153 Full PDF
Diunggah oleh
Wahyuningsih HamidJudul Asli
Hak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
153 Full PDF
Diunggah oleh
Wahyuningsih HamidHak Cipta:
Format Tersedia
SPECIAL ARTICLE Abhimanyu Garg, MBBS, MD
Management of Scott M. Crundy, MD, PhD
Dyslipidemia in NIDDM
Coronary heart disease is the leading cause of death may be required in many patients. However, first-line
among patients with non-insulin-dependent diabetes drugs for nondiabetic patients (nicotinic acid and bile
mellitus (NIDDM). NIDDM patients have a high acid sequestrants) may be less desirable in NIDDM
frequency of dyslipidemia, which along with obesity, patients than hydroxymethylglutaryl coenzyme A
hypertension, and hyperglycemia may contribute (HMG CoA) reductase inhibitors and even fibric acids.
significantly to accelerated coronary atherosclerosis. In fact, HMG CoA reductase inhibitors may be the
Because risk factors for coronary heart disease are drugs of choice for NIDDM patients with elevated
additive and perhaps multiplicative, even mild degrees LDL cholesterol and borderline hypertriglyceridemia,
of dyslipidemia may enhance coronary heart disease whereas gemfibrozil appears preferable for NIDDM
risk. Therefore, therapeutic strategies for management patients with severe hypertriglyceridemia. Diabetes
of NIDDM should give equal emphasis to controlling Care 13:153-69, 1990
hyperglycemia and dyslipidemia. The National
Cholesterol Education Program recently issued
guidelines for treatment of hyperlipidemia in adults
including diabetic patients. Because of the unique
P
features of diabetic dyslipidemia, however, we suggest atients with non-insulin-dependent diabetes mel-
that certain modifications in these guidelines be litus (NIDDM) commonly have dyslipidemia that
made to meet specific needs of diabetic patients. may contribute to accelerated coronary athero-
For example, therapeutic goals for serum cholesterol sclerosis, the leading cause of death among
reduction should be lower in diabetic patients than
NIDDM patients (1). Lipoprotein abnormalities in NIDDM
in nondiabetic subjects. Particular emphasis should be
given to weight reduction in NIDDM patients. In some patients involve all classes of lipoproteins and may con-
diabetic patients, monounsaturated fatty acids may be sist of chylomicronemia, high levels of very-low-density
a better replacement for saturated fatty acids than lipoprotein (VLDL) and low-density lipoprotein (LDL),
carbohydrates. The target for cholesterol lowering and low levels of high-density lipoprotein (HDL) (2). In
should include both very-low-density lipoprotein some patients with NIDDM, dyslipidemia is secondary
and low-density lipoprotein (LDL) (non-high-density to derangement in intermediary metabolism caused by
lipoprotein) rather than LDL alone. To obtain a insulin deficiency and insulin resistance; in these pa-
substantial reduction of cholesterol levels, drug therapy tients, improved control of hyperglycemia will mitigate
the dyslipidemia. Unfortunately, complete reversal of
From the Center for Human Nutrition and the Departments of Clinical Nutrition, deranged metabolism is rarely possible in NIDDM pa-
Internal Medicine, and Biochemistry, University of Texas Southwestern Medical tients. Consequently, some degree of dyslipidemia usu-
Center at Dallas; and the Veterans Administration Medical Center, Dallas,
Texas.
ally persists despite good glycemic control (3). Some
Address correspondence and reprint requests to Scott M. Grundy, MD, PhD, diabetic patients will have concomitant genetic hyper-
Director, Center for Human Nutrition, University of Texas Southwestern Medical lipidemia; in these patients, diabetes mellitus worsens
Center at Dallas, 5323 Harry Hines Boulevard, Dallas, TX 75235-9052.
Received for publication 29 June 1989 and accepted in revised form 20 Sep- the dyslipidemia, but correction of hyperglycemia will
tember 1989. not normalize lipid levels (4). Frequently, in practice, it
DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990 153
MANAGEMENT OF DYSLIPIDEMIA IN NIDDM
is not possible to determine with certainty the contri- TABLE 2
butions of diabetes and genetics to elevated serum lip- Prevalence (%) of dyslipidemia in non-insulin-dependent
ids. diabetes mellitus (NIDDM): Diabetes Intervention Study,
German Democratic Repulic
NIDDM
PREVALENCE OF DYSLIPIDEMIA Dresden (n = 1139)
population
The prevalence of dyslipidemia in NIDDM patients un- (n = 1216) Men Women
doubtedly varies among different populations. The World
Hypertriglyceridemia
Health Organization multinational study of vascular dis- (triglycerides >2.82 mM) 3.4 11.3 11.2
ease in diabetic subjects revealed a high frequency of Hypercholesterolemia
both hypercholesterolemia and hypertriglyceridemia (cholesterol >7.76 mM) 3.7 3.8 3.2
among adult diabetic individuals from many countries Mixed hyperlipoproteinemia 0.5 3.0 2.6
(5,6; Table 1). The Diabetes Intervention Study found a Total 7.6 18.1 17.0
twofold increase in hyperlipidemia in men and women
with NIDDM compared with the general population of
Dresden, GDR (Table 2; 7). Likewise, the Framingham
Heart Study noted that hypertriglyceridemia and re- LIPOPROTEIN ABNORMALITIES
duced levels of HDL cholesterol (HDL-chol) were in-
creased twofold in adult diabetic patients compared with The most common lipid abnormality of NIDDM is ele-
nondiabetic subjects of both sexes (Table 3; 8). The Pro- vated serum triglycerides (12-16). High levels of serum
spective Cardiovascular Munster Study (9) further con- triglycerides occur mainly in VLDL and can result from
firmed a two- to threefold increase in prevalence of hy- two abnormalities. First, patients with NIDDM over-
pertriglyceridemia, mixed hyperlipidemia, and low levels produce triglyceride-rich VLDL, and this response prob-
of HDL-chol in middle-aged subjects with NIDDM. ably results from increased serum levels of free fatty
According to the National Cholesterol Education Pro- acids and glucose (17-19). In many patients, overpro-
gram (NCEP; 10), people should receive medical su- duction of VLDL results partly from obesity and insulin
pervision to lower serum cholesterol if they have an resistance, but a decrease in insulin secretion in NIDDM
LDL-chol level constantly >4.1 mM or a level ranging may further enhance synthesis of VLDL triglycerides (20).
from 3.4 to 4.1 mM in the presence of coronary heart A second cause of hypertriglyceridemia is retarded li-
disease (CHD) or two other CHD risk factors (Table 4). polysis of VLDL triglycerides, most likely due to reduced
Stern et al. (11) recently assessed the frequency at which lipoprotein lipase activity (15). If the latter becomes se-
NIDDM patients and nondiabetic individuals fall into vere due to marked insulin deficiency, patients can de-
one of these two risk categories. Among 460 NIDDM velop chylomicronemia in addition to elevated VLDL
patients, 43.5% qualified for active medical manage- (type V hyperlipoproteinemia), and such patients are at
ment on the basis of high LDL-chol levels and other risk high risk for acute pancreatitis (21,22). Beyond high
factors, whereas only 23.1% of 4666 nondiabetic sub- concentrations of VLDL, which include VLDL remnants
jects were so qualified. An additional 22.8% of patients or Svedberg flotation constant Sf 20-100 lipoproteins,
with NIDDM had serum triglyceride levels >2.8 mM VLDL particles of diabetic patients contain excess unes-
and/or HDL-chol <0.9 mM, both of which may raise terified cholesterol; the latter may interfere with reverse
CHD risk. cholesterol transport and perhaps even make VLDL more
prone to uptake by arterial wall macrophages (23,24).
In some diabetic patients, the presence of homozygosity
for apolipoprotein E2 (apoE2) may predispose them to
TABLE 1 development of dysbetalipoproteinemia.
Prevalence of dyslipidemia in adult patients with diabetes Patients with NIDDM often do not manifest high LDL-
mellitus: World Health Organization multinational study
chol concentrations compared with nondiabetic sub-
Men (%) Women (%) Both (%) jects of the same population, but many will have an
increase in LDL-apoB levels, similar to that of other
Plasma cholesterol (mM)* hypertriglyceridemic states (25,26). Kissebah et al. (27)
>6.72 22 .6 23.5 23 .1 reported that patients with NIDDM frequently have high
4.65-6.70 58 .2 59.3 58 .8 turnover rates for LDL-apoB, due to either overproduc-
<4.65 19 .3 17.2 18 .2 tion of apoB-containing lipoproteins or to increased
Plasma triglycerides (mM)t conversion of VLDL to LDL. This increased input of LDL
S2.82 19 .2
may raise LDL-chol levels, but even when they are not
1.13-2.81 56 .2
24 .6
elevated, LDL-apoB concentrations can be increased
<1.13
(hyperapobetalipoproteinemia). Furthermore, LDL par-
*Data on 3189 men and 3295 women. ticles frequently are abnormal in NIDDM patients; many
tData from 5 of 14 centers on 1911 subjects. particles are small and dense, but the overall LDL frac-
154 DIABETES CARE, V O L . 13, N O . 2, FEBRUARY 1990
A. GARG AND S.M. GRUNDY
TABLE 3
Prevalence (%) of dyslipidemia in adult patients with diabetes mellitus (DM): Framingham heart study
Men Women
LRC cutoff Normal DM LRC cutoff Normal DM
value* (n = 1074) (n = 130) value* (n = 1449) (n - 135)
Total cholesterol (mM) >6.72 14 13 >7.11 21 24
Triglycerides (mM) >2.65 9 19t >2.26 8 17+
Very-low-density lipoprotein
cholesterol (mM) >1.03 26 34t >0.91 31 38
Low-density lipoprotein
cholesterol (mM) >4.91 11 9 >4.91 16 15
High-density lipoprotein
cholesterol (mM) <0.80 12 21t <1.06 10 25+
* Approximate 90th or 10th percentile age- and sex-matched values from Lipid Research Clinic (LRC) tables are given for comparison with
other studies (see ref. 158).
+P <0.05.
tion tends to be unusually heterogeneous (polydisperse) Low concentrations of HDL-chol and apoAl are yet
(28,29). The abnormalities in LDL composition and me- another characteristic of NIDDM patients (13-16,25,33-
tabolism appear to be partly the result of hypertriglyc- 36). Subfraction analysis of HDL reveals that concentra-
eridemia. For NIDDM patients with moderately severe tions of HDL2-chol in particular are reduced. Low levels
hyperglycemia, a reduced fractional clearance rate for of apoAl are due to increased catabolism of HDL be-
LDL further raises LDL-apoB concentration (20,27). Be- cause production rates for apoAl appear to be normal
cause LDL-apoB levels tend to be increased out of pro- (37). HDL of diabetic patients is enriched in triglyceride
portion to LDL-chol concentrations in NIDDM patients, that may interfere with reverse cholesterol transport; fur-
the levels of LDL-chol fail to reflect true concentrations thermore, preliminary data suggest that in vivo gluco-
of LDL particles. sylation of HDL apolipoproteins can slow down reverse
Some investigators have speculated that hypergly- cholesterol transport (38).
cemia can cause glucosylation of LDL-apoB and thereby
promote uptake of LDL by arterial wall macrophages
(30). Glucosylated LDL has been identified in plasma
but is present in low concentrations, whereas heavier RELATIONSHIP OF DYSLIPIDEMIA IN
glucosylation may occur in LDL trapped in the arterial NIDDM TO CHD RISK
wall and helps to facilitate LDL uptake by macrophages.
Likewise, increased peroxidation of lipids has been de- Risk for CHD in NIDDM patients is at least twice that
scribed in patients with diabetes mellitus, and if LDL of comparable nondiabetic populations (8,39-46). This
lipids trapped in the arterial wall become oxidized, up- increased risk may be related to dyslipidemia, although
take of LDL by macrophages may be enhanced (31,32). coexisting coronary risk factors, e.g., obesity (>30%
above ideal body weight) and hypertension, may also
contribute. In addition, various phenomenon that di-
TABLE 4 rectly accompany diabetes mellitus could accelerate
Classification based on total and low-density lipoprotein atherogenesis, i.e., glucosylation of arterial wall pro-
cholesterol (LDL-chol): National Cholesterol Education teins and lipoproteins, increased peroxidation of lipids,
Program microvascular disease, abnormalities in platelet func-
Total cholesterol (mM) LDL-chol (mM)
tion, and defective hemostasis (31,32,47-51). Besides
these potential aggravating factors, dyslipidemia of di-
Desirable <5.2 <3.4 abetes may play an important role in increasing CHD
Borderline high risk 5.2-6.2 3.4-4.1 risk; thus, the role of serum lipids and lipoproteins in
High risk >6.2 causation of CHD can be considered briefly.
