Anda mungkin juga menyukai
- Radiation Dermatitis ManagementDokumen11 halamanRadiation Dermatitis ManagementAdonanBelum ada peringkat
- 9475-Jurnal Keperawatan Terapan Vol 2 No 2 September 2016 Pengaruh Batik EfektifDokumen8 halaman9475-Jurnal Keperawatan Terapan Vol 2 No 2 September 2016 Pengaruh Batik EfektifNYONGKERBelum ada peringkat
- Symptom Management Guidelines: Care of Malignant WoundsDokumen7 halamanSymptom Management Guidelines: Care of Malignant WoundsPatrico Rillah Setiawan100% (1)
- Disorders of Pigmentations: Vitiligo, Melasma and Other ConditionsDokumen76 halamanDisorders of Pigmentations: Vitiligo, Melasma and Other ConditionsJeremy HermantoBelum ada peringkat
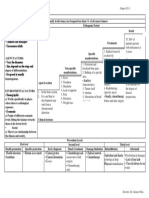
- Fibro PathwayDokumen2 halamanFibro Pathwayapi-163168129Belum ada peringkat
- (DERMA) Revalida Review 2018Dokumen202 halaman(DERMA) Revalida Review 2018anonymousBelum ada peringkat
- CPWSC - TOWA - Brochure - 210x210 - No MarksDokumen24 halamanCPWSC - TOWA - Brochure - 210x210 - No MarksKlinik KitamuraBelum ada peringkat
- Smart antibiotic use in children with serious bacterial infectionsDokumen44 halamanSmart antibiotic use in children with serious bacterial infectionsAlbertBelum ada peringkat
- Derm LOsDokumen37 halamanDerm LOskatherine nunnBelum ada peringkat
- Fungal Infections: Major Predisposing FactorsDokumen6 halamanFungal Infections: Major Predisposing FactorsIsabel CastilloBelum ada peringkat
- DrugStudy - 01 02 24Dokumen3 halamanDrugStudy - 01 02 24Laurente, Patrizja Ysabel B. BSN-2DBelum ada peringkat
- Serious Pathology Guide FINALDokumen25 halamanSerious Pathology Guide FINALFirmansyah PurwantoBelum ada peringkat
- Symptom Management Guidelines: XEROSTOMIADokumen9 halamanSymptom Management Guidelines: XEROSTOMIAالعمري العمريBelum ada peringkat
- NCM 101 HEALTH ASSESSMENT Powerpoint1Dokumen23 halamanNCM 101 HEALTH ASSESSMENT Powerpoint1John TacordaJrBelum ada peringkat
- Patient's ExaminationDokumen50 halamanPatient's Examination蔡長家Belum ada peringkat
- Atopic Dermatitis, Allergic Rhinits, and Asthma: Tracie Kirkland, DNP, RN, ANP-BC, CPNPDokumen19 halamanAtopic Dermatitis, Allergic Rhinits, and Asthma: Tracie Kirkland, DNP, RN, ANP-BC, CPNPNick flemmingBelum ada peringkat
- KULKEL Atopic DermatitisDokumen34 halamanKULKEL Atopic Dermatitisirhamni istiqomahBelum ada peringkat
- EMERGENCY SKIN DISORDERS 2021 Lecture - dr NanaDokumen33 halamanEMERGENCY SKIN DISORDERS 2021 Lecture - dr Nanawilliam atmadjiBelum ada peringkat
- Managing Emergencies in Palliative & Geriatric CareDokumen47 halamanManaging Emergencies in Palliative & Geriatric CareprashantBelum ada peringkat
- Malignant Wounds Assessment and Management Algorithm: Treat Patient/Family ConcernsDokumen67 halamanMalignant Wounds Assessment and Management Algorithm: Treat Patient/Family ConcernsWisnuardhyHendrawardhanaBelum ada peringkat
- Dermatology in 2hrsDokumen222 halamanDermatology in 2hrslarisaP100% (4)
