Anda mungkin juga menyukai
- Anestesia General para Césarea PDFDokumen7 halamanAnestesia General para Césarea PDFAgnese ValentiniBelum ada peringkat
- Subarachnoid Block For Caesarean Section in Severe PreeclampsiaDokumen6 halamanSubarachnoid Block For Caesarean Section in Severe PreeclampsiaAndi BintangBelum ada peringkat
- Medical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TDokumen3 halamanMedical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TAndi BintangBelum ada peringkat
- Overweight linked to increased risk of lower back painDokumen8 halamanOverweight linked to increased risk of lower back painAndi BintangBelum ada peringkat
- Cultural Sociology of Mental Illness n28Dokumen5 halamanCultural Sociology of Mental Illness n28Andi BintangBelum ada peringkat
- Bar A Zanchi 2018Dokumen17 halamanBar A Zanchi 2018Andi BintangBelum ada peringkat
- Anestesia General para Césarea PDFDokumen7 halamanAnestesia General para Césarea PDFAgnese ValentiniBelum ada peringkat
- Procalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaDokumen5 halamanProcalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaAndi BintangBelum ada peringkat
- 1 s2.0 S0002937803001388 MainDokumen3 halaman1 s2.0 S0002937803001388 MainAndi BintangBelum ada peringkat
- 1 s2.0 S1052305714000561 MainDokumen6 halaman1 s2.0 S1052305714000561 MainAndi BintangBelum ada peringkat
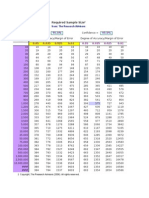
- Required Sample Size: From: The Research AdvisorsDokumen3 halamanRequired Sample Size: From: The Research AdvisorsAbhishek Sharma100% (1)
- Sacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityDokumen5 halamanSacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityAndi BintangBelum ada peringkat
- 1 s2.0 S0002937803001388 MainDokumen3 halaman1 s2.0 S0002937803001388 MainAndi BintangBelum ada peringkat
- Depresión e InmunidadDokumen13 halamanDepresión e InmunidadgabisaenaBelum ada peringkat
- Instruction For Author ClimactericDokumen9 halamanInstruction For Author ClimactericAndi BintangBelum ada peringkat
- 1 s2.0 S0002937800704534 Main PDFDokumen1 halaman1 s2.0 S0002937800704534 Main PDFAndi BintangBelum ada peringkat
- Urologi PDFDokumen237 halamanUrologi PDFAndi BintangBelum ada peringkat
- MK Giz Slide Infant Feeding PracticeDokumen1 halamanMK Giz Slide Infant Feeding PracticeAndi BintangBelum ada peringkat
- Association Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesDokumen10 halamanAssociation Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesAndi BintangBelum ada peringkat
- Prevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationDokumen6 halamanPrevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationAndi BintangBelum ada peringkat
- Cap Bts 2009 ComplitdgDokumen139 halamanCap Bts 2009 ComplitdgAndi BintangBelum ada peringkat
- 1 s2.0 S0021755713002003 MainDokumen6 halaman1 s2.0 S0021755713002003 MainAndi BintangBelum ada peringkat
- 1 s2.0 S0021755713002003 MainDokumen6 halaman1 s2.0 S0021755713002003 MainAndi BintangBelum ada peringkat
- 2013 Student Membership ApplicationDokumen1 halaman2013 Student Membership ApplicationAndi BintangBelum ada peringkat
- Hepatitis C APASLfghDokumen27 halamanHepatitis C APASLfghAndi BintangBelum ada peringkat
- Anthropometry: Ergonomics Additional ResourcesDokumen5 halamanAnthropometry: Ergonomics Additional ResourcesAndi BintangBelum ada peringkat
- ATS Guidelines CAP ManagementDokumen25 halamanATS Guidelines CAP ManagementMae Matira AbeladorBelum ada peringkat
- PCT CAP ABiuytoDokumen10 halamanPCT CAP ABiuytoAndi BintangBelum ada peringkat
- Serviks DocjhjuDokumen366 halamanServiks DocjhjuAndi BintangBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- PH20-000531 SDV Pneumococcal 13-Valent Conjugate Vaccine Prevenar 13 VialDokumen39 halamanPH20-000531 SDV Pneumococcal 13-Valent Conjugate Vaccine Prevenar 13 VialLoanne RamiterreBelum ada peringkat
- Metabolic Bone Disease PDFDokumen50 halamanMetabolic Bone Disease PDFAdBelum ada peringkat