The possible connection between elevated triglycer-
Treatment decisions with either diet or drug therapy are based on risk
ide concentrations and CHD risk has been a subject of
status of patients, whether they already have definite coronary heart
disease, or if they have any two of the following risk factors: male
long debate. Some investigators contend that increased
sex, family history of premature coronary heart disease, cigarette triglycerides are an independent risk factor for CHD
smoking, hypertension, LDL- or high-density lipoprotein cholesterol, (52,53); in most epidemiological studies, triglyceride
diabetes mellitus, definite cerebrovascular or peripheral vascular dis- levels are positively correlated with CHD rates. How-
ease, or severe obesity. ever, when multivariate analysis is used (i.e., when total
DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990 155
MANAGEMENT OF DYSUPIDEMIA IN NIDDM
cholesterol and HDL-chol levels are considered), serum
triglycerides lose much of their predictive power. Serum CLASSIFICATION, DETECTION, AND EVALUATION OF
triglycerides probably are not directly atherogenic, be- DYSUPIDEMIA: TARGETS FOR THERAPY
cause triglycerides typically are not found in athero-
sclerotic plaques. On the other hand, elevations of VLDL A guide to management of dyslipidemia in patients with
triglycerides can induce several lipoprotein abnormali- NIDDM is outlined in the adult treatment panel report
ties that have been implicated in atherogenesis, which of the NCEP (10). This report designates diabetes mel-
include high concentrations of chylomicron remnants, litus as a major risk factor for CHD, and its presence
VLDL remnants, intermediate density lipoproteins, small modifies goals for cholesterol lowering. According to
dense LDL, and reduced concentrations of HDL-chol the guidelines, the initial measurement for all patients
(54-57). Moreover, VLDL from NIDDM patients exhibit is serum total cholesterol. If total cholesterol exceeds
altered metabolic behavior, i.e., they are taken up more 6.2 mM in any individual, diabetic or not, a lipoprotein
readily by macrophages than normal VLDL (58). Recent analysis is indicated regardless of the presence or ab-
reports of the 11-yr follow-up of patients with NIDDM sence of other risk factors. This analysis includes total
or with impaired glucose tolerance from the Paris Pro- cholesterol, triglyceride, and HDL-chol, and it must be
spective Study (59) indicate that hypertriglyceridemia done on fasting serum. From these parameters, LDL-
may be the most potent lipid predictor for CHD mor- chol is estimated by the following equation: LDL-chol
tality. Therefore, although high serum triglycerides may (mM) = total cholesterol - HDL-chol - triglycerides/
not directly cause atherosclerosis, concomitant abnor- 2.18.
malities in lipoprotein metabolism induced by hyper- Furthermore, if the total cholesterol level is in the
triglyceridemia certainly raise the risk for CHD. range of 5.2-6.2 mM, a lipoprotein analysis is indi-
Several studies suggest that LDL levels are not in- cated if CHD or two other risk factors are present (Table
creased in patients with NIDDM compared with non- 4). Because male sex counts as a risk factor, all NIDDM
diabetic individuals. Although by usual criteria LDL-chol men with a borderline high cholesterol level need li-
concentrations may not be raised in NIDDM, LDL me- poprotein analysis. Because being female does not count
tabolism cannot be dismissed as benign. Turnover rates as a risk factor in the guidelines, lipoprotein analysis
for LDL typically are high in NIDDM patients. Further- theoretically is not required in diabetic women with bor-
more, LDL particles tend to be abnormally small and derline high cholesterol levels; however, because sev-
dense, and concentrations of LDL-apoB are often in- eral studies indicate that diabetes wipes out any protec-
creased (29). All of these abnormalities have been re- tion afforded by the female sex against CHD, it seems
ported to increase coronary risk in nondiabetic subjects prudent to measure lipoproteins in NIDDM women with
(60,61). Even borderline elevations of LDL-chol may di- borderline high cholesterol levels as well as in NIDDM
rectly raise CHD risk or signify increased risk in NIDDM men (8,39-41,43,44,46). In fact, considering the high
patients. This is illustrated by the finding of a low prev- prevalence of CHD and complex dyslipidemias in
alence of CHD among patients with NIDDM in certain NIDDM patients, a lipoprotein analysis in patients of
populations, e.g., Pima Indians of Arizona (62), Japa- both sexes probably is justified regardless of the total
nese (5), and Chinese (5); all of these populations have cholesterol concentration.
low concentrations of serum total cholesterol and LDL- The NCEP panel based targets for therapy of dyslipi-
chol (16,63). Thus, if serum LDL-chol could be reduced demia primarily on estimated LDL-chol levels. In the
to low levels in NIDDM patients belonging to higher- absence of CHD or other risk factors, the minimum goal
risk populations, this change should appreciably reduce of lipid-lowering therapy is to lower LDL-chol concen-
their risk for CHD. trations to <4.1 mM. In patients with two other risk
Another common abnormality in NIDDM is a low factors, which we propose should include all NIDDM
concentration of HDL-chol. An inverse correlation be- patients, the minimum goal is an LDL-chol concentra-
tween HDL levels and CHD risk is well established, tion <3.4 mM. Indeed, the NCEP panel indicated that
although mechanisms for this connection are poorly an optimal goal for LDL lowering in high-risk patients is
understood. Some investigators believe that HDL is re- a level in the range of 2.6 mM (10). This goal appears
quired for reverse cholesterol transport and that low HDL appropriate for NIDDM patients who already carry such
levels interfere with removal of excess cholesterol from high risk for CHD and in whom the LDL-chol level may
the walls of coronary arteries. Others suggest that low underestimate the true concentration of LDL particles.
HDL concentrations signify the presence of high con- Because prevalence of CHD is low in diabetic popula-
centrations of other atherogenic lipoproteins, e.g., VLDL tions that typically have LDL-chol levels in the range of
remnants and small dense LDL particles. Whatever the 2.6-3.4 mM, it seems reasonable that this level is a
mechanism, there is no reason to doubt that low HDL desirable goal for all NIDDM patients (16,63).
levels in NIDDM patients are indicative of increased risk However, whether lipid-lowering therapy of NIDDM
for CHD. Thus, abnormalities in all lipoprotein fractions patients should be directed solely toward LDL-chol can
(VLDL, LDL, and HDL) contribute to heightened coro- be questioned. An abnormal distribution of cholesterol
nary risk in NIDDM. in various lipoprotein fractions (VLDL, LDL, and HDL)
156 DIABETES CARE, V O L . 13, N O . 2, FEBRUARY 1990
A. GARG AND S.M. GRUNDY
commonly occurs in NIDDM patients (15,16,25,33,34). Step-One Diet of the NCEP (65). ADA advises liberal
Although triglyceride enrichment of VLDL in NIDDM intakes of carbohydrates up to 55-60% of total energy
may increase VLDL triglyceride-to-cholesterol ratios, in- and restriction of total fat to 30% of total energy. Satu-
creased triglyceride levels typically are accompanied by rated fatty acids are limited to <10% of total energy and
an elevated VLDL-chol level. Indeed, a high VLDL-chol cholesterol to <300 mg/day. In addition, high-fiber foods
level, in addition to a high LDL-chol level, appears to are recommended to increase fiber intake to ~40 g/day.
be a risk factor in NIDDM patients (6,59,64). For this For NIDDM patients with hyperlipidemia, the ADA ad-
reason, we propose that cholesterol in both VLDL and vocates further restriction of dietary fats to 20% of total
LDL be included in risk assessment and therapeutic goals. energy intake and cholesterol to 100-150 mg/day.
This combined fraction may be called non-HDL-chol Despite these recommendations, a recent Consensus
and can be the target for cholesterol lowering (Table 5). Development Conference on Diet and Exercise in
Because of the high prevalence of hypertriglyceridemia NIDDM, sponsored by the National Institutes of Health
and triglyceride enrichment of VLDL particles in NIDDM (66), questioned the wisdom of recommending high-
patients, calculated values of LDL-chol may be falsely carbohydrate diets to all diabetic patients because of
low. The use of non-HDL-chol for NIDDM patients as their potentially harmful effects on lipoprotein levels.
the therapeutic target is simple, accurate, and practical. Concern was expressed about raised triglyceride and
It is independent of triglyceride levels and gives weight VLDL-chol levels and lowered HDL-chol levels resulting
to both VLDL-chol and LDL-chol in risk assessment. If from high-carbohydrate diets. In recognition of differ-
this approach is accepted, the minimum goal of therapy ences of opinion among investigators regarding the de-
in patients with NIDDM is a non-HDL-chol level <4.1 sirable proportion of carbohydrates and fats for diabetic
mM, with the ideal goal being 3.4 mM. Our proposed patients, the NCEP panel indicated that an alternative
use of non-HDL-chol as a target of therapy does not diet with lower intakes of carbohydrates (i.e., 40-45%
extend to the choice of hypolipidemic therapy in dia- of energy) may be appropriate for hyperlipidemic pa-
betic patients. It is necessary to distinguish between VLDL tients with diabetes mellitus (10).
and LDL in the selection of specific therapy in individual Encouraged by the Consensus Development Confer-
patients. One or the other lipoprotein species may pre- ence, we recently compared two approaches to dietary
dominate in a given individual and require a particular treatment of dyslipidemia in patients with NIDDM, i.e.,
mode of therapy. a diet high in carbohydrates versus one high in mono-
unsaturated fatty acids (67). Both diets were low in
saturated fatty acids and cholesterol. Our study revealed
DIETARY THERAPY OF DIABETIC DYSLIPIDEMIA that the diet high in monounsaturates improved gly-
cemic control, reduced triglyceride and VLDL-chol lev-
The NCEP panel advises that dietary therapy for elevated els, and raised HDL-chol levels compared with the high-
cholesterol levels should occur in two steps (10). Die- carbohydrate diet. Moreover, preliminary studies from
tary therapy aims to progressively reduce intakes of sat- our laboratory do not support claims that high-carbo-
urated fatty acids and cholesterol and to eliminate ex- hydrate diets improve insulin sensitivity in NIDDM pa-
cess energy intake. The Step-One Diet calls for reduction tients (68). Therefore, we suggest that partial replace-
of saturated fatty acids to <10% of total energy intake ment of dietary carbohydrates with monounsaturated fatty
and daily cholesterol to <300 mg. The Step-Two Diet acids may be beneficial for certain groups of NIDDM
recommends curtailing saturated fatty acids to <7% of patients (e.g., hypertriglyceridemic patients, those with
total energy intake and cholesterol consumption to <200 HDL-chol levels <0.9 mM, and elderly patients with
mg/day. In both diets, saturated fatty acids are replaced poor compliance with high-carbohydrate diets) and dur-
by carbohydrates, and both diets have a high content of ing pregnancy when energy requirements are high.
carbohydrates (50-60% of total energy). Another issue for the diabetic patient pertains to the
The diet for NIDDM patients recommended by the appropriate dietary content of n-3 polyunsaturated fatty
American Diabetes Association (ADA) is similar to the acids. Fish oils are a rich source of these highly unsat-
urated fatty acids, such as eicosapentaenoic acid (EPA;
TABLE 5 20:5) and docosahexaenoic acid (DHA; 22:6). The n-
Proposed therapeutic goals for men and women with non- 3 polyunsaturates have a potent hypotriglyceridemic ac-
insulin-dependent diabetes mellitus
tion that is dose dependent (69,70). Clinically signifi-
Minimum goal Ideal goal cant reductions in plasma triglyceride levels are usually
(mM) (mM) observed on daily consumption of 5-10 g n-3 polyun-
saturated fatty acids. However, the NCEP panel did not
Total cholesterol <5.2 -4.4 advocate n-3 polyunsaturates for the treatment of hy-
Low-density lipoprotein pertriglyceridemia and advised against the use of fish
cholesterol <3.4 -2.6 oil capsules as a supplement in a therapeutic diet for
Non-high-density lipoprotein
high-risk LDL-chol levels (10). According to the NCEP
cholesterol <4.1 -3.4
panel, the total amount of polyunsaturated fatty acids
DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990 157
MANAGEMENT OF DYSLIPIDEMIA IN NIDDM
(n-6 plus n-3) should be betwen 7 and 10% of daily hance satiety and allow for a decrease in total energy
energy intake, and the relative content of n-6 versus n- intake (84).
