Anda mungkin juga menyukai
- Anxiety Scale - ChildDokumen2 halamanAnxiety Scale - Childbrian@coombsmd.com90% (20)
- Autism Spectrum Ratig ScalesDokumen16 halamanAutism Spectrum Ratig ScalesAndreea Sandu75% (4)
- Vanderbilt Adhd Diagnostic ParentDokumen3 halamanVanderbilt Adhd Diagnostic Parentadinaroman100% (1)
- SRS 2 TemplateDokumen2 halamanSRS 2 TemplateMelanie Greenway33% (3)
- BASC-2 (Parent Child Ages 6 To 11) PDFDokumen3 halamanBASC-2 (Parent Child Ages 6 To 11) PDFLili Carreira100% (2)
- Vanderbilt Rating Scale Scoring InstructionsDokumen2 halamanVanderbilt Rating Scale Scoring InstructionsYeon Ae Narita100% (2)
- Adhd Rating TeacherDokumen2 halamanAdhd Rating TeacherRicardoDG100% (1)
- Child Behavior Check List (CBCL)Dokumen4 halamanChild Behavior Check List (CBCL)Antonella María De Jesús Napán Carbajal100% (2)
- Difficultiesinemotionalregulation ScaleDokumen1 halamanDifficultiesinemotionalregulation ScaleRoxanaElena100% (1)
- CARS - 2 هاد النسخة الجديدة PDFDokumen9 halamanCARS - 2 هاد النسخة الجديدة PDFKhadidja BoutouilBelum ada peringkat
- Vineland Adaptive Behavior ScalesDokumen2 halamanVineland Adaptive Behavior ScalesAlice BulkaBelum ada peringkat
- Depression Scale - ChildDokumen2 halamanDepression Scale - Childbrian@coombsmd.com100% (7)
- Appendix - E.17 Study Start Social Responsiveness Scale-Preschool PDFDokumen4 halamanAppendix - E.17 Study Start Social Responsiveness Scale-Preschool PDFMa Cyril Dawn Muncada50% (2)
- SRS-2 Assessment Reveals Severe Social Difficulties Indicative of ASDDokumen2 halamanSRS-2 Assessment Reveals Severe Social Difficulties Indicative of ASDHong Chun YeohBelum ada peringkat
- Rcmas 2Dokumen1 halamanRcmas 2api-507192289Belum ada peringkat
- Clinician's Handbook of Child Behavioral AssessmentDari EverandClinician's Handbook of Child Behavioral AssessmentPenilaian: 3 dari 5 bintang3/5 (2)
- Revised Childrens Manifest Anxiety ScaleDokumen3 halamanRevised Childrens Manifest Anxiety ScaleAnita Rosalina100% (8)
- Beck Youth InventoryDokumen2 halamanBeck Youth InventoryHina Abbas Khan37% (30)
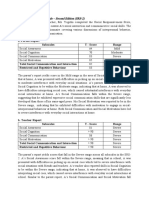
- Adhd Vanderbilt Assessement Teacher Informant 3RD Edition - SensitiveDokumen4 halamanAdhd Vanderbilt Assessement Teacher Informant 3RD Edition - SensitiveStephen Ferry100% (1)
- Conners and Basc2 ReportDokumen11 halamanConners and Basc2 Reportapi-210400247100% (1)
- Child Depression Inventory Cdi InterpretationDokumen2 halamanChild Depression Inventory Cdi InterpretationGerlinde M Schmidt75% (4)
- Vanderbilt ADHD Diagnostic Rating ScaleDokumen2 halamanVanderbilt ADHD Diagnostic Rating ScalevkBelum ada peringkat
- Manual Vineland PDFDokumen101 halamanManual Vineland PDFJosé LuccaBelum ada peringkat
- Child Behavior Checklist (CBCL) PDFDokumen3 halamanChild Behavior Checklist (CBCL) PDFRocio Jimenez Carcamo57% (7)
- Measure Child Conduct Problems (ECBIDokumen4 halamanMeasure Child Conduct Problems (ECBIoctavian100% (1)
- Manual PDFDokumen159 halamanManual PDFDoniLeite33% (3)
- Child Behavior Checklist AssessmentDokumen16 halamanChild Behavior Checklist AssessmentAbhijit Karegaonkar25% (4)
- The Revised Children'S Manifest Anxiety Scale (Rcmas) : "What I Think and Feel"Dokumen3 halamanThe Revised Children'S Manifest Anxiety Scale (Rcmas) : "What I Think and Feel"Rizal Saeful Drajat100% (1)
- Parent Child Relationship Inventory PCRIDokumen3 halamanParent Child Relationship Inventory PCRIselseptianaBelum ada peringkat
- EHNMC BeckDepressionInventory - DSM IVDokumen3 halamanEHNMC BeckDepressionInventory - DSM IVrevectoc50% (2)
- Child Behavior ChecklistDokumen2 halamanChild Behavior ChecklistPricope MadalinaBelum ada peringkat
- Vanderbilt ADHD rating scaleDokumen3 halamanVanderbilt ADHD rating scaleYet Barreda Basbas100% (1)
- RCMAS-2 Manual Provides Assessment of Anxiety in StudentsDokumen4 halamanRCMAS-2 Manual Provides Assessment of Anxiety in StudentsOyiq Yarsi0% (2)