- Emergency Dermatology: Case 1, Question 1 The Most Likely Diagnosis Is: Case 1, Question 1 The Most Likely Diagnosis IsDokumen16 halamanEmergency Dermatology: Case 1, Question 1 The Most Likely Diagnosis Is: Case 1, Question 1 The Most Likely Diagnosis IskarbikashBelum ada peringkat
- Skin Lesions and DiagnosisDokumen25 halamanSkin Lesions and DiagnosisBUCM Class 2023Belum ada peringkat
- Concept MapDokumen1 halamanConcept MapSheryl Ann Barit PedinesBelum ada peringkat
- Assessing Skin, Face, Eyes, Ears, Nose, Mouth and NeckDokumen20 halamanAssessing Skin, Face, Eyes, Ears, Nose, Mouth and NeckEUREKA PEARL PAIRATBelum ada peringkat
- Scabies - Other Parasitic InfestationsDokumen54 halamanScabies - Other Parasitic InfestationsRaziHashmiBelum ada peringkat
- BurnsDokumen33 halamanBurnscoco brillqnteBelum ada peringkat
- Cancer Rehabilitation Goals and Treatment EffectsDokumen4 halamanCancer Rehabilitation Goals and Treatment EffectsJia MedinaBelum ada peringkat
- Skin and BurnDokumen52 halamanSkin and Burniifatmax20Belum ada peringkat
- Dermis Medical Students Dermatology Revision Lecture 2018: Topic A - Inflammation and InfectionDokumen10 halamanDermis Medical Students Dermatology Revision Lecture 2018: Topic A - Inflammation and InfectionBradley JacksonBelum ada peringkat
- Symptom Management Guidelines: Dyspnea: Dyspnea: A Disorder Characterized by Difficulty BreathingDokumen8 halamanSymptom Management Guidelines: Dyspnea: Dyspnea: A Disorder Characterized by Difficulty Breathingmia fitryniBelum ada peringkat
- HANDOUTS-CD-MR.-BALANONDokumen8 halamanHANDOUTS-CD-MR.-BALANONz6cc9vgg6nBelum ada peringkat
- Psoriasis Dermatitis FinalDokumen50 halamanPsoriasis Dermatitis Finalapi-546809761Belum ada peringkat
- Lelovas P 2023 Recognition of Abnormal Behaviour, Discomfort, PainDokumen28 halamanLelovas P 2023 Recognition of Abnormal Behaviour, Discomfort, PainDimitris AnestisBelum ada peringkat
- Pharm 1290 StudyguideDokumen20 halamanPharm 1290 StudyguideKayla Nicole BrillaBelum ada peringkat
- Leilani O. Estacio, Man RN: Chemotherapeutic Agents, Antibiotics, Immunosuppressive DrugsDokumen42 halamanLeilani O. Estacio, Man RN: Chemotherapeutic Agents, Antibiotics, Immunosuppressive DrugsHERLIN HOBAYANBelum ada peringkat
- Allergic Rhinitis PathoDokumen3 halamanAllergic Rhinitis PathoAce FabrigasBelum ada peringkat
- Historia Natural Ingles MasachaDokumen1 halamanHistoria Natural Ingles MasachaSalma LopezBelum ada peringkat
- Shanz - PEDIA II 2.01 NEWDokumen8 halamanShanz - PEDIA II 2.01 NEWPetrina XuBelum ada peringkat
- Joice Das - Pain Management in BurnsDokumen21 halamanJoice Das - Pain Management in BurnsJoice DasBelum ada peringkat
- DM Foot 81Dokumen20 halamanDM Foot 81Zar Ni OoBelum ada peringkat
- Immunology TA v.01 Paramita Mycomments v.01Dokumen80 halamanImmunology TA v.01 Paramita Mycomments v.01Miral Sandipbhai MehtaBelum ada peringkat
- Case Report Tinea Corporis: By: Nurul Ayni Supervisor: Irma Tarida L, Dr. SP - KKDokumen22 halamanCase Report Tinea Corporis: By: Nurul Ayni Supervisor: Irma Tarida L, Dr. SP - KKnurulayniBelum ada peringkat