3 polyunsaturated fatty acids was not further elaborated. Diabetic patients should consume at least three meals
According to ADA (65), EPA is acceptable in the diet of every day. In some patients with mild hyperglycemia,
patients with diabetes mellitus, but ADA did not make oral hypoglycemic drugs or insulin may be discontinued
specific recommendations as to desirable EPA intakes. before initiation of a weight-loss program. In others,
Preliminary evidence indicates that fish oil polyun- weight reduction can be started after stabilizing gly-
saturates can reduce serum triglyceride levels in NIDDM cemic control with minimum doses of oral hypoglyce-
patients, but they may have adverse effects on glycemic mic drugs or insulin, and as the patient responds by
control (71-73). Of further concern is the increase in losing weight, the dose can be gradually and progres-
LDL-chol and LDL-apoB concentrations that can occur sively reduced. Frequent self-monitoring of blood glu-
in hypertriglyceridemic subjects given fish oil (74,75). cose is essential for some patients to deal with the
Side effects of n-3 polyunsaturates are rare and limited changing metabolic and pharmacological environment
to gastric upset and a bleeding tendency. Furthermore, during weight reduction. If possible, an exercise pro-
if studies prove that n-3 polyunsaturates directly prevent gram should be initiated, although amounts and types
atherosclerosis, they could have an important role in the of exercise will depend on the patient's cardiovascular
treatment of patients with NIDDM. However, until that status. If patients have peripheral vascular disease or
time, their use as a supplement cannot be recom- diabetic foot disease, they may be unable to increase
mended, although their ingestion with fish need not be walking, although they can be encouraged to conduct
curtailed. upper-body exercises. Appetite suppressants are to be
Whatever approach to dietary treatment of NIDDM is avoided completely in NIDDM patients.
selected, emphasis should be on reducing excess body For most patients, use of dietary therapy to control
weight by restricting total energy intake and increasing both glucose and lipid levels should be continued for a
energy expenditure by appropriate exercise. Weight loss period of 3-6 mo before resorting to lipid-lowering drugs.
has been shown to improve both glycemic control and Dietary therapy may be supervised by a physician, but
lipoprotein pattern in NIDDM patients (76-78). Weight assistance of a registered dietitian can be especially help-
reduction may further reduce requirements for antihy- ful in diabetic patients. Any smoker must be urged to
pertensive agents in hypertensive patients with NIDDM. drop the habit. An effort should be made to reduce the
Weight loss is perhaps the only effective measure to dose of or if possible avoid drugs having adverse effects
reduce resistance to the peripheral action of insulin (79, on lipids and lipoproteins (e.g., p-adrenergic blocking
80). High levels of serum triglycerides often respond agents and thiazide and loop diuretics). During dietary
markedly to weight loss, and a modest decrease in LDL- therapy, depending on the severity of hyperglycemia, a
chol levels may occur after only a small reduction in decision can be made about use of oral hypoglycemic
body weight. HDL-chol levels also have been reported agents or insulin for glycemic control. Without fail, con-
to rise after weight reduction, but normalization is not trolling hyperglycemia often mitigates abnormalities in
a consistent finding in NIDDM patients (76-78). lipoproteins and will reduce the need for lipid-lowering
The best approach to weight reduction in NIDDM drugs.
patients is a matter of dispute. Very-low-energy diets are
widely used and have the advantage of promoting rapid
weight reduction that is desired by many patients. How- DRUG THERAPY
ever, there are disadvantages to this approach. Rapid
weight loss can result in undesirable loss of lean body Although the severity of dyslipidemia can be improved
mass or skeletal muscle volume, which is potentially by glycemic control and weight reduction, hypolipi-
detrimental (81). It also induces cholesterol gallstones demic drugs may be appropriate for selected patients
in many patients (82). A gradual sustained weight loss after other therapeutic measures have failed to achieve
is theoretically better because it allows for behavior the proposed goals for cholesterol lowering. According
modification, maintenance of muscle mass, and a lower to the NCEP panel report (10), nicotinic acid and bile
risk for gallstone formation. Unfortunately, many pa- acid sequestrants are drugs of first choice for treatment
tients become discouraged with slow weight reduction of hyperlipidemia; other drugs worthy of consideration
and give up the attempt before they have achieved suc- include lovastatin, gemfibrozil, and probucol. How-
cess. Disagreement about the best weight-reducing diet ever, guidelines of the NCEP panel may not be directly
for diabetic patients also extends to diet composition. applicable to NIDDM patients, and advantages and dis-
Although some believe that high-carbohydrate diets will advantages of each category of drugs for treatment of
promote weight loss, this remains to be proved (83). diabetic dyslipidemia must be considered.
At this time, long-term studies are lacking to determine Nicotinic acid. Because elevated VLDL-chol and re-
which nutrient, carbohydrates, or monounsaturated fatty duced HDL-chol levels are the characteristic lipoprotein
acids are better for inducing weight loss. For some pa- pattern in most patients with NIDDM, nicotinic acid
tients, high-carbohydrate high-fiber diets may be more theoretically should be the drug of choice for diabetic
acceptable, but for others, some fat in the diet may en- dyslipidemia. Nicotinic acid therapy reduces hepatic
158 DIABETES CARE, V O L . 13, N O . 2, FEBRUARY 1990
A. GARG AND S.M. GRUNDY
production of VLDL and thereby lowers both VLDL and ommended in patients with significant hypertriglyceri-
LDL levels (85). Furthermore, the drug usually increases demia (99).
HDL-chol levels (86). The Coronary Drug Project (87) To date, there is a paucity of data on the effectiveness
evaluated long-term nicotinic acid therapy and observed of bile acid sequestrants in patients with NIDDM (100,
a decrease in recurrence rates of myocardial infarction 101). A few comments nonetheless may be in order.
compared with placebo in nondiabetic patients with es- Worsening of hypertriglyceridemia by sequestrant ther-
tablished CHD. In a 15-yr follow-up of the Coronary apy cannot be considered desirable in NIDDM patients
Drug Project, a reduction in total mortality rate was noted who already have a tendency for high levels of plasma
for patients who had received nicotinic acid during the triglycerides. Another common side effect of bile acid
trial (88). Likewise, the Cholesterol Lowering Athero- sequestrants is constipation that may be worsened by
sclerosis Study (89) reported a favorable response to ni- autonomic neuropathy in diabetic patients. Sequestrants
cotinic acid therapy. In this study, the combination of can interfere with intestinal absorption of various drugs,
diet, bile acid sequestrants, and nicotinic acid was shown e.g., digoxin, digitoxin, warfarin, thyroxine, thiazide di-
to retard formation of new atheromas and to cause uretics, and p-adrenergic blockers, and therefore should
regression of coronary plaque in some nondiabetic pa- be used with caution in patients on multiple medica-
tients with preexisting coronary artery disease. tions. Because of these considerations, use of bile acid
However, nicotinic acid therapy is accompanied by sequestrants probably should be limited to a select group
many side effects. Flushing of skin occurs immediately of patients with NIDDM, i.e., those having an isolated
after starting the drug, but its intensity usually decreases increase in LDL-chol levels and normal serum triglyc-
after a period of several weeks. In some patients, con- erides (plasma triglycerides <1.69 mM). Serum triglyc-
comitant administration of aspirin or other nonsteroidal eride levels should be monitored closely in patients with
anti-inflammatory agents helps to prevent severe flush- NIDDM on sequestrant therapy.
ing. Other common side effects include exacerbation of Hydroxymethylglutaryl coenzyme A (HMG CoA) re-
peptic ulcer and reversible abnormalities in liver func- ductase inhibitors. This new class of drugs reduces
tion tests. In patients with NIDDM, nicotinic acid ther- cholesterol synthesis by competitive inhibition of the
apy unfortunately worsens glycemic control and raises rate-limiting enzyme hydroxymethylglutaryl coenzyme
plasma uric acid levels (90-93). We observed definite A (HMG CoA) reductase (102). These drugs reduce the
increases in plasma glucose values and glycosylated cholesterol content of cells and stimulate synthesis of
hemoglobin concentrations and increased glycosuria LDL receptors, particularly in the liver (97). Increased
during nicotinic acid therapy in NIDDM patients (93). hepatic LDL-receptor activity promotes receptor-medi-
Although precise mechanisms whereby nicotinic acid ated clearance of both LDL and VLDL remnants. Lovas-
therapy worsens hyperglycemia in NIDDM patients are tatin was the first drug of this class to be available in the
not known, this response may be due to accentuation U.S., and several others, notably pravastatin and sim-
of insulin resistance (91,94). Moreover, hyperuricemia vastatin, are under evaluation. Lovastatin has now been
induced by nicotinic acid therapy can precipitate gout, used in patients for >7 yr and, based on results thus far,
because patients with NIDDM and impaired glucose tol- holds considerable promise as a cholesterol-lowering
erance are already at increased risk for gout (95,96). drug.
Hyperuricemia may also worsen renal function due to Recent studies from our laboratory revealed that lo-
uric acid nephropathy. Consequently, despite its action vastatin (20 mg twice daily) is highly effective for low-
to improve lipid and lipoprotein levels, nicotinic acid ering plasma lipids in NIDDM patients who have mild
therapy must be used with considerable caution or to moderate increases in total cholesterol levels (103).
avoided altogether in patients with NIDDM. For this In our patients, lovastatin reduced total cholesterol by
reason, nicotinic acid cannot be considered first-line 26%, LDL-chol by 28%, and LDL-apoB by 26%. Lo-
therapy for the dyslipidemia of NIDDM, although it may vastatin therapy also decreased plasma triglyceride and
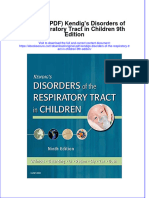
be useful in primary forms of dyslipidemia. VLDL-chol levels by 31 and 42%, respectively, and even
Bile acid sequestrants. These drugs bind to bile acids more so in patients with borderline (moderate) hyper-
in the intestinal tract and interrupt their enterohepatic triglyceridemia (Fig. 1). Although lovastatin did not
circulation. Consequently, more cholesterol is con- change the level of HDL-chol, the total cholesterol-to-
verted into bile acids in the liver. The resultant deple- HDL-chol ratio fell by 29%, which may reflect an over-
tion of hepatic cholesterol content stimulates hepatic all reduction in coronary risk.
LDL-receptor synthesis and thereby promotes removal In our view, HMG CoA reductase inhibitors may soon
of LDL from the circulation (97). In the Lipid Research become the drugs of choice for treatment of dyslipide-
Clinic Primary Prevention Trial, hypercholesterolemic mia in NIDDM. In our study (103), LDL-chol levels were
middle-aged men without diabetes had a reduction in reduced close to the ideal level for NIDDM patients,
CHD risk with cholestyramine therapy (98). As shown i.e., 2.6 mM. Lovastatin therapy effectively lowered not
in this trial, bile acid sequestrants in doses of 16-20 only LDL-chol levels but also decreased concentrations
g/day usually induce a 15-30% lowering of LDL-chol of remnant lipoproteins, as evidenced by a decrease in
levels. Unfortunately, sequestrants tend to increase VLDL-chol. This action on both VLDL and LDL should
serum triglycerides; therefore, their use cannot be rec- reduce non-HDL-chol concentrations to near the ideal
DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990 159
MANAGEMENT OF DYSLIPIDEMIA IN NIDDM
TOTAL CHOLESTEROL LDL - CHOLESTEROL LDL • APOLIPOPROTEIN - B that could interfere with its disposal or with liver dis-
4.5 140 ease.
6.5
Lovastatin produces cataracts in dogs when given in
120
6.0 4.0 very high doses. Although clinical studies with lova-
100 statin have revealed no increase in formation of lentic-
1 5.5 5
5, 80 ular opacities over a period of 1-2 yr in many nondi-
E
5.0
3.0 60
abetic subjects (109,110), the fact that NIDDM patients
4.5
are at increased risk for developing cataracts justifies
2.5 40
periodic slit-lamp examinations during lovastatin ther-
Placebo Lovastatin
0
Placebo Lovastatin
0
Placebo Lovastatin
apy. Certainly, NIDDM patients with mature cataracts
or who have already undergone lens extraction do not
TRIGLYCERDES VLDL - CHOLESTEROL HDL - CHOLESTEROL need slit-lamp examinations if on lovastatin therapy. In
1.3
T 2.5 usual doses, lovastatin does not cause marked reduc-
5.0
1.2 T tions in whole-body synthesis of cholesterol nor does it
2.0
4.0 1.1 decrease levels of cholesterol products, e.g., adrenal
i 3.0 5
o
1.5 and gonadal steroids and bile salts. Reduced lithogen-
E
icity of bile with HMG CoA reductase inhibitors may be
2.0 1.0 0.9
potentially advantageous in NIDDM patients who al-
0.8
1.0 0.5 ready appear to be predisposed to formation of choles-
0.7 terol gallstones (111,112). Other minor side effects of
0 0 oi 1 1
Placebo Lovastatin Placebo Lovastatin Placebo Lovastatin lovastatin include headache, sleep disturbances, and skin
rash.
FIG. 1. Patients with non-insulin-dependent diabetes
mellitus during treatment with placebo and lovastatin. Fibric acid derivatives. Drugs of this class (gemfibrozil,
Plasma levels of total cholesterol, low-density lipopro- clofibrate, and fenofibrate) are potent lipid-lowering
tein cholesterol (LDL-cholesterol), LDL apolipoprotein B, drugs. They may reduce hepatic formation of VLDL tri-
triglycerides, very-low-density lipoprotein cholesterol glycerides, but they promote lipolysis of serum triglyc-
(VLDL-cholesterol), and high-density lipoprotein choles- erides by enhancing the activity of lipoprotein lipase
terol (HDL-cholesterol) in normotriglyceridemic (•, n = (113). In patients with normal triglyceride levels, fibric
7, plasma triglycerides <2.82 mM) and borderline hyper- acids also reduce LDL-chol concentrations by stimulat-
triglyceridemic (A, n = 9, plasma triglycerides 2.82-5.65 ing clearance of LDL from the circulation. On the other
mM) patients. Values are means ± SE. (Figure modified
hand, in hypertriglyceridemic patients, fibric acids raise
from Garg A, Grundy SM: Cardiovasc Rev Rep 9:30-39,
1988.) LDL-chol concomitantly with triglyceride lowering (114).
Fibric acids can raise HDL-chol levels, possibly through
their action to lower triglyceride concentrations. Treat-
level of ~3.4 mM. Lovastatin, however, is not appro- ment of hypertriglyceridemia by fibric acids could the-
priate for patients having severe hypertriglyceridemia with oretically reduce the risk for CHD in several ways. Fibric
excess chylomicrons because it will not reduce triglyc- acid therapy will decrease levels of atherogenic VLDL
erides to a safe range. remnants, may raise HDL-chol, and may reduce the risk
Glycemic control did not deteriorate in our patients of coronary thrombosis. According to some investiga-
on lovastatin therapy, and the drug was well tolerated. tors, hypertriglyceridemia predisposes to coronary
Our finding that this class of drugs does not adversely thrombosis possibly by raising levels of activated factor
affect glycemic control has been confirmed recently by X and enhancing platelet responsiveness; therefore, these
Yoshinoetal. (104) in a 1-yr study of pravastatin therapy abnormalities presumably will be reversed by triglyc-
in 10 patients with NIDDM. eride lowering (115,116).