- AQ Child Scoring KeyDokumen3 halamanAQ Child Scoring Keydanielaica21100% (1)
- CBCLDokumen4 halamanCBCLRachmania BudiatiBelum ada peringkat
- Instructions: Below Are A Number of Common Problems That Children Have in School. Please Rate Each Item According ToDokumen1 halamanInstructions: Below Are A Number of Common Problems That Children Have in School. Please Rate Each Item According ToKarina Espina Figueroa100% (1)
- Screening Results Summary and IDEA EligibilityDokumen1 halamanScreening Results Summary and IDEA EligibilitysaraBelum ada peringkat
- Revised Children's Anxiety and Depression Scale (And Subscales) (Rcads)Dokumen6 halamanRevised Children's Anxiety and Depression Scale (And Subscales) (Rcads)e_nov78Belum ada peringkat
- CHILD-parent Relationship ScaleDokumen1 halamanCHILD-parent Relationship ScaleDyane Juntura100% (6)
- Conners 3 Self Report Assessment PDFDokumen18 halamanConners 3 Self Report Assessment PDFJohan ZuñigaBelum ada peringkat
- Beck Youth Inventories Assess Children's EmotionsDokumen12 halamanBeck Youth Inventories Assess Children's EmotionsNarmin Abida22% (9)
- CDI Maria KovacsDokumen3 halamanCDI Maria KovacsWentyAnggrainiBelum ada peringkat
- SDQ InstrumentDokumen4 halamanSDQ InstrumentInggit BanafsajBelum ada peringkat
- Teste SNAP-IV e SWAN - ManualDokumen20 halamanTeste SNAP-IV e SWAN - ManualAnastasio umBelum ada peringkat
- RcmasDokumen9 halamanRcmasapi-507192289Belum ada peringkat
- AQ AdolescentDokumen5 halamanAQ Adolescentdnutter012576Belum ada peringkat
- SDQ English (UK) 4-17scoringDokumen3 halamanSDQ English (UK) 4-17scoringprithiksBelum ada peringkat
- SNAP-IV-C Rating Scale # 6160Dokumen1 halamanSNAP-IV-C Rating Scale # 6160ChrisBelum ada peringkat
- Adaptive Behavior Assessment System-II: Clinical Use and InterpretationDari EverandAdaptive Behavior Assessment System-II: Clinical Use and InterpretationBelum ada peringkat
- Research Design and Planning TechniquesDokumen8 halamanResearch Design and Planning TechniquesAngelique BarizoBelum ada peringkat
- E 456 - 13ae4Dokumen10 halamanE 456 - 13ae4Acilasac 2018100% (2)
- Male Profile: 6-1: - L - L Date: I LDokumen1 halamanMale Profile: 6-1: - L - L Date: I LsaraBelum ada peringkat
- School RefusalDokumen77 halamanSchool RefusalAbhilasha PandeyBelum ada peringkat
- Diagnostic Test in PR1Dokumen4 halamanDiagnostic Test in PR1Anonymous IWfo6JvdA100% (1)
- Reynolds Adolescent Depression Scale PPDokumen18 halamanReynolds Adolescent Depression Scale PPBridget Monroe0% (1)
- Ielts LinkDokumen3 halamanIelts LinkSoikotBelum ada peringkat
- The Revised Children Anxiety TestDokumen21 halamanThe Revised Children Anxiety TestAnonymous jH2v0BBelum ada peringkat
- List Jurnal Kedokteran Gigi Yang Bisa Diakses GratisDokumen2 halamanList Jurnal Kedokteran Gigi Yang Bisa Diakses GratisRizky Darmawan83% (6)
- Separation AnxietyDokumen14 halamanSeparation AnxietyzahradoukBelum ada peringkat
- Reliability and validity of Spanish STAIDokumen1 halamanReliability and validity of Spanish STAIOrero roeoBelum ada peringkat
- Suinn, 2001Dokumen4 halamanSuinn, 2001Mahbub SarkarBelum ada peringkat
- Review of Commonly Used Tests For Assessment For Counselors, 2 EditionDokumen36 halamanReview of Commonly Used Tests For Assessment For Counselors, 2 EditionRolandoEstebanTorresAravenaBelum ada peringkat
- RADS 2chapterDokumen39 halamanRADS 2chapterPrateek Kumar PandaBelum ada peringkat
- Jadwal SPV Desember 2018Dokumen121 halamanJadwal SPV Desember 2018Rizal Saeful DrajatBelum ada peringkat
- Jadwal SPV Desember 2018Dokumen121 halamanJadwal SPV Desember 2018Rizal Saeful DrajatBelum ada peringkat
- Scalling and Root Planing Oleh: Kelompok Dental 24Dokumen17 halamanScalling and Root Planing Oleh: Kelompok Dental 24Rizal Saeful DrajatBelum ada peringkat