- Morpho - Pathology Final Summary: Chapter 1: Cellular Reactions To AggressionDokumen21 halamanMorpho - Pathology Final Summary: Chapter 1: Cellular Reactions To Aggressiondjxela89Belum ada peringkat
- 11 Vesiculopustular, Bullous and Erosive Diseases of The NeonateDokumen20 halaman11 Vesiculopustular, Bullous and Erosive Diseases of The Neonatecgs08Belum ada peringkat
- MERRF Syndrome: Rare Mitochondrial DiseaseDokumen4 halamanMERRF Syndrome: Rare Mitochondrial DiseaseQuezon D. Lerog Jr.Belum ada peringkat
- Cell Comparison ChartDokumen3 halamanCell Comparison ChartJake BryantBelum ada peringkat
- Abstract Supplement: 2017 ACR/ARHP Annual Meeting November 3-8, 2017 San Diego, CADokumen4.482 halamanAbstract Supplement: 2017 ACR/ARHP Annual Meeting November 3-8, 2017 San Diego, CADavid Gimenez RomeroBelum ada peringkat
- Oxygen-Ozone Autohaemotherapy and Intravescical Oxygen-Ozone Insufflations in Treatment of Recurrent and Interstitial Cystitis: Preliminary ResultsDokumen3 halamanOxygen-Ozone Autohaemotherapy and Intravescical Oxygen-Ozone Insufflations in Treatment of Recurrent and Interstitial Cystitis: Preliminary ResultsSabrina JonesBelum ada peringkat
- Anti-Aging Effects of L-Arginine - ScienceDirectDokumen26 halamanAnti-Aging Effects of L-Arginine - ScienceDirectJohayrah DiangcaBelum ada peringkat
- Internal Medicine Review: Key Concepts and Practice QuestionsDokumen26 halamanInternal Medicine Review: Key Concepts and Practice QuestionsDivine SangutanBelum ada peringkat
- Intestinal AtresiaDokumen16 halamanIntestinal AtresiaMalueth AnguiBelum ada peringkat
- Prof BSP-Akinetic Rigid Synd - PDDokumen139 halamanProf BSP-Akinetic Rigid Synd - PDSavitha BasriBelum ada peringkat
- Pancreatic Function TestsDokumen12 halamanPancreatic Function TestsDhera CharlesBelum ada peringkat
- Approach To Diagnosis of Haemolytic AnaemiasDokumen2 halamanApproach To Diagnosis of Haemolytic AnaemiasGerardLumBelum ada peringkat
- The Microbiome's Impact on HealthDokumen17 halamanThe Microbiome's Impact on HealthDejan PopovBelum ada peringkat
- Clinical Significance of Antinuclear Antibody Staining Patterns and Associated Autoantibodies - UpToDateDokumen13 halamanClinical Significance of Antinuclear Antibody Staining Patterns and Associated Autoantibodies - UpToDateMelanie NgBelum ada peringkat
- Gastrinomas Medical or Surgical TreatmentDokumen25 halamanGastrinomas Medical or Surgical TreatmentTony Miguel Saba SabaBelum ada peringkat
- EMREE Study Guide for Medical Residency Entrance ExamDokumen62 halamanEMREE Study Guide for Medical Residency Entrance Examfayad weezyBelum ada peringkat
- NclexDokumen34 halamanNclexErnie John OyaoBelum ada peringkat
- Brex CVS DrugsDokumen287 halamanBrex CVS DrugsKate EvangelistaBelum ada peringkat
- Approach To Interstitial Lung Disease 2Dokumen58 halamanApproach To Interstitial Lung Disease 2MichaelBelum ada peringkat
- Artificial Intelligence and Deep Learning in OphthalmologyDokumen9 halamanArtificial Intelligence and Deep Learning in OphthalmologySilvia Rossa MuisBelum ada peringkat
- Dumitrita Rodica Bagireanu U4 Assessment Feedback2 (PASS)Dokumen4 halamanDumitrita Rodica Bagireanu U4 Assessment Feedback2 (PASS)Rodica Dumitrita0% (1)
- Back Pain PDFDokumen40 halamanBack Pain PDFsana shiekhBelum ada peringkat
- ExamDokumen1.008 halamanExamPaul Carty SorianoBelum ada peringkat
- Subacute Sclerosing Panencephalitis - Current Perspectives: Pediatric Health, Medicine and Therapeutics DoveDokumen5 halamanSubacute Sclerosing Panencephalitis - Current Perspectives: Pediatric Health, Medicine and Therapeutics DoveClarestaBelum ada peringkat
- Perichondritis PinnaDokumen2 halamanPerichondritis PinnaAnish RajBelum ada peringkat
- Exercise Program Design For Special PopulationDokumen9 halamanExercise Program Design For Special Populationkitu_alagappan4720Belum ada peringkat
- Thyroiditis: Review ArticleDokumen10 halamanThyroiditis: Review Articlexander trujilloBelum ada peringkat
- Physical Changes in The Integumentary System As The Person AgesDokumen10 halamanPhysical Changes in The Integumentary System As The Person AgesDinarkram Rabreca EculBelum ada peringkat