Lovastatin therapy has been reported to cause minor Clofibrate was the first fibric acid to be used exten-
gastrointestinal upsets, mild and reversible abnormali- sively, and experience with this drug extends to patients
ties in liver function tests, and occasional development with diabetes mellitus. Indeed, there are studies sug-
of myopathy syndrome (105). Lovastatin-induced my- gesting that clofibrate improves glucose tolerance in ad-
opathy can manifest as muscle weakness, soreness and dition to its action to lower triglycerides (117). Despite
tenderness, elevated serum creatine kinase levels and these potential advantages, clofibrate usage has de-
rarely as rhabdomyolysis, myoglobinuria, and acute clined because of the results of the World Health Or-
kidney failure (106-108). Although precise mechanisms ganization study (118). In this study, clofibrate appar-
are not known, myopathy probably results from high ently had side effects that offset its beneficial effect to
serum levels of lovastatin and its metabolites. Severe reduce risk for CHD. Furthermore, more patients in the
myopathy is most likely to occur during concomitant clofibrate group developed diabetes mellitus than in the
use of other medications, e.g., cyclosporin, gemfibrozil, placebo group.
and nicotinic acid, or in patients with hepatic dysfunc- Results of the recently published Helsinki Heart Study
tion impairing drug metabolism (108,109). Therefore, (119) showed that long-term gemfibrozil therapy is gen-
lovastatin should be avoided in any patient taking drugs erally safe and effective for reducing risk for CHD in
160 DIABETES CARE, VOL. 13, NO. 2, FEBRUARY 1990
A. GARG AND S.M. GRUNDY
nondiabetic patients with hypercholesterolemia. Part of was reported to raise fasting and postprandial plasma
the reduction in CHD risk was attributed to an increase glucose levels in patients with NIDDM (121,122). We
in HDL-chol levels. This study has rekindled interest in observed no deleterious action of gemfibrozil on gly-
fibric acid derivatives as lipid-lowering drugs. The Food cemic control. Gemfibrozil, like clofibrate, can cause
and Drug Administration recently approved use of gem- lithogenic bile, and therefore could increase the risk for
fibrozil for lowering cholesterol to reduce the risk of gallstones during long-term use in patients with NIDDM
CHD in patients with type MB hyperlipoproteinemia, (123). Fibric acid derivatives can induce myopathy when
particularly when accompanied by low HDL-chol lev- used alone, particularly in patients with impaired renal
els. function (124). Other side effects of gemfibrozil of lesser
Our experience with gemfibrozil therapy (600 mg concern include various gastrointestinal symptoms, oc-
twice daily) suggests that it is highly effective for low- casional changes in hematologic parameters, and ab-
ering plasma triglyceride levels in NIDDM patients with normal liver function tests. There is no evidence that
severe hypertriglyceridemia, and thus it should reduce gemfibrozil increases risk for malignancy.
risk for acute pancreatitis in these patients (120). Modest Probucol. Probucol is an LDL-loweringdrug. It reduces
elevations in HDL-chol concentrations also occurred in LDL-chol levels by increasing the clearance of LDL (125).
our study, but in most patients, HDL-chol remained <0.9 Whether or not enhanced removal of LDL by probucol
mM despite treatment. Furthermore, LDL-chol levels occurs through receptor-mediated or non-receptor-me-
frequently rose, and LDL-apoB concentrations were not diated mechanisms has not been determined. Probucol
reduced (Fig. 2). Therefore, only limited reduction in also lowers HDL-chol concentrations but does not affect
coronary risk can be expected with gemfibrozil used plasma triglyceride levels. Although probucol reduces
alone in NIDDM patients with marked hypertriglyceri- HDL-chol levels, it apparently can cause regression of
demia. In fact, to reduce risk of CHD, lovastatin might xanthomas in some hypercholesterolemic patients (126).
be added to gemfibrozil therapy for lowering LDL-chol Probucol is carried in LDL particles and is a potent an-
and LDL-apoB levels, and our results support this con- tioxidant (127). Recently, some investigators have pro-
tention (120). However, as mentioned earlier, the com- posed that oxidative modification of LDL may play an
bination of gemfibrozil and lovastatin raises the risk of important role in atherogenesis by facilitating accumu-
severe myopathy (108,109). Because of this, the com- lation of lipids in arterial wall macrophages (128). If this
bination should be used with caution and only in se- mechanism pertains, probucol could retard develop-
lected patients; it cannot be recommended for routine ment of atherosclerosis because it resists oxidation of
use in diabetic patients. LDL. However, this possibility does not justify routine
In earlier studies, long-term therapy with gemfibrozil use of probucol in NIDDM patients, because it currently
remains a theory.
TOTAL CHOLESTEROL LDL- CHOLESTEROL LDL - APOLIPOPROTEIN - B
140
135
SPECIAL CONSIDERATIONS
130
Familial hypercholesterolemia. Some patients with
120 NIDDM have concomitant hyperlipidemias of genetic
115 origin. For example, we recently studied a woman with
0s
NIDDM who was an obligate heterozygote for familial
Placebo Gemfibrozil Placebo Gemlibrozil Placebo Gemfibrozil
hypercholesterolemia; the diagnosis was known be-
TRIGLYCERIDES VLDL- CHOLESTEROL HDL - CHOLESTEROL cause the patient's child had homozygous familial hy-
0.80 percholesterolemia. Despite controlling hyperglycemia
0.75 with insulin therapy, the patient's LDL-chol level re-
0.70
mained markedly elevated. However, she responded to
0.65
lovastatin therapy with near normalization of her lipo-
protein profile (Fig. 3). Thus, familial hypercholestero-
0.60
lemia should be suspected in NIDDM patients who
0.55
persist with severe hypercholesterolemia despite nor-
Placebo Gemfibrozil Placebo Gemfibrozil Placebo Gemfibrozil
malization of plasma glucose. The preferred drug reg-
imen for heterozygous familial hypercholesterolemia
FIG. 2. Plasma levels of total cholesterol, low-density li- appears to be the combination of an HMG CoA reduc-
poprotein cholesterol (LDL-cholesterol), LDL apolipopro- tase inhibitor with bile acid sequestrants (97).
tein B, triglycerides, very-low-density lipoprotein choles- Familial dysbetalipoproteinemia. A few patients with
terol (VLDL-cholesterol), and high-density lipoprotein NIDDM will have concomitant dysbetalipoproteinemia
cholesterol (HDL-cholesterol) in 10 markedly hypertriglyc-
or type III hyperlipoproteinemia. Such patients usually
eridemic (plasma triglycerides >5.65 mM) patients with
non-insulin-dependent diabetes mellitus during treatment have tuberous xanthomas or planar xanthomas (in pal-
with placebo and gemfibrozil. Values are means ± SE. mar creases), accumulation of (3-VLDL, or remnant li-
* P < 0.002; * * P < 0.001. poproteins rich in cholesterol esters. Patients with type
DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990 161
MANAGEMENT OF DYSLIPIDEMIA IN NIDDM
Baseline Insulin + Lovastatln
malities in lipids and lipoproteins even after long-term
good glycemic control, and the presence of hyperlipi-
demia in nondiabetic first-degree relatives. The finding
of concomitant genetic hyperlipidemia in a diabetic pa-
tient should further enhance risk for CHD that will add
to the justification for the use of lipid-lowering drugs. In
such patients, it may not be necessary to try dietary
LDL-C HDL-C
therapy alone for 3-6 mo before turning to hypolipi-
Insulin Dose (units/day) 0
demic drugs.
Mean Plasma Glucoso (mmol/l) 17.7
Mean Body Weight (kg) 65.0 66.5
Type V hyperlipoproteinemia. Occasionally, NIDDM
Glucosylalod Hemoglobin (%) 17.3 12.3
patients present with severe hypertriglyceridemia and
marked elevations in both VLDL and chylomicrons (type
FIG. 3. Plasma levels of total cholesterol (TC), triglycer- V hyperlipoproteinemia). Multiple factors (i.e., hyper-
ides (TG), low-density lipoprotein cholesterol (LDL-C), and glycemia, increased energy intake with obesity, mod-
high-density lipoprotein cholesterol (HDL-C) in 37-yr-old erate-to-heavy alcohol consumption, drugs such as es-
woman with non-insulin-dependent diabetes mellitus and
trogen-containing oral contraceptives and (3-adrenergic
obligate heterozygous familial hypercholesterolemia dur-
ing baseline period (mean of 4 daily determinations), after blockers, and underlying genetic forms of hypertriglyc-
18 days of intensive insulin therapy (insulin; mean of 5 eridemia) may contribute to marked elevations in serum
daily determinations), and 4 wk after treatment with insulin triglycerides in diabetic patients. Such patients are at
and lovastatin (mean of 6 daily determinations). Results increased risk of acute pancreatitis. Miller et al. (22)
are means ± SE. reported that severe abdominal pain of pancreatitis is
likely to occur in patients with serum triglycerides >68
Ill hyperlipoproteinemia are usually homozygous for mM, whereas less severe attacks are common when serum
apoE2/E2 (129). VLDL remnants containing only apoE2 triglycerides are between 23 and 56 mM.
have a poor affinity for hepatic LDL receptors, which Reduction of serum triglycerides in patients with type
explains why VLDL remnants accumulate in plasma. V hyperlipoproteinemia is mandatory to decrease the
Even so, most individuals with apoE2/E2 do not mani- risk for acute pancreatitis. Serum triglycerides preferably
fest type III hyperlipoproteinemia; apparently, another should be lowered to <5.6 mM. Patients presenting with
form of hyperlipidemia must be present concomitantly. acute pancreatitis may need discontinuation of oral in-
Other mutations in apoE, which do not manifest as apoE2, take and should be given parenteral nutrition without
also may impair affinity for LDL receptors and thus may lipid emulsions. Prompt institution of insulin therapy and
contribute to type III hyperlipoproteinemia (130). ApoE2 control of hyperglycemia are necessary in NIDDM pa-
homozygosity is present in — 1 % of the general popu- tients with type V hyperlipoproteinemia. In most cases,
lation; therefore, the apoE2/E2 phenotype and NIDDM chylomicronemia can be eliminated by good control of
may be present in an individual as two unrelated dis- hyperglycemia. If severe hypertriglyceridemia persists
orders (131). The gene frequencies of various apoE al- despite appropriate glycemic control, the patient prob-
leles in patients with NIDDM have been found to be ably has primary type V hyperlipoproteinemia in addi-
similar to that in the nondiabetic population, not favor- tion to NIDDM. For such patients, very-low-fat diets are
ing a genetic linkage between NIDDM and apoE2 hom- helpful for minimizing chylomicron production. Weight
ozygosity (132). On the other hand, there is evidence reduction and restriction of alcohol intake will promote
of an increased frequency of abnormal glucose toler- reduction of triglyceride levels. (3-Adrenergic blocking
ance and NIDDM in patients with type III hyperlipopro- agents can cause marked hypertriglyceridemia in some
teinemia, and this suggests that NIDDM and E2 hom- NIDDM patients and should be withdrawn if possible.
ozygosity interact strongly to produce the type III pattern Fibric acids, e.g., gemfibrozil, are useful for serum tri-
(129). Fibric acids are efficacious in most patients with glyceride lowering in NIDDM patients with persistent
type III hyperlipoproteinemia, although lovastatin also severe hypertriglyceridemia and can be recommended
has been reported to be effective in this form of hyper- for prevention of acute pancreatitis (120). The n-3 poly-
lipidemia (129,133). unsaturated fatty acids have potent hypotriglyceridemic
Other familial hyperlipidemias. Other familial hyper- action, but their potential for treatment of type V hy-
lipidemias, e.g., primary (polygenic) hypercholesterol- perlipoproteinemia in NIDDM patients needs further in-
emia, familial combined hyperlipidemia, and familial vestigation.
hypertriglyceridemia may coexist in patients with Elderly patients with NIDDM. In general, elderly pa-
NIDDM. Unfortunately, a lack of unique markers for tients have not been included in trials for prevention of
these familial hyperlipidemias makes it difficult to di- CHD, but trial results obtained in younger individuals
agnose them with certainty in patients with NIDDM. are frequently extrapolated to the elderly. Recent data
Some features nonetheless suggest the presence of ac- from the Framingham Heart Study reveal that lipid risk
companying genetic hyperlipidemias in NIDDM pa- profiles, including total serum cholesterol, predict CHD
tients including hyperlipidemia out of proportion to the nearly as well in older as in younger people (134). Di-
degree of hyperglycemia, persistence of marked abnor- abetes mellitus seems to impart an unusually high risk
162 DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990
A. GARG AND S.M. GRUNDY
for CHD in the elderly (134). Therefore, reduction of chronic renal insufficiency (140). Although this ap-
cholesterol levels should be appropriate for older NIDDM proach has both experimental and theoretical rationales,
patients with dyslipidemia. The goals of therapy in el- there is limited experience with low-protein diets in
derly NIDDM patients are the same as given in Table 5, clinical practice. General acceptance of such diets by
although nonpharmacological means of lowering cho- most diabetic patients remains to be documented. Fur-
lesterol may be more appropriate for them. Increased thermore, hyperlipidemic patients with diabetic ne-
prevalence of hypothyroidism in the elderly, particularly phropathy, especially those with nephrotic syndrome,
in women, justifies excluding the diagnosis of secondary may not be responsive to usual dietary modifications,
hyperlipidemias due to this condition. i.e., reduction in dietary saturated fatty acids and cho-
Because pharmacokinetics of drugs change with ag- lesterol.