- LRR DERMATDokumen190 halamanLRR DERMATpdivyashreerajBelum ada peringkat
- OTC Course: Zienab Halem SCUDokumen4 halamanOTC Course: Zienab Halem SCUHAMIDBelum ada peringkat
- Antineoplastic Drug Administration Intravenous Skill Oncology COVID 19 Toolkit 140420Dokumen15 halamanAntineoplastic Drug Administration Intravenous Skill Oncology COVID 19 Toolkit 140420diah fitriyaniBelum ada peringkat
- Drug Eruptions 2 Medical Students-1Dokumen24 halamanDrug Eruptions 2 Medical Students-1Abdelmouez AnwerBelum ada peringkat
- JJJJJDokumen6 halamanJJJJJRhani AzhraaBelum ada peringkat
- Cellular Regulation Student VersionDokumen15 halamanCellular Regulation Student VersionCruz YrBelum ada peringkat
- P E R S O N S: School of Health SciencesDokumen11 halamanP E R S O N S: School of Health SciencesContented LinganBelum ada peringkat
- Stockwell - The Red Eye ExpressDokumen31 halamanStockwell - The Red Eye ExpressSiti HaniwidiyaBelum ada peringkat
- Management of Cancer PatientsDokumen10 halamanManagement of Cancer Patientswieka mawieBelum ada peringkat
- Corneal Disease and Dystrophy Management PDFDokumen53 halamanCorneal Disease and Dystrophy Management PDFScerbatiuc CristinaBelum ada peringkat
- 2 Patient Assessment Pocket DentistryDokumen1 halaman2 Patient Assessment Pocket DentistryVictor FanBelum ada peringkat
- Natural PhototherapyDokumen77 halamanNatural PhototherapyLeo FluxBelum ada peringkat
- Dr. J.T. Kent's Evalution Order of SymptomsDokumen1 halamanDr. J.T. Kent's Evalution Order of Symptomsvidhipatel1601Belum ada peringkat
- Assessment of The BreastDokumen14 halamanAssessment of The BreastArlyn MendenillaBelum ada peringkat
- Perio Lecture 3Dokumen69 halamanPerio Lecture 3Roisin TangBelum ada peringkat
- Your Emotional Type: Key to the Therapies That Will Work for YouDari EverandYour Emotional Type: Key to the Therapies That Will Work for YouPenilaian: 1 dari 5 bintang1/5 (1)
- Low Dose Ketamin: Keyword: Cite This ArticleDokumen7 halamanLow Dose Ketamin: Keyword: Cite This ArticleDevana MaelissaBelum ada peringkat
- Spaide 2019Dokumen15 halamanSpaide 2019Devana MaelissaBelum ada peringkat
- Ipd 1Dokumen16 halamanIpd 1Devana MaelissaBelum ada peringkat
- Ipd 1Dokumen16 halamanIpd 1Devana MaelissaBelum ada peringkat
- 5 - OA-Medhat-Inj Pain PDFDokumen4 halaman5 - OA-Medhat-Inj Pain PDFDevana MaelissaBelum ada peringkat
- Post-Operative Pain: Mechanisms and ManagementDokumen6 halamanPost-Operative Pain: Mechanisms and ManagementDevana MaelissaBelum ada peringkat
- Post-Operative Pain: Mechanisms and ManagementDokumen6 halamanPost-Operative Pain: Mechanisms and ManagementDevana MaelissaBelum ada peringkat
- 566-Article Text-1105-1-10-20190208Dokumen6 halaman566-Article Text-1105-1-10-20190208Devana MaelissaBelum ada peringkat
- 566-Article Text-1105-1-10-20190208Dokumen6 halaman566-Article Text-1105-1-10-20190208Devana MaelissaBelum ada peringkat
