis: Inappropriate Colonization of The Premature Intestine Can Cause Neonatal Necrotizing EnterocolitisLinda MutiaraBelum ada peringkat
- Programming Infant Gut Microbiota: Influence of Dietary and Environmental FactorsDokumen8 halamanProgramming Infant Gut Microbiota: Influence of Dietary and Environmental FactorsMauren Osorio DíazBelum ada peringkat
- Cesárea e Microbiota 2021 - CópiaDokumen16 halamanCesárea e Microbiota 2021 - Cópiayogarte.vivaBelum ada peringkat
- A Review of The Relationship Between Gut Microbiome and ObesityDokumen16 halamanA Review of The Relationship Between Gut Microbiome and ObesityMorana JaganjacBelum ada peringkat
- Prevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDDokumen7 halamanPrevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDMusainah FeisalBelum ada peringkat
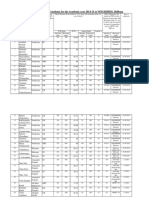
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Dokumen10 halamanAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaBelum ada peringkat
- TLE9 AgriCropProd Q3 Module4 PDFDokumen18 halamanTLE9 AgriCropProd Q3 Module4 PDFJ de GuzmanBelum ada peringkat
- JUSTINE Medical-for-Athletes-2-1Dokumen2 halamanJUSTINE Medical-for-Athletes-2-1joselito papa100% (1)
- Anarchy RPG 0.2 Cover 1 PDFDokumen14 halamanAnarchy RPG 0.2 Cover 1 PDFanon_865633295Belum ada peringkat
- Bcspca Factsheet Life of An Egg Laying Hen PDFDokumen2 halamanBcspca Factsheet Life of An Egg Laying Hen PDFAnonymous 2OMEDZeqCDBelum ada peringkat
- Roberts Race Gender DystopiaDokumen23 halamanRoberts Race Gender DystopiaBlythe TomBelum ada peringkat
- SIWW2024 Water Convention Call For PapersDokumen15 halamanSIWW2024 Water Convention Call For PapersAssistant General Manager R&DBelum ada peringkat
- PE GCSE Revision Quiz - Updated With AnswersDokumen40 halamanPE GCSE Revision Quiz - Updated With AnswersmohitBelum ada peringkat
- MBSR Standards of Practice 2014Dokumen24 halamanMBSR Standards of Practice 2014wasdunichtsagst100% (1)
- Cosmetic BrochureDokumen4 halamanCosmetic BrochureDr. Monika SachdevaBelum ada peringkat
- Dr. Nilofer's Guide to Activator & Bionator AppliancesDokumen132 halamanDr. Nilofer's Guide to Activator & Bionator Appliancesdr_nilofervevai2360100% (3)
- 4400 SystemDokumen24 halaman4400 SystemRaniel Aris LigsayBelum ada peringkat
- University of TasmaniaDokumen3 halamanUniversity of TasmaniaSleepingstar S.Belum ada peringkat
- Fitness WalkingDokumen60 halamanFitness WalkingJC LeriaBelum ada peringkat
- Social Welfare Administrartion McqsDokumen2 halamanSocial Welfare Administrartion McqsAbd ur Rehman Vlogs & VideosBelum ada peringkat
- 32 Vol4 EpaperDokumen32 halaman32 Vol4 EpaperThesouthasian TimesBelum ada peringkat
- Repair of Obstetric Perineal LacerationsDokumen7 halamanRepair of Obstetric Perineal LacerationsadriantiariBelum ada peringkat
- 1 - DS SATK Form - Initial Application of LTO 1.2Dokumen4 halaman1 - DS SATK Form - Initial Application of LTO 1.2cheska yahniiBelum ada peringkat
- Summer Internship Report on Chemist Behavior Towards Generic ProductsDokumen30 halamanSummer Internship Report on Chemist Behavior Towards Generic ProductsBiswadeep PurkayasthaBelum ada peringkat
- L-Sit ProgressionsDokumen2 halamanL-Sit ProgressionsMattBelum ada peringkat
- SGLGB Form 1 Barangay ProfileDokumen3 halamanSGLGB Form 1 Barangay ProfileMark Lenon Par Mapaye100% (1)
- EN Sample Paper 12 UnsolvedDokumen9 halamanEN Sample Paper 12 Unsolvedguptasubhanjali21Belum ada peringkat
- The Digestive System ExplainedDokumen33 halamanThe Digestive System ExplainedGulAwezBelum ada peringkat
- BSHF-101 E.MDokumen8 halamanBSHF-101 E.MRajni KumariBelum ada peringkat
- Lung Cancer - Symptoms and Causes - Mayo ClinicDokumen9 halamanLung Cancer - Symptoms and Causes - Mayo ClinicTakuranashe DebweBelum ada peringkat
- Speaking Level Placement Test Business English PDFDokumen2 halamanSpeaking Level Placement Test Business English PDFLee HarrisonBelum ada peringkat
- Sip Annex 2a Child-Friendly School Survey-3Dokumen9 halamanSip Annex 2a Child-Friendly School Survey-3aimee duranoBelum ada peringkat
- Culture Shock and Adaptation StrategiesDokumen12 halamanCulture Shock and Adaptation StrategiesMuhammad UsmanBelum ada peringkat
- Tingkat KesadaranDokumen16 halamanTingkat KesadaranShinta NurjanahBelum ada peringkat