ing, hypolipidemic agents may be more toxic in older There is a paucity of information on the safety and
people and should be used with care. In patients 65- effectiveness of lipid-lowering drugs for patients with
74 yr of age, treatment decisions must be individualized renal insufficiency. Recently, however, HMG CoA re-
and based on the presence or absence of other risk fac- ductase inhibitors have been shown to be effective for
tors and overall health, especially hepatic and renal lowering cholesterol in nondiabetic patients with ne-
function. For those >75 yr of age, the risk-benefit ratio phrotic syndrome; therefore, these drugs could be of use
for drug therapy will often be too high to use drugs. in diabetic nephrotic syndrome (139,141,142). The liver
Moreover, life expectancy of patients >75 yr of age may appears to be the primary route of excretion of lovas-
be too short to expect a long-term benefit from choles- tatin, and ~10% of the orally administered drug and its
terol reduction with drugs; consequently, dietary mod- metabolites are excreted in urine. Therefore, lovastatin
ification should be stressed. should be safe for patients with nephrotic syndrome who
Pregnancy. For pregnant women with NIDDM, dietary have only mild renal insufficiency; whether it is equally
therapy is definitely the first choice for lipid lowering. safe for patients with moderately severe renal failure is
Because the teratogenic effects of hypolipidemic drugs unclear. Experience with lovastatin in patients with di-
are not known, it is best to avoid drug therapy unless abetic nephropathy is not available, and the drug must
absolutely necessary. Hypertriglyceridemia with chy- be used with great caution if at all. Bile acid-binding
lomicronemia can pose immediate risk for acute pan- resins and probucol also have been observed to be safe
creatitis, especially if serum triglyceride concentrations in patients with nephrotic syndrome, but they are not
exceed 11.3 mM. Therefore, for diabetic women with as effective in lowering LDL-chol levels as HMG CoA
severe hypertriglyceridemia, intake of fat should be re- reductase inhibitors (141,143).
stricted, and hyperglycemia should be controlled with For treatment of hypertriglyceridemia in patients with
insulin in the attempt to reduce serum triglyceride lev- chronic renal failure or nephrotic syndrome, clofibrate
els. If marked hypertriglyceridemia persists, fish oil has been used in the past, but an unacceptably high
polyunsaturates may be tried in moderate amounts (5- incidence of myopathy is reported; in some cases, se-
10 g n-3 polyunsaturates/day), closely monitoring gly- vere rhabdomyolysis and myoglobinuria occurred that
cemic control because fish oils may cause hypergly- resulted in acute renal failure (124,144). Myotoxicity is
cemia. attributed to the presence of toxic concentrations of clo-
Diabetic nephropathy. The presentation of diabetic ne- fibrate and its metabolites occurring with renal insuffi-
phropathy may range from microalbuminuria to chronic ciency, because the drug is excreted predominantly by
renal insufficiency and/or nephrotic syndrome (135). the kidneys. Even reduction in the dose of clofibrate, as
Several studies in IDDM patients have shown that dia- suggested by some investigators (145), has not com-
betic nephropathy in its early stages presenting with mi- pletely eliminated the risk of myopathy in uremic pa-
croalbuminuria can raise levels of serum triglycerides, tients (146). Renal excretion is the major route of elim-
VLDL-chol, LDL-chol, and LDL-apoB and reduce levels ination of other fibric acid derivatives, e.g., bezafibrate,
of HDL-chol, in particular HDL2-chol (136,137). This fenofibrate, and gemfibrozil, and the increased risk of
association also may extend to NIDDM patients but has myopathy with fibrates in patients with chronic renal
yet to be documented. In patients with chronic renal failure warrants careful monitoring (147). Theoretically,
insufficiency, reduced functional activity of lipoprotein n-3 polyunsaturated fatty acids should be safe for serum
lipase appears to be the predominant mechanism for triglyceride reduction in patients with chronic renal fail-
hypertriglyceridemia and low levels of HDL-chol (138). ure, but their effectiveness for lowering lipids in such
In patients with nephrotic syndrome, two mechanisms patients remains to be studied.
(i.e., overproduction of apoB-containing lipoproteins, Implications for insulin-dependent diabetes mellitus
VLDL and LDL, and reduced lipoprotein lipase activity) (IDDM). Most patients with IDDM who are maintained
probably account for high levels of both VLDL and LDL under good glycemic control have normal levels of
(139). Often patients with diabetic nephropathy have lipids and lipoproteins, and some patients may even
both chronic renal failure and nephrotic syndrome, and have subnormal levels of VLDL and LDL and increased
their presence may accentuate diabetic dyslipidemia. HDL-chol levels (148). Nonetheless, marked hypertri-
Restriction in protein intake to —40 g/day or 0.8 g/kg glyceridemia with chylomicronemia can occur in insu-
body wt/day is often advised for NIDDM patients with lin-deficient patients who are in poor glycemic control
DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990 163
MANAGEMENT OF DYSLIPIDEMIA IN NIDDM
and have ketoacidosis (149). Such patients can have management. We propose several modifications of the
eruptive xanthomas and lipemia retinalis and may de- guidelines of the NCEPs adult treatment panel to meet
velop acute pancreatitis. The severe hypertriglyceride- specific needs of NIDDM patients. For example, we
mia in most of these patients will disappear with appro- suggest that the therapeutic target for cholesterol low-
priate insulin therapy, and hypolipidemic drugs are rarely ering in NIDDM include both VLDL and LDL (non-
required (149). HDL-chol) rather than LDL-chol alone. Furthermore,
However, it has been noted that IDDM patients with maximum reduction in cholesterol levels may be indi-
microalbuminuria or early incipient nephropathy may cated to minimize risk for CHD in NIDDM. Thus, we
have higher concentrations of serum triglycerides, VLDL- propose that a minimum goal of therapy for non-HDL-
chol, LDL-chol, and LDL-apoB and lower HDL-chol chol be <4.1 mM and the ideal goal be 3.4 mM. This
levels than those without microalbuminuria (136,137). suggestion is made because diabetes appears to enhance
Worsening of dyslipidemia often occurs with progres- risk for CHD even more than other risk factors. At the
sion of diabetic nephropathy. Therefore, IDDM patients very least, the panel's guidelines should be followed.
who develop nephropathy may deserve special attention Reduction in adiposity should be particularly empha-
for lowering lipids and lipoproteins. Unfortunately, ex- sized in NIDDM patients, and for the therapeutic diet,
perience with hypolipidemic drugs is virtually non- we suggest an alternative approach to use monounsa-
existent in IDDM patients, and it seems premature to turated fatty acids rather than carbohydrates as a re-
use them in routine practice. Modification of the diet placement for saturated fatty acids.
should be stressed instead. For most NIDDM patients, lipid-lowering drugs should
If hypolipidemic therapy is deemed necessary for be considered only if a combination of diet, exercise,
IDDM patients with hypercholesterolemia, bile acid se- and hypoglycemic therapy tried for 3-6 mo fails to
questrants may be preferable to lovastatin because no achieve desirable levels of cholesterol. For those with
information is available on lovastatin therapy for IDDM. concomitant genetic hyperlipoproteinemias, hypolipi-
Gemfibrozil may be used in IDDM patients with marked demic therapy may be started without a prolonged trial
hypertriglyceridemia not responding to diet and insulin of dietary therapy. The following recommendations re-
therapy; most of these patients will have concomitant flect our clinical approach to use of lipid-lowering drugs,
genetic hyperlipidemia. Nicotinic acid probably should although consideration can be given to using drugs in
be avoided in IDDM patients because of its numerous the sequence outlined by the NCEP panel. We suggest
side effects. that for patients with isolated elevations of LDL-chol or
Impaired glucose tolerance. Several studies claim that with elevated LDL-chol and borderline hypertriglyceri-
impaired glucose tolerance is associated with increased demia, lovastatin is preferred over bile acid sequestrants
CHD risk (41,150,151). Similar claims have been made because the latter may exacerbate hypertriglyceridemia.
for hyperinsulinemia in the absence of frank diabetes Gemfibrozil, however, is a better choice than lovastatin
mellitus (152-154). However, documentation of a link for NIDDM patients with marked hypertriglyceridemia.
between these factors and CHD risk is not nearly as Finally, nicotinic acid deteriorates glycemic control, in-
strong as for clinical diabetes mellitus. When multivar- duces hyperuricemia and, in our view, cannot be con-
iate analysis is used considering other CHD risk factors, sidered a first-line drug for NIDDM patients.
e.g., hypertension, smoking, and lipoproteins, impaired
glucose tolerance or hyperinsulinemia lose much of their
predictive value. Most patients with primary hypertrig-
lyceridemia manifest impaired glucose tolerance, ACKNOWLEDGMENTS
hyperinsulinemia, or other abnormalities in glucose me-
tabolism, and this association further complicates the This work was supported in part by the Veterans Admin-
issue; most patients with primary hypertriglyceridemia istration, National Institutes of Health Grants HL-29252
never develop frank diabetes mellitus (155-157). Ad- and M01-RR-00633, the Southwestern Medical Foun-
ditional research will be required to determine whether dation, and the Moss Heart Foundation of Dallas, Texas.
impaired glucose tolerance and hyperinsulinemia are
truly linked independently to CHD, the mechanisms for
such a connection, and whether their presence requires REFERENCES
modification of lipid-lowering regimens.
1. Barrett-Connor E, Orchard T: Diabetes and heart dis-
ease. In Diabetes in America. Diabetes Data Compiled
1984. National Diabetes Data Group. Washington, DC,
CONCLUSIONS Dept. of Health and Human Services, 1985, p. XVI-1-
41 (NIH publ. no. 85-1468)
N
IDDM is a major risk factor for CHD, and the 2. Howard BV: Lipoprotein metabolism in diabetes melli-
lipoprotein abnormalities that occur with tus. J Lipid Res 28:613-28, 1987
NIDDM probably contribute to increased CHD 3. Reaven GM: Non-insulin-dependent diabetes mellitus,
risk. Because of the unique features of diabetic abnormal lipoprotein metabolism, and atherosclerosis.