- JURNAL BEDAH DR - Ubay SP.B PDFDokumen4 halamanJURNAL BEDAH DR - Ubay SP.B PDFDevana MaelissaBelum ada peringkat
- Dr. Ajit K VarmaDokumen36 halamanDr. Ajit K VarmaDevana MaelissaBelum ada peringkat
- Dr. Peni KusumastutiDokumen80 halamanDr. Peni KusumastutiDevana MaelissaBelum ada peringkat
- 8650 Status Ginekologi-1Dokumen6 halaman8650 Status Ginekologi-1Devana MaelissaBelum ada peringkat
- Critical Journal CareDokumen7 halamanCritical Journal CareMuhammadKadafiBelum ada peringkat
- Endophthalmitis, Prevention and TreatmentDokumen20 halamanEndophthalmitis, Prevention and TreatmentIan TombokanBelum ada peringkat
- Tri PPT Bels PalsyDokumen29 halamanTri PPT Bels PalsyTrii Asih FatubunBelum ada peringkat
- JURNAL BEDAH DR - Ubay SP.B PDFDokumen4 halamanJURNAL BEDAH DR - Ubay SP.B PDFDevana MaelissaBelum ada peringkat
- 191 Prevalence of Pterygium in A Rural Community of Meskan DDokumen4 halaman191 Prevalence of Pterygium in A Rural Community of Meskan DDevana MaelissaBelum ada peringkat
- JURNAL BEDAH DR - Ubay SP.B PDFDokumen4 halamanJURNAL BEDAH DR - Ubay SP.B PDFDevana MaelissaBelum ada peringkat
- Workshop Rs Sistem Monitoring Dengan Skoring PDFDokumen26 halamanWorkshop Rs Sistem Monitoring Dengan Skoring PDFSukriadiBelum ada peringkat
- 5 - OA-Medhat-Inj Pain PDFDokumen4 halaman5 - OA-Medhat-Inj Pain PDFDevana MaelissaBelum ada peringkat
- Acneiform Rash PDFDokumen5 halamanAcneiform Rash PDFDevana MaelissaBelum ada peringkat
- 1 Prosedur Pemeriksaan Radiologi Untuk Mendeteksi Kelainan Dan Cedera Tulang BelakangDokumen4 halaman1 Prosedur Pemeriksaan Radiologi Untuk Mendeteksi Kelainan Dan Cedera Tulang BelakangShofi Dhia AiniBelum ada peringkat
- Rap Sang 2014Dokumen10 halamanRap Sang 2014Devana MaelissaBelum ada peringkat
- PCP v5n4p289 enDokumen8 halamanPCP v5n4p289 enDevana MaelissaBelum ada peringkat
- Critical Journal CareDokumen7 halamanCritical Journal CareMuhammadKadafiBelum ada peringkat
- Function of Professional Scuba DiversDokumen5 halamanFunction of Professional Scuba DiversDevana MaelissaBelum ada peringkat
- Jurnal Kulit JerawatDokumen13 halamanJurnal Kulit JerawatDevana MaelissaBelum ada peringkat
- CD NCLEX NOTES-Infection ControlDokumen1 halamanCD NCLEX NOTES-Infection ControlrenchiecaingletBelum ada peringkat
- Patogenesis Infeksi BakteriDokumen47 halamanPatogenesis Infeksi BakteribellabelbonBelum ada peringkat
- VILSAN CatalougeDokumen97 halamanVILSAN CatalougeSầu VeBelum ada peringkat
- Visitation-Guidelines 10.9.20 FINALDokumen5 halamanVisitation-Guidelines 10.9.20 FINALWIS Digital News StaffBelum ada peringkat
- Natural Tea Give Health Benefits (A3 Size)Dokumen8 halamanNatural Tea Give Health Benefits (A3 Size)itsjai1303m80Belum ada peringkat
- Caiazza, Toole - 2003 PDFDokumen4 halamanCaiazza, Toole - 2003 PDFNICOLÁS SEBASTÍAN GOMEZ SEQUEDABelum ada peringkat
- Application For An Establishment License - To Be Completed by Operator of EstablishmentDokumen6 halamanApplication For An Establishment License - To Be Completed by Operator of EstablishmentDonteBelum ada peringkat