- Improving Scaling and Root Planing Over The Past Years A Metaanalysis 2161 1122.1000205Dokumen5 halamanImproving Scaling and Root Planing Over The Past Years A Metaanalysis 2161 1122.1000205Rizal Saeful DrajatBelum ada peringkat
- Music Reduces Dental Patient AnxietyDokumen4 halamanMusic Reduces Dental Patient AnxietyRizal Saeful DrajatBelum ada peringkat
- Xerostomia: Oedijani-Santoso Bagian/SMF Gigi Dan Mulut FK Undip/RSUP DR Kariadi SemarangDokumen40 halamanXerostomia: Oedijani-Santoso Bagian/SMF Gigi Dan Mulut FK Undip/RSUP DR Kariadi SemarangRizal Saeful DrajatBelum ada peringkat
- Kuliah Sistem Pernafasan (DR - Yani)Dokumen29 halamanKuliah Sistem Pernafasan (DR - Yani)Rizal Saeful DrajatBelum ada peringkat
- SelectionList-R1-Web - 04.07.2018 PDFDokumen366 halamanSelectionList-R1-Web - 04.07.2018 PDFRUSHIKESHBelum ada peringkat
- Self-report quality of life measure for people with schizophrenia: the SQLSDokumen6 halamanSelf-report quality of life measure for people with schizophrenia: the SQLSWulandari AdindaBelum ada peringkat
- Research MwthodologyDokumen4 halamanResearch Mwthodologycityboy.angel07Belum ada peringkat
- NATG6 Stratified Sampling TemplateDokumen154 halamanNATG6 Stratified Sampling Templatemichelle.bulfaBelum ada peringkat
- Mms-IV Sem FormateDokumen7 halamanMms-IV Sem FormateVAISHNAVI SALGAONKARBelum ada peringkat
- Advanced Expert Pre-Course QuizDokumen1 halamanAdvanced Expert Pre-Course QuizRo Mi Na100% (1)
- Survey On IELTS CandidatesDokumen1 halamanSurvey On IELTS Candidatesanon_162931207Belum ada peringkat
- Research Design Components and PrinciplesDokumen10 halamanResearch Design Components and PrinciplesChariz AudreyBelum ada peringkat
- BRM 110519071214 Phpapp01Dokumen31 halamanBRM 110519071214 Phpapp01Harpinder KaurBelum ada peringkat
- What Do You Mean by ANCOVA?: Advantages of SPSSDokumen5 halamanWhat Do You Mean by ANCOVA?: Advantages of SPSSAnantha NagBelum ada peringkat
- Non ParametricTestsDokumen57 halamanNon ParametricTestssanjay yadavBelum ada peringkat
- Chapter1Questions and SolutionsDokumen3 halamanChapter1Questions and SolutionsMohammed NajibBelum ada peringkat
- Mps Revised SpeDokumen50 halamanMps Revised SpeJester Ambojnon TuklingBelum ada peringkat
- SSGB Cert InsertDokumen12 halamanSSGB Cert InsertAfzalul Karim NirvickBelum ada peringkat
- Elements of A Test of HypothesisDokumen5 halamanElements of A Test of HypothesisNadia AlamBelum ada peringkat
- Direction: Read Each Question Carefully. Encircle The Letter of The Best AnswerDokumen2 halamanDirection: Read Each Question Carefully. Encircle The Letter of The Best AnswerThons Nacu LisingBelum ada peringkat
- Summative 3-4Dokumen5 halamanSummative 3-4Wilmar EspinosaBelum ada peringkat
- Research Designs and ApproachDokumen32 halamanResearch Designs and Approachdr.anu RkBelum ada peringkat
- Researc H DesignDokumen18 halamanResearc H DesignTj NovalBelum ada peringkat
- Validity and ReliabilityDokumen20 halamanValidity and ReliabilityFahad Mushtaq100% (1)
- Department of Education: Republic of The PhilippinesDokumen16 halamanDepartment of Education: Republic of The PhilippinesAr Anne Ugot100% (1)
- Original Research PaperDokumen4 halamanOriginal Research PaperInigoraniBelum ada peringkat
- Complemento Aula 8Dokumen43 halamanComplemento Aula 8Hamsaveni ArulBelum ada peringkat
- Module No. 9 Title: Testing The Difference Between The Population Means (Large Independent Samples) and (Small Independent Samples)Dokumen13 halamanModule No. 9 Title: Testing The Difference Between The Population Means (Large Independent Samples) and (Small Independent Samples)Janine LerumBelum ada peringkat
- Rohner 2003Dokumen7 halamanRohner 2003Michele Benavides SilvaBelum ada peringkat
- Quantitative Methods Mid QDokumen3 halamanQuantitative Methods Mid Qsap6370Belum ada peringkat