dyslipidemia, special consideration must be given to its Metabolism 36 (Suppl. 1):1-8, 1987
164 DIABETES CARE, V O L . 13, N O . 2, FEBRUARY 1990
A. GARG AND S.M. GRUNDY
4. Brunzell JD, Hazzard WR, Matulsky AC, Bierman EL: mellitus and marked hypertriglyceridemia. Metabolism
Evidence for diabetes mellitus and genetic forms of hy- 33:117-23, 1984
pertriglyceridemia as independent entities. Metabolism 19. Kissebah AH, Alfarsi S, Evans DJ, Adams PW: Integrated
24:1115-21, 1975 regulation of very low density lipoprotein triglyceride
5. Diabetes Drafting Group: Prevalence of small vessel and and apolipoprotein-B kinetics in non-insulin-dependent
large vessel disease in diabetic patients from 14 centres: diabetes mellitus. Diabetes 31:217-25, 1982
the World Health Organization multinational Study of 20. Howard BV, Abbott WGH, Beltz WF, Harper IT, Fields
Vascular Disease in Diabetics. Diabetologia 28 (Suppl. RM, Grundy SM, Taskinen M-R: Integrated study of low
1):615-40, 1985 density lipoprotein metabolism and very low density li-
6. West KM, Ahuja MMS, Bennett PH, Czyzyk A, Mateo poprotein metabolism in non-insulin-dependent diabe-
De Acosta O, Fuller JH, Grab B, Grabauskas V, Jarrett tes. Metabolism 36:870-77, 1987
RJ, Kosaka K, Keen H, Krolewski AS, Miki E, Schliack 21. Chait A, Robertson HT, Brunzell JD: Chylomicronemia
V, Teuscher A, Watkins PJ, Stober JA: The role of cir- syndrome in diabetes mellitus. Diabetes Care 4:343-53,
culating glucose and triglyceride concentrations and 1981
their interactions with other "risk factors" as determi- 22. Miller A, Lees RS, McCluskey MA, Warshaw AL: The
nants of arterial disease in nine diabetic population sam- natural history and surgical significance of hyperlipemic
ples from the WHO multinational study. Diabetes Care abdominal crisis. Ann Surg 190:401-408, 1979
6:361-69, 1983 23. Patti L, Swinburn B, Riccardi G, Howard BV: VLDL
7. Hanefeld M, Schulze J, Fischer S, Julius U, Schmechel subfractions composition in Pima Indians with type 2
H, Haller H: The diabetes intervention study (DIS): a (non-insulin-dependent) diabetes mellitus: comparison
cooperative multi-intervention trial with newly mani- with non-diabetic control subjects (Abstract). Diabeto-
fested type II diabetics: preliminary results. Monogr Ath- logia 30:530A, 1987
erosder 13:98-103, 1985 24. Fielding CJ, Fielding PE: Cholesterol transport between
8. Wilson PWF, Kannel WB, Anderson KM: Lipids, glucose cells and body fluids: role of plasma lipoproteins and
intolerance and vascular disease: the Framingham study. the plasma cholesterol esterification system. Med Clin
Monogr Atherosder 13:1-11, 1985 North Am 66:363-73, 1982
9. Assmann G, Schulte H: The Prospective Cardiovascular 25. Schonfeld G, Birge C, Miller JP, Kessler G, Santiago J:
Munster (PROCAM) study: prevalence of hyperlipidemia Apolipoprotein B levels and altered lipoprotein com-
in persons with hypertension and/or diabetes mellitus position in diabetes. Diabetes 23:827-34, 1974
and the relationship to coronary heart disease. Am Heart 26. Sniderman AD, Wolfson C, Teng B, Franklin FA, Bach-
I 116:1713-24, 1988 orik PS, Kwiterovich PO: Association of hyperapobeta-
10. National Cholesterol Education Program Expert Panel, lipoproteinemia with endogenous hypertriglyeridemia and
National Heart, Lung, and Blood Institute: Report of the atherosclerosis. Ann Intern Med 97:833-39, 1982
National Cholesterol Education Program Expert Panel on 27. Kissebah AH, Alfrasi S, Evans DJ, Adams PW: Plasma
detection, evaluation, and treatment of high blood cho- low density lipoprotein transport kinetics in noninsulin-
lesterol in adults. Arch Intern Med 148:36-69, 1988 dependent diabetes mellitus. I Clin Invest 71:655-67,
11. Stern MP, Patterson JK, Haffner SM, Hazuda HP, Mitch- 1983
ell BD: Lack of awareness and treatment of hyperlipi- 28. Austin MA, Krauss RM: Genetic control of low density
demia in type II diabetes in a community survey. JAMA lipoprotein subclasses. Lancet 2:592-94, 1986
262:360-64, 1989 29. Fisher WR: Heterogeneity of plasma low density lipo-
12. Mancini M, Rivellese A, Rubba P, Riccardi G: Plasma proteins manifestations of the physiologic phenomenon
lipoproteins in maturity onset diabetes. Nutr Metab 24:65- in man. Metabolism 32:283-91, 1983
73, 1980 30. Steinbrecher UP, Witztum JL: Glucosylation of low-den-
13. Barrett-Connor E, Grundy SM, Holdbrook MJ: Plasma sity lipoproteins to an extent comparable to that seen in
lipids and diabetes mellitus in an adult community. Am diabetes slows their catabolism. Diabetes 33:130-34,
1 Epidemiol 115:657-63, 1982 1984
14. Laakso M, Voutilainen E, Sarlund H, Aro A, Pyorala K, 31. Nishigaki I, Hagihara M, Tsunekawa H, Maseki M, Yagi
Penttila I: Serum lipids and lipoproteins in middle-aged K: Lipid peroxide levels of serum lipoprotein fractions
non-insulin-dependent diabetics. Atherosderosis 6:271— of diabetic patients. Biochem Med 25:373-78, 1981
81, 1985 32. Altomare E, Vendemiale G, Procacci V, Giovine A, Al-
15. Taskinen M-R, Nikkila EA, Kussi T, Harno K: Lipoprotein bano O: Increased lipid peroxidation in diabetic patients
lipase activity and serum lipoproteins in untreated type (Abstract). Diabetologia 31:464A, 1988
2 (insulin-independent) diabetes associated with obesity. 33. Uusitupa M, Siitonen O, Voutilainen E, Aro A, Hersio
Diabetologia 22:46-50, 1982 K, Pyorala K, Penttila I, Ehnholm C: Serum lipids and
16. Howard BV, Knowler WC, Vasquez B, Kennedy AL, Pet- lipoproteins in newly diagosed non-insulin-dependent
titt DJ, Bennett PH: Plasma and lipoprotein cholesterol (type II) diabetic patients, with special reference to fac-
and triglyceride in the Pima Indian population: com- tors influencing HDL-cholesterol and triglyceride levels.
parison of diabetics and nondiabetics. Arteriosclerosis Diabetes Care 9:17-22, 1986
4:462-71, 1984 34. Barrett-Connor E, Witztum JL, Holdbrook MJ: A com-
17. Abrams JJ, Ginsberg H, Grundy SM: Metabolism of cho- munity study of high density lipoproteins in adult non-
lesterol and plasma triglycerides in nonketotic diabetes insulin-dependent diabetics. Am J Epidemiol 117:186-
mellitus. Diabetes 31:903-10, 1982 92, 1983
18. Dunn FL, Raskin P, Bilheimer DW, Grundy SM: The 35. GaborJ, Spain M, Kalant N: Composition of serum very-
effect of diabetic control on very low-density lipoprotein low-density and high-density lipoproteins in diabetes.
triglyceride metabolism in patients with type II diabetes Clin Chem 26:1261-65, 1983
DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990 165
MANAGEMENT OF DYSLINDEMIA IN NIDDM
36. Briones ER, Mao SJT, Palumbo PJ, O'Fallon WM, Chen- not for angina pectoris: results from a 10-year follow-up
weth W, Kottke BA: Analysis of plasma lipids and apo- of Uppsala primary preventive study. Atherosclerosis
lipoproteins in insulin-dependent and noninsulin-de- 54:89-97, 1985
pendent diabetes. Metabolism 33:42-49, 1984 54. Weintraub MS, Eisenberg S, Breslow JL: Different pat-
37. Golay A, Zech L, Shi M-Z, Chiou Y-A, Reaven GM, terns of postprandial lipoprotein metabolism in normal,
Chen Y-D: High density lipoprotein (HDL) metabolism type lla, type III, and type IV hyperlipoproteinemic in-
in noninsulin-dependent diabetes mellitus: measure- dividuals: effects of treatment with cholestyramine and
ment of HDL turnover using tritiated HDL. ) Clin En- gemfibrozil. } Clin Invest 79:1110-19, 1987
docrinol Metab 65:512-18, 1987 55. Richards GE, Grundy SM, Cooper K: Influence of plasma
38. Duell PB, Bierman EL: Nonenzymatic glycosylation of triglycerides on lipoprotein patterns in normal subjects
high density lipoprotein inhibits receptor binding (Ab- and in patients with coronary heart disease. Am J Cardiol
stract). Clin Res 37:448A, 1989 63:1214-20, 1989
39. Heyden S, Heiss G, Bartel AG, Hames CG: Sex differ- 56. Austin MA: Plasma triglyceride as a risk factor for cor-
ences in coronary mortality among diabetics in Evans onary heart disease. Am J Epidemiol 129:249-59, 1989
County, Georgia. J Chronic Dis 33:265-73, 1980 57. Krauss RM, Lindgren FT, Ray RM: Interrelationships
40. Barrett-Connor E, Wingard DL: Sex differential in is- among subgroups of serum lipoproteins in normal hu-
chemic heart disease mortality in diabetics: a prospec- man subjects. Clin Chim Acta 104:275-90, 1980
tive population-based study. Am ) Epidemiol 118:489- 58. Kraemer FB, Chen Y-D, Lopez RD, Reaven GM: Effects
96, 1983 of noninsulin-dependent diabetes mellitus on the uptake
41. Jarrett RJ, McCartney P, Keen H: The Bedford Survey: of very low density lipoproteins by thioglycolate-elicited
ten year mortality rates in newly diagnosed diabetics, mouse peritoneal macrophages. / Clin Endocrinol Metab
borderline diabetics and normoglycaemic controls and 61:335-42, 1985
risk indices for coronary heart disease in borderline di- 59. Fontbonne A, Eschwege E, Cambien F, Richard J-L, Du-
abetics. Diabetologia 22:79-84, 1982 cimetiere P, Thibult N, WametJ-M, Claude J-R, Rosselin
42. Butler WJ, Ostrander LD Jr, Carman WJ, Lamphiear DE: G-E: Hypertriglyceridemia as a risk factor of coronary
Mortality from coronary heart disease in the Tecumseh heart disease mortality in subjects with impaired glucose
study: long-term effect of diabetes mellitus, glucose tol- tolerance or diabetes: results from the 11-year follow-
erance and other risk factors. Am J Epidemiol 121:541- up of the Paris prospective study. Diabetologia 32:300-
47, 1985 304, 1989
43. Pan W-H, Cedres LB, Liu K, Dyer A, Schoenberger JA, 60. Sniderman A, Shapiro S, Marpole D, Skinner B, Teng B,
Shekelle RB, Stamler R, Smith D, Collette P, Stamler J: Kwiterovich PO Jr: Association of coronary atheroscle-
Relationship of clinical diabetes and asymptomatic hy- rosis with hyperapobetalipoproteinemia (increased pro-
perglycemia to risk of coronary heart disease mortality tein but normal cholesterol levels in human plasma low-
in men and women. Am I Epidemiol 123:504-16, 1986 density (B) lipoproteins). Proc Natl Acad Sci USA 77:
44. Pyorola K, Laakso M, Uusitupa M: Diabetes and ather- 604-608, 1980
osclerosis: an epidemiologic view. Diabetes Metab Rev 61. Austin MA, Breslow JL, Hennekens CH, BuringJE, Wil-
3:463-524, 1987 lett WC, Krauss RM: Low-density lipoprotein subclass
45. Kleinman JC, Donahue RP, Harris Ml, Finucane FF, Ma- patterns and risk of myocardial infarction. JAMA 260:
dans JH, Brock DB: Mortality among diabetics in a na- 1917-21, 1988
tional sample. Am j Epidemiol 128:389-401, 1988 62. Ingelfinger JA, Bennett PH, Liebow IM, Miller M: Cor-
46. Zimmet PZ, Finch CF, Schooneveldt MG, King HO, onary heart disease in the Pima Indians: electrocardi-
Thoma K: Mortality from diabetes in Nauru: results of ographic findings and postmortem evidence of myocar-
4-yr follow-up. Diabetes Care 11:305-10, 1988 dial infarction in a population with high prevalence of
47. Ruderman NB, Haudenschild C: Diabetes as an ather- diabetes mellitus. Diabetes 25:561-65, 1976
ogenic factor. Prog Cardiovasc Dis 26:373-412, 1984 63. Pan X-R, Walden CE, Warnick GR, Hu S-X, Albers JJ,
48. Brownlee M, Cerami A, Vlassara H: Advanced glyco- Cheung M, Bierman EL: Comparison of plasma lipopro-
sylation end products in tissue and the biochemical basis teins and apolipoproteins in Chinese and American non-
of diabetic complications. N Engl) Med 318:1315-21, insulin-dependent diabetic subjects and controls. Dia-
1988 betes Care 9:395-400, 1986
49. Ledet T, Gotzsche O, Heickendorff L: The pathology of 64. Laakso M, Ronnemaa T, Pyorala K, Kallio V, Puukka P,
diabetic cardiopathy: pathogenetic reflections. In Dia- Penttila I: Atherosclerotic vascular disease and its risk
betes and Heart Disease. Jarrett RJ, Ed. Amsterdam, El- factors in non-insulin-dependent diabetic and nondi-
sevier, 1984, p. 25-46 abetic subjects in Finland. Diabetes Care 11:449-63,
50. Colwell JA, Halushka PV, Sarji KE, Sagel J: Platelet func- 1988
tion and diabetes mellitus. Med Clin North Am 62:753- 65. American Diabetes Association: Nutritional recommen-
66, 1978 dations and principles for individuals with diabetes mel-
51. Greaves M, Preston FE: Haemostatic abnormalities in litus: 1986. Diabetes Care 10:126-32, 1987
diabetics. In Diabetes and Heart Disease. Jarrett RJ, Ed. 66. National Institutes of Health: Consensus development
Amsterdam, Elsevier, 1984, p. 47-80 conference on diet and exercise in non-insulin-depen-