- Treatment of Rheumatoid Arthritis in Patients With Concomitant Chronic Hepatitis C InfectionDokumen24 halamanTreatment of Rheumatoid Arthritis in Patients With Concomitant Chronic Hepatitis C InfectionMuhammad Farras Razin PerdanaBelum ada peringkat
- Alopecia Totalis Following HFMDDokumen3 halamanAlopecia Totalis Following HFMDVilt VilBelum ada peringkat
- Cryptococcosis: Dr.C.Meenakshisundaram.Dokumen16 halamanCryptococcosis: Dr.C.Meenakshisundaram.Meenakshisundaram CBelum ada peringkat
- Hiv 101-2018Dokumen47 halamanHiv 101-2018Alvin QuiranteBelum ada peringkat
- MEDT02 Lesson 2 - Safety in PhlebotomyDokumen5 halamanMEDT02 Lesson 2 - Safety in PhlebotomySHELDY AGONCILLOBelum ada peringkat
- BC-6800 Auto Hematology Analyzer Small Cube, Big DifferenceDokumen16 halamanBC-6800 Auto Hematology Analyzer Small Cube, Big DifferencePieter Du Toit-EnslinBelum ada peringkat
- The Big Red Book of Spanish Vocabulary - Thomas, ScottDokumen3.136 halamanThe Big Red Book of Spanish Vocabulary - Thomas, ScottAshlie Cui100% (8)
- NEENA KHANNA'S DermatologyDokumen465 halamanNEENA KHANNA'S Dermatologybrij bhushan kumar75% (16)
- TLE 9-10 Nail Care M6 For PrintingDokumen22 halamanTLE 9-10 Nail Care M6 For Printingveronica relenteBelum ada peringkat
- KKM Policies & Procedures On Infection Prevention and Control 2019Dokumen305 halamanKKM Policies & Procedures On Infection Prevention and Control 2019Noor AtiqahBelum ada peringkat
- Test Bank Current Medical Diagnosis and Treatment 2020 PapadakisDokumen15 halamanTest Bank Current Medical Diagnosis and Treatment 2020 Papadakisguadaluperomerojz6s100% (12)
- Hiv ProphylaxisDokumen193 halamanHiv ProphylaxisKiran MishraBelum ada peringkat
- Week 13 NCMB 312 Lect NotesDokumen18 halamanWeek 13 NCMB 312 Lect NotesAngie BaylonBelum ada peringkat
- The Fungi of Medical ImportanceDokumen74 halamanThe Fungi of Medical ImportancenrahmaBelum ada peringkat
- Nursing Seminar 1 SAS Session 17Dokumen8 halamanNursing Seminar 1 SAS Session 17ZiaBelum ada peringkat
- Periorbital and Orbital CellulitisDokumen10 halamanPeriorbital and Orbital CellulitisValéria DuarteBelum ada peringkat
- Reflective Journal (HDU)Dokumen2 halamanReflective Journal (HDU)Wench Ryechelle SodosoBelum ada peringkat
- Standard Operating Procedure for Eye CultureDokumen2 halamanStandard Operating Procedure for Eye CultureSemeeeJuniorBelum ada peringkat
- Inventing The AIDS VirusDokumen724 halamanInventing The AIDS VirusMartin Barrett100% (11)
- Septic Shock Nursing Assessment and ManagementDokumen6 halamanSeptic Shock Nursing Assessment and ManagementJenn GallowayBelum ada peringkat
- Tetracycline SDokumen51 halamanTetracycline SPapaindoBelum ada peringkat
- Hubungan Mikroorganisme Dengan SanitasiDokumen31 halamanHubungan Mikroorganisme Dengan SanitasiAlbar PervectBelum ada peringkat
- 2 Environmental EpidemiologyDokumen33 halaman2 Environmental EpidemiologyRatna Ismail80% (5)