52. Carlson LA, Bottiger LE: Risk factors for ischaemic heart dent diabetes mellitus. Diabetes Care 10:639-44, 1987
disease in men and women: results of the 19-year fol- 67. Garg A, Bonanome A, Grundy SM, Zhang Z-J, Unger
low-up of the Stockholm prospective study. Acta Med RH: Comparison of a high-carbohydrate diet with a high-
Scand 218:207-11, 1985 monounsaturated-fat diet in patients with non-insulin-
53. Aberg H, Lithell H, Selinus I, Hedstrand H: Serum tri- dependent diabetes mellitus. N Engl I Med 319:829-34,
glycerides are a risk factor for myocardial infarction but 1988
166 DIABETES CARE, VOL. 13, NO. 2, FEBRUARY 1990
A. GARG AND S.M. GRUNDY
68. Garg A, Grundy SM, Helderman JH, Unger RH: High nicotinic acid on metabolism of cholesterol and triglyc-
carbohydrate diets do not induce insulin sensitivity in erides in man. ) Lipid Res 22:24-36, 1982
NIDDM patients (Abstract). Diabetes 38 (Suppl. 2):46A, 86. Shepherd J, Packard CJ, Patsch JR, Gotto AM Jr, Taunton
1989 OD: Effects of nicotinic acid therapy on plasma high
69. Phillipson BE, Rothrock DW, Connor WE, Harris WS, density lipoprotein subfraction distribution and compo-
Illingworth DR: Reduction of plasma lipids, lipoproteins sition and on apolipoprotein A metabolism. J Clin Invest
and apoproteins by dietary fish oils in patients with hy- 63:858-67, 1979
pertriglyceridemia. N Engl J Med 312:1210-16, 1985 87. Coronary Drug Project Research Group: Clofibrate and
70. Spiller GA, Jensen CD, Scala J: Effect of low dose omega- niacin in coronary heart disease. JAMA 231:360-81,
3 fatty acids on plasma fatty acids and lipids (Abstract). 1975
Clin Res 35:779A, 1987 88. Canner PL, Berge KG, Wenger NK, Stamler J, Friedman
71. Glauber H, Wallace P, Griver K, Brechtel G: Adverse L, Prineas RJ: Fifteen-year mortality in Coronary Drug
metabolic effect of omega-3 fatty acids in non-insulin- Project patients: long-term benefit with niacin. j Am Coll
dependent diabetes mellitus. Ann Intern Med 108:663- Card/o/8:1245-55, 1986
68, 1988 89. Blankenhorn DH, Nessim SA, Johnson RL, Snamarco
72. Schectman G, Kaul S, Kissebah AH: Effect of fish oil ME, Azen SP, Cashin-Hemphill L: Beneficial effects of
concentrate on lipoprotein composition in NIDDM. Di- combined colestipol-niacin therapy on coronary athero-
abetes 37:1567-73, 1988 sclerosis and coronary venous bypass grafts. JAMA 257:
73. Friday KE, Childs MT, Tsunehara CH, Fujimoto WY, 3233-40, 1987
Bierman EL, Ensinck JW: Elevated plasma glucose and 90. Gurian H, Aldersberg D: The effect of large doses of
lowered triglyceride levels from omega-3 fatty acid sup- nicotinic acid on circulating lipids and carbohydrate tol-
plementation in type II diabetes. Diabetes Care 12:276— erance. Am I Med Sci 237:12-22, 1959
81, 1989 91. Miettinen TA, Taskinen M-R, Pelkonen R, Nikkila EA:
74. Simons LA, Hickie JB, Balasubramaniam S: On the ef- Glucose tolerance and plasma insulin in man during
fects of dietary n-3 fatty acids (Maxepa) on plasma lipids acute and chronic administration of nicotinic acid. Ada
and lipoproteins in patients with hyperlipidaemia. Ath- Med Scand 186:247-53, 1969
erosclerosis 54:75-88, 1985 92. Molnar GD, Berge KG, Rosevear JW, McGuckin WF,
75. Sullivan DR, Sanders TAB, Trayner IM, Thompson GR: Achor WP: The effect of nicotinic acid in diabetes mel-
Paradoxical elevation of LDL apoprotein B levels in litus. Metabolism 13:181-89, 1964
hypertriglyceridemic patients and normal subjects in- 93. Garg A, Grundy SM: Nicotinic acid may not be first line
gesting fish oil. Atherosclerosis 61:129-34, 1986 therapy for dyslipidemia in non-insulin-dependent dia-
76. Kennedy L, Washe K, Hadden DR, Weaver JA, Buch- betes mellitus (NIDDM) (Abstract). Clin Res 37:449A,
anan KD: The effect of intensive dietary therapy on serum 1989
high density lipoprotein-cholesterol in patients with type 94. Kahn SE, Beard JC, Schwartz MW, Ward WK, Ding HL,
2 non-insulin-dependent diabetes mellitus: a prospec- Bergman RN, Taborsky GJ Jr, Porte D Jr: Increased (3-
tive study. Diabetologia 23:24-27, 1982 cell secretory capacity as mechanism for islet adaptation
77. Wolf RN, Grundy SM: Influence of weight reduction on to nicotinic acid-induced insulin resistance. Diabetes
plasma lipoproteins in obese patients. Arteriosclerosis 38:562-68, 1989
3:160-69, 1983 95. Weiss TE, Segaloff A, Moore C: Gout and diabetes. Me-
78. Hughes TA, Gwynne JT, Switzer BR, Herbst C, White tabolism 6:103-106, 1957
G: Effects of caloric restriction and weight loss on gly- 96. Whitehouse FW, Cleary WJ Jr: Diabetes mellitus in pa-
cemic control, insulin release and insulin resistance, and tients with gout. JAMA 197:73-76, 1966
atherosclerotic risk in obese patients with type II diabetes 97. Bilheimer DW, Grundy SM, Brown MS, Goldstein JL:
mellitus. Am J Med 77:7-17, 1984 Mevinolin and colestipol stimulate receptor-mediated
79. Zawadzki JK, Bogardus C, Foley JE: Insulin action in clearance of low density lipoprotein from plasma in fa-
obese non-insulin-dependent diabetics and in their iso- milial hypercholesterolemia heterozygotes. Proc Natl Acad
lated adipocytes before and after weight loss. Diabetes Sci USA 80:4124-28, 1983
36:227-36, 1987 98. Lipid Research Clinic Program: The Lipid Research Clinic
80. Henry RR, Wallace P, Olefsky JM: Effects of weight loss Coronary Primary Prevention Trial results. II. The rela-
on mechanisms of hyperglycemia in obese non-insu- tionship of reduction in incidence of coronary heart dis-
lin-dependent diabetes mellitus. Diabetes 35:990-98, ease to cholesterol lowering. JAMA 251:365-74, 1984
1986 99. Crouse JR: Hypertriglyceridemia: a contraindication to
81. Garrow JS: Combined medical-surgical approaches to the use of bile acid binding resins. Am J Med 83:243-
treatment of obesity. Am J Clin Nutr 33:425-30, 1980 48, 1987
82. Broomfield PH, Chopra R, Sheinbaum RC, Bonorris GG, 100. Bandisode MS, Boshell BR: Hypocholesterolemic activ-
Silverman A, Schoenfield LJ, Marks JW: Effects of urso- ity of colestipol in diabetes. Curr Ther Res 18:276-84,
deoxycholic acid and aspirin on the formation of litho- 1975
genic bile and gallstones during loss of weight. N Engl 101. Duntsch VG: Langzeittherapie der Hypercholesterina-
I Med 319:1567-72, 1988 mie beim Diabetiker mit colestipol. Fortschr Med 99:73-
83. Sims EAH, Danforth E Jr: Expenditure and storage of 75, 1981
energy in man. / Clin Invest 79:1019-25, 1987 102. Endo A, Kurodo M, Tsujita G: ML-236A, ML-236B, and
84. Garg A, Grundy SM: High monounsaturated fat diet for ML-236C, new inhibitors of cholesterogenesis produced
non-insulin-dependent diabetes mellitus (Letter). N Engl by Penicillium citrinum. J Antibiot (Tokyo) 29:1346-48,
J Med 320:536-37, 1989 1976
85. Grundy SM, Mok HYI, Zech L, Berman M: Influence of 103. Garg A, Grundy SM: Lovastatin for lowering cholesterol
DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990 167
MANAGEMENT OF DYSUPIDEMIA IN NIDDM
levels in non-insulin-dependent diabetes mellitus. N Engl nation with lovastatin for treatment of hypertriglyceri-
) Med 318:81-86, 1988 demia in NIDDM. Diabetes 38:364-72, 1989
104. Yoshino G, Kazumi T, Iwai M, Matsushita M, Matsuba 121. Marks J, Howard AN: A comparative study of gemfibro-
K, Uenoyama R, Iwatani I, Baba S: Long-term treatment zil and clofibrate in the treatment of hyperlipidemia in
of hypercholesterolemic non-insulin-dependent diabetes patients with maturity-onset diabetes. Res Clin Forum
mellitus (NIDDM) with pravastatin (CS-514). Athero- 4:95-103, 1982
sclerosis 75:67-72, 1989 122. Konttinen A, Kuisma I, Raili R, Pohjola S, Ojala K: The
105. Grundy SM: HMG-CoA reductase inhibitors for treat- effect of gemfibrozil on serum lipids in diabetic patients.
ment of hypercholesterolemia. N Engl J Med 319:24- Ann Clin Res 11:240-45, 1979
33, 1988 123. Leiss O, von Bergmann K, Gnasso A, Augustin J: Effect
106. East C, Alivizatos PA, Grundy SM, Jones PH, Farmer JA: of gemfibrozil on biliary lipid metabolism in normoli-
Rhabdomyolysis in patients receiving lovastatin after pemic subjects. Metabolism 34:74-82, 1985
cardiac transplantation (Letter). N Engl j Med 318:47- 124. Pierides AM, Alvarez-Ude F, Kerr DNS, Skillen AW: Clo-
48, 1988 fibrate-induced muscle damage in patients with chronic
107. Norman DJ, Illingworth DR, MunsonJ, Hosenpud J: My- renal failure. Lancet 2:1279-82, 1975
olysis and acute renal failure in a heart-transplant recip- 125. Kesaniemi YA, Grundy SM: Influence of probucol on
ient receiving lovastatin (Letter). N Engl) Med 318:46- cholesterol and lipoprotein metabolism in man. / Lipid
47, 1988 Res 25:780-90, 1984
108. Tobert JA: Rhabdomyolysis in patients receiving lova- 126. Yamamoto A, Matsuzawa Y, Yokoyama S, Funahashi T,
statin after cardiac transplantation (Letter). N Engl) Med Yamamura T, Kishino B-l: Effects of probucol on xan-
318:48, 1988 thomata regression in familial hypercholesterolemia. Am
109. Tobert JA: Efficacy and long-term adverse effect pattern J Cardiol 57:29-35H, 1986
of lovastatin. Am J Cardiol 62:28J-34, 1988 127. Parthasarathy S, Young SG, Witztum JL, Pittman RC,
110. Hunninghake DB, Miller VT, Goldberg I, Schonfeld G, Steinberg D: Probucol inhibits oxidative modification of
Stein EA, Tobert JA: The Lovastatin Study Group. II. Lo- low density lipoprotein. / Clin Invest 77:641-44, 1986
vastatin: follow-up ophthalmologic data. )AMA 259:354- 128. Steinberg D, Parthasarathy S, Carew TE, Khoo JC, Witz-
55, 1988 tum JL: Beyond cholesterol: modifications of low-density
111. Duane WC, Hunninghake DB, Freeman ML, Pooler PA, lipoprotein that increase its atherogenticity. N Engl J Med
Schlasner LA, Gebhard RL: Simvastatin, a competitive 320:915-24, 1989
inhibitor of HMG-CoA reductase, lowers cholesterol sat- 129. Morganroth J, Levy Rl, Fredrickson DS: The biochemi-
uration index of gallbladder bile. Hepatology 8:1147- cal, clinical, and genetic features of type III hyperlipo-
50, 1988 proteinemia. Ann Intern Med 82:158-74, 1975
112. Bennion LJ, Grundy SM: Effects of diabetes mellitus on 130. Rail SC Jr, Newhouse YM, Clarke RG, Weisgraber KH,
cholesterol metabolism in man. N Engl) Med 296:1365- McCarthy BJ, Mahley RW, Bersot TP: Type III hyperli-
71, 1977 poproteinemia associated with apolipoprotein E phen-
113. Saku K, Gartside PS, Hynd BA, Kashyap ML: Mechanism otype E3/3: structure and genetics of an apolipoprotein
of action of gemfibrozil on lipoprotein metabolism. / E3 variant. / Clin Invest 83:1095-101, 1989
Clin In vest 75:1702-12, 1985 131. Uterman G, Steinmetz A, Weber W: Genetic control of
114. Vega GL, Grundy SM: Gemfibrozil therapy in primary human apolipoprotein E polymorphism: comparison of
hypertriglyceridemia associated with coronary heart dis- one- and two-dimensional techniques of isoprotein anal-
ease: effects on metabolism of low-density lipoproteins. ysis. Hum Genet 60:344-51, 1982
JAMA 253:2398-403, 1985 132. Eto M, Watanabe K, Iwashima Y, Morikawa A, Oshima
115. Bradley WA, Gianturco SH: Vitamin K-dependent pro- E, Sekiguchi M, Ishii K: Apolipoprotein E polymorphism
teins bind to very low-density lipoproteins. Semin Thromb and hyperlipemia in type II diabetics. Diabetes 35:1374-
Hemostasis 14:253-57, 1988 82, 1986
116. Brook JG, Aviram M: Platelet lipoprotein interactions. 133. Vega GL, East C, Grundy SM: Lovastatin therapy in fa-
Semin Jhromb Hemostasis 14:258-65, 1988 milial dysbetalipoproteinemia: effects on kinetics of
117. Kobayashi M, Shigeta Y, Hirata Y, Omori Y, Sakaoto N, apolipoprotein B. Atherosclerosis 70:131-43, 1988
Namby S, Baba S: Improvement of glucose tolerance in 134. Castelli WP, Wilson PWF, Levy D, Anderson K: Cardio-
NIDDM by clofibrate: randomized double-blind study. vascular risk factors in the elderly. Am jCardiol 63:12H-
Diabetes Care 11:495-99, 1988 19, 1989
118. Committee of Principal Investigators: A co-operative trial 135. Mogensen CE: Microalbuminuria predicts clinical pro-
in the primary prevention of ischaemic heart disease us- teinuria and early mortality in maturity-onset diabetes.
ing clofibrate: report from the Committee of Principal N Engl J Med 310:356-60, 1984
Investigators. Br Heart I 40:1069-118, 1978 136. Vannini P, Ciavarella A, Flammini M, Bargossi AM, For-
119. Frick MH, Elo O, Happa K, Heinonen OP, Heinsalmi P, lani G, Borgnino LC, Orsoni G: Lipid abnormalities in
Helo P, Huttunen JK, Kaitaniemi P, Koshinen P, Man- insulin-dependent diabetic patients with albuminuria.
ninen V, Maenpaa H, Malkonen M, Manttari M, Norolas Diabetes Care 7:151-54, 1984
S, Pasternack A, Pikkarainen J, Romo M, Sjoblom T, 137. Winocour PH, Durrington PN, Ishola M, Anderson DC,
Nikkila EA: Helsinki heart study: primary-prevention trial Cohen H: Influence of proteinuria on vascular disease,
with gemfibrozil in middle-aged men with dyslipidemia, blood pressure, and lipoproteins in insulin dependent
safety of treatment, changes in risk factors, and inci- diabetes mellitus. Br Med) 294:1648-51, 1987
dence of coronary heart disease. N Engl J Med 317:1237- 138. Bagdade JD, Porte D Jr, Bierman EL: Hypertriglyceri-
45, 1987 demia: a metabolic consequence of chronic renal fail-
120. Garg A, Grundy SM: Gemfibrozil alone and in combi- ure. N Engl} Med 279:181-85, 1968
168 DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990
A. GARG AND S.M. GRUNDY
139. Vega GL, Grundy SM: Lovastatin therapy in nephrotic tality from coronary heart disease and stroke in relation
hyperlipidemia: effects on lipoprotein metabolism. Kid- to degree of glycaemia: the Whitehall study. Br Med )
neylnt 33:1060-68, 1988 287:867-70, 1983
140. Noth RH: Diabetic nephropathy: hemodynamic basis 151. Stamler R, Stamler J (Eds.): Asymptomatic hypergly-
and implications for disease management. Ann Intern cemia and coronary heart disease: a series of papers by
Med 110:795-813, 1989 the International Collaborative Group, based on studies
141. Rabelink AJ, Hene RJ, Erkelens DW, Joles JA, Koomans in fifteen populations.) Chronic Dis 32:683-837, 1979
HA: Effects of simvastatin and cholestyramine on lipo- 152. Welborn TA, Wearne K: Coronary heart disease inci-
protein profile in hyperlipidaemia of nephrotic syn- dence and cardiovascular mortalilty in Busselton with
drome. Lancet 2:1335-38, 1988 reference to glucose and insulin concentrations. Dia-
142. Golper TA, Illingworth DR, Morris CD, Bennett WM: betes Care 2:154-60, 1979
Lovastatin in the treatment of multifactorial hyperlipi- 153. Pyorala K, Savolainen E, Kaukola S, Happakoski J: Plasma
demia associated with proteinuria. Am / Kidney Dis insulin as coronary heart disease risk factor: relationship
13:312-20, 1989 to other risk factors and predictive value during 9 1/2-
143. lida H, Izumino K, Asaka M, Fujita M, Nishino A, Sa- year follow-up of the Helsinki Policemen Study popu-
sayama S: Effect of probucol on hyperlipidemia in pa- lation. Ada Med Scand Suppl 701:38-52, 1985
tients with nephrotic syndrome. Nephron 47:280-83, 154. Fontbonne A, Tchobroutsky G, Eschwege E, Richards JL,
1987 Claude JR, Rosselin GE: Coronary heart disease mortality
144. Bridgman JF, Rosen SM, Thorp JM: Complications during risk: plasma insulin level is a more sensitive marker than
clofibrate treatment of nephrotic-syndrome hyperlipo- hypertension or abnormal glucose tolerance in over-
proteinaemia. Lancet 2:506-509, 1972 weight males: the Paris prospective study. I Obes 12:557—
145. Goldberg AP, Sherrard DJ, Haas LB, BrunzellJD: Control 65, 1988
of clofibrate toxicity in uremic hypertriglyceridemia. Gin 155. Olefsky JM, Farquhar JW, Reaven GM: Reappraisal of
Pharmacol Ther 21:317-25, 1977 the role of insulin in hypertriglyceridemia. Am I Med
146. DiGiulio S, Boulu R, Drueke T, Nicolai A, Zingraff J, 57:551-60,1974
Crosnier J: Clofibrate treatment of hyperlipidemia in 156. Abbott WGH, Lillioja S, Young AA, Zawadzki JK, Yki-
chronic renal failure. Clin Nephrol 8:504-509, 1977 Jarvinen H, Christin L, Howard BV: Relationship be-
147. Pasternack A, Vanttinen T, Solakivi T, Kuusi T, Korte T: tween plasma lipoprotein concentrations and insulin ac-
Normalization of lipoprotein lipase and hepatic lipase tion in an obese hyperinsulinemic population. Diabetes
by gemfibrozil results in correction of lipoprotein ab- 36:897-904, 1987
normalities in chronic renal failure. Clin Nephrol 27:163- 157. Garg A, Helderman JH, Koffler M, Ayuso R, Rosenstock
68, 1987 J, Raskin P: Relationship between lipoprotein levels and
148. SosenkoJM, BreslowJL, Miettinen OS, Gabbay KH: Hy- in vivo insulin action in normal young white men. Me-
perglycemia and plasma lipid levels: a prospective study tabolism 37:982-87, 1988
of young insulin-dependent diabetic patients. N Engl ] 158. The Lipid Research Clinics Population Studies Data Book:
Med 302:650-54, 1980 The Prevalence Study. Aggregate Distribution of Lip-
149. Bagdade JD, Porte D Jr, Bierman EL: Diabetic lipemia: ids, Lipoproteins and Selected Variables in 11 North
a form of acquired fat-induced lipemia. N Engl) Med American Populations. Washington, DC, U.S. Dept. of
276:427-33, 1978 Health and Human Services, 1980 (NIH publ. no. 80-
150. Fuller JH, Shipley MJ, Rose G, Jarrett RJ, Keen H: Mor- 1527)
DIABETES CARE, VOL. 13, N O . 2, FEBRUARY 1990 169
Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Cardiovascular Disease Trends in IndiaDokumen24 halamanCardiovascular Disease Trends in IndiaWahyuningsih HamidBelum ada peringkat
- Management of Dyslipidemia in Adults With DiabetesDokumen19 halamanManagement of Dyslipidemia in Adults With DiabetesWahyuningsih HamidBelum ada peringkat
- 2A17882Fd01 PDFDokumen5 halaman2A17882Fd01 PDFWahyuningsih HamidBelum ada peringkat
- The Beneficial Effects of Tree Nuts On The Aging Brain: Amanda N. Carey, Shibu M. Poulose and Barbara Shukitt-HaleDokumen13 halamanThe Beneficial Effects of Tree Nuts On The Aging Brain: Amanda N. Carey, Shibu M. Poulose and Barbara Shukitt-HaleWahyuningsih HamidBelum ada peringkat
- Dislipidemia Dan CardiovasculerDokumen2 halamanDislipidemia Dan CardiovasculerWahyuningsih HamidBelum ada peringkat
- 8 Vol. 4, Issue 2, Feb 2013, IJPSR, RE-821, Paper 8Dokumen7 halaman8 Vol. 4, Issue 2, Feb 2013, IJPSR, RE-821, Paper 8Wahyuningsih HamidBelum ada peringkat
- Dislipid 2 PDFDokumen4 halamanDislipid 2 PDFWahyuningsih HamidBelum ada peringkat
- Dislipidemia Dan DiabetesDokumen11 halamanDislipidemia Dan DiabetesWahyuningsih HamidBelum ada peringkat
- Phytosterols: Natural Compounds With Established and Emerging Health BenefitsDokumen8 halamanPhytosterols: Natural Compounds With Established and Emerging Health BenefitsWahyuningsih HamidBelum ada peringkat
- Peanut Consumption and Cardiovascular RiskDokumen6 halamanPeanut Consumption and Cardiovascular RiskWahyuningsih HamidBelum ada peringkat
- Public Health NutritionFirstView Articles717516Dokumen18 halamanPublic Health NutritionFirstView Articles717516Wahyuningsih HamidBelum ada peringkat
- Humans Phytosterol Glycosides Reduce Cholesterol Absorption inDokumen6 halamanHumans Phytosterol Glycosides Reduce Cholesterol Absorption inWahyuningsih HamidBelum ada peringkat
- Eating Behavior Correlates of Adult Weight Gain and Obesity in Healthy Women Aged 55-65 yDokumen8 halamanEating Behavior Correlates of Adult Weight Gain and Obesity in Healthy Women Aged 55-65 yWahyuningsih HamidBelum ada peringkat
- Peanuts PDFDokumen4 halamanPeanuts PDFWahyuningsih HamidBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Yes We CanDokumen3 halamanYes We CanSpeech & Language Therapy in PracticeBelum ada peringkat
- World Persp 2008 - FinalDokumen248 halamanWorld Persp 2008 - FinalBuğra EgeliBelum ada peringkat
- PharmacyDokumen223 halamanPharmacyYamchi ArnavazBelum ada peringkat
- Review: Curar, Persuadir, Gobernar: La Construcción Histórica de La Profesión Médica en Buenos Aires (1852-1886), by R. González LeandriDokumen2 halamanReview: Curar, Persuadir, Gobernar: La Construcción Histórica de La Profesión Médica en Buenos Aires (1852-1886), by R. González LeandriXoyyo Xoyyodevuelta0% (1)
- Pharmacological and Parenteral TherapiesDokumen99 halamanPharmacological and Parenteral TherapieslBelum ada peringkat
- Tissue Salts CombinationsDokumen12 halamanTissue Salts Combinationsherbacija9213100% (2)
- Roche Chemstrip 2 Insert Instruction SheetDokumen2 halamanRoche Chemstrip 2 Insert Instruction SheetEveyBelum ada peringkat
- Learning Module 4 Layers Bio-Security, Vaccination and Cleaning Poultry HousesDokumen30 halamanLearning Module 4 Layers Bio-Security, Vaccination and Cleaning Poultry HousesTshegofatsoBelum ada peringkat
- Lesson 3Dokumen6 halamanLesson 3api-316910625Belum ada peringkat
- RA 8203 - Special Law On Counterfeit DrugsDokumen13 halamanRA 8203 - Special Law On Counterfeit DrugsYuzu SakuraBelum ada peringkat
- NauliDokumen2 halamanNauliGurjit Singh BoparaiBelum ada peringkat
- Arguments: THW Ban Miss UniverseDokumen3 halamanArguments: THW Ban Miss UniverseGen eralBelum ada peringkat
- PBL 5 ObjectivesDokumen7 halamanPBL 5 ObjectivesHugh JacobsBelum ada peringkat
- Case Analysis PaperDokumen2 halamanCase Analysis PaperKukugirl DavisBelum ada peringkat
- Health Department of Indonesia: Puskesmas Cibulan Jalan Raya Puncak KM.81 Bogor Telp. 0251 053053Dokumen2 halamanHealth Department of Indonesia: Puskesmas Cibulan Jalan Raya Puncak KM.81 Bogor Telp. 0251 053053Ribka RisnawatiBelum ada peringkat
- 1272 PDFDokumen4 halaman1272 PDFsBelum ada peringkat
- Zero B Product PresentationDokumen27 halamanZero B Product PresentationKalyan DeshpandeBelum ada peringkat
- Drug Interactions Results - MICROMEDEXDokumen5 halamanDrug Interactions Results - MICROMEDEXAna SibajaBelum ada peringkat
- Social Responsibility of Business and Business Ethics: 2.1 IntroductionDokumen25 halamanSocial Responsibility of Business and Business Ethics: 2.1 IntroductionimadBelum ada peringkat
- Original PDF Kendigs Disorders of The Respiratory Tract in Children 9th Edition PDFDokumen41 halamanOriginal PDF Kendigs Disorders of The Respiratory Tract in Children 9th Edition PDFmichael.richardson540100% (30)
- Sensors 22 08161 v2Dokumen20 halamanSensors 22 08161 v2Kristian DokicBelum ada peringkat
- Lockout/Tagout (Loto) Checklist: 1. Scope of WorkDokumen3 halamanLockout/Tagout (Loto) Checklist: 1. Scope of WorkPutri UnaBelum ada peringkat
- Fiscal Year 2014 BUDGET of The United States GovernmentDokumen244 halamanFiscal Year 2014 BUDGET of The United States GovernmentAlex Tango FuegoBelum ada peringkat
- LP U1209300 Inoa 2013 Inoa Color ChartDokumen4 halamanLP U1209300 Inoa 2013 Inoa Color ChartbinreBelum ada peringkat
- Business Spotlight Fit For WorkDokumen7 halamanBusiness Spotlight Fit For WorkMrs PlentiBelum ada peringkat
- WECOC Final Announcement 29th CompressedDokumen32 halamanWECOC Final Announcement 29th CompressedChristabella Natalia WijayaBelum ada peringkat
- Primary Open Rhinoplasty: Preoperative Assessment and PlanningDokumen16 halamanPrimary Open Rhinoplasty: Preoperative Assessment and PlanningМаратBelum ada peringkat
- Provisional Mop Up Selection List For Neet PG CPS 2021Dokumen47 halamanProvisional Mop Up Selection List For Neet PG CPS 2021Rikesh K MhatreBelum ada peringkat
- Body ReadingDokumen1 halamanBody Readingpradeep6288Belum ada peringkat
- Middle Meatal AntrostomyDokumen2 halamanMiddle Meatal AntrostomymajidjankakakhelBelum ada